

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fixation of pedicle screws during spinal surgery using a robotic system (Renaissance™, Mazor Robotics, Caesarea, Israel) is highly accurate.123456 However, one report has indicated that robot-assisted surgery does not provide superior outcomes over conventional surgery.7 Furthermore, a recent meta-analysis revealed no significant advantage in using the robot-assisted pedicle screw insertion technique, compared to the conventional technique.8
We recently performed a radiographic analysis of robot-assisted pedicle screw insertion, and found that this approach decreased proximal facet joint violations, increased screw positioning accuracy, and provided less hazardous orientations.9 Additionally, we performed a biomechanical finite element analysis, which revealed that robot-assisted screw fixation provided biomechanical superiority in terms of alleviating contact force on adjacent segment facets and disc pressure.10 However, the radiographic outcomes [e.g., adjacent segment degeneration (ASD)] and clinical outcomes of robot-assisted surgery have not been evaluated. Therefore, the present study was undertaken to prospectively assess early radiographic and clinical outcomes of robot-assisted pedicle screw insertion after a minimum follow-up of 2 years in comparison to those of the conventional freehand pedicle insertion technique.
MATERIALS AND METHODS
Study design and patient population
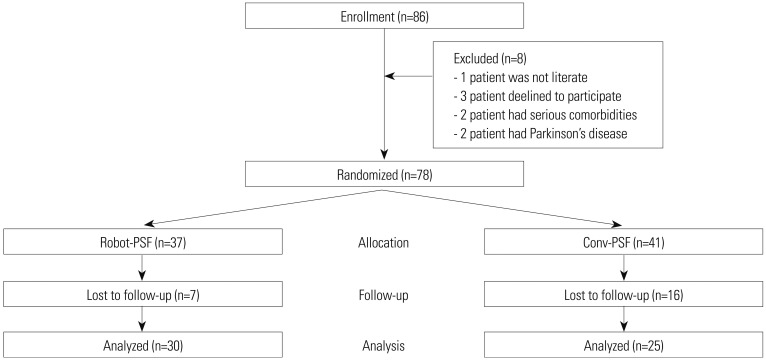
This study's observational cohort protocol was approved by our center's Institutional Review Board, and all participants provided written informed consent before enrollment in an earlier randomized controlled single-center trial (IRB No.: E-1310/222-001). In that trial, participants were randomly assigned 1:1 to undergo robot-assisted pedicle screw fixation (Robot-PSF) or fusion using the conventional freehand pedicle screw fixation (Conv-PSF). All procedures were performed by a single experienced spine surgeon at a single site between December 2013 and October 2014. The trial was registered with ClinicalTrials.gov (NCT02121249), and its design has been previously described.9 The trial enrolled a total of 78 patients who were randomly assigned to the Robot-PSF group (37 patients) or the Conv-PSF (41 patients). However, seven patients in the Robot-PSF group and 16 patients in the Conv-PSF group were lost to follow-up. Thus, the present study evaluated radiographic ASD and clinical outcomes from 55 patients (30 patients in the Robot-PSF group and 25 patients in the Conv-PSF group) (Fig. 1).
Surgical technique
The Robot-PSF group underwent thin-slice computed tomography (CT), which was used to define the pedicle screw trajectories, insertion points, and screw sizes. Posterior interbody fusion was performed using the minimal invasive technique.11 The Renaissance Surgical Guidance Robot (Mazor Robotics) was placed on a mounting platform, which was attached with a clamp to the patient's spinous process or was fixed to the bed rails, and connected using a 2.5-mm surgical pin to a proximal adjacent spinous process. A radiographic marker was placed on the mounting platform before two fluoroscopic images were obtained. These fluoroscopic images were automatically fitted with the pre-planned CT; the robot was placed on the mounting platform; and then, the robot was moved to the preplanned trajectory. The robot's drilling guide was used to insert pedicle screws (Sextant; Medtronic Inc., Minneapolis, MN, USA) using the percutaneous technique over guidewires. The detailed surgical procedures have been described in our previous report.12
In the Conv-PSF group, a midline longitudinal incision was used to expose the spine to the lateral tips of the transverse processes and clearly identify bony landmarks. Pedicle screws were inserted using the conventional freehand technique and the Weinstein method.13 Portable radiography was used to verify the instrumentation placement after screw insertion. Interbody fusion in both groups was performed using autologous laminar bone from the decompression and polyether ether ketone cages on both sides.
Data collection
The incidence of radiographic ASD was determined using radiographic parameters on simple lateral radiographs during regular follow-up. Radiographic measurements of the proximal adjacent segment were performed using a Picture Archiving and Communications System (INFINITT Healthcare Co. Ltd, Phillipsburg, NJ, USA). Preoperative proximal adjacent disc degeneration was measured using a T2-weighted midsagittal image and Pfirrmann classification.14 Disc degeneration was also measured using plain radiographs during the follow- up using the University of California at Los Angeles (UCLA) disc degeneration grading, which grades degeneration based on disc height decrease, osteophyte formation, and endplate sclerosis.1516 The intervertebral disc height was defined as the distance between the upper and lower endplates, perpendicular from the mid-point of a bisecting line drawn between the anterior and posterior disc heights.17 Angular motion of the proximal adjacent segment was calculated using the difference between the disc angle values, which are formed between the line of the upper vertebra's inferior endplate and the lower vertebra's upper endplate, based on flexion and extension lateral radiographs. Vertebral body translation was measured using the shift of the superior vertebra relative to the inferior vertebra. Radiographic ASD was diagnosed based on a development or increase of >4 mm in vertebral translation, angular motion of >10° on dynamic radiographs, >10% loss of disc height, or deterioration of UCLA grade ≥1 versus the preoperative radiographic parameters.151819
Preoperative baseline data were collected by independent research personnel who interviewed the participants and collected their questionnaire answers, including visual analogue scale (VAS) and Oswestry disability index (ODI) scores. The VAS for back pain and leg pain comprised a 10-cm line with “none” (0) on one end of the scale and “disabling pain” (10) on the other end. The ODI is based on a self-administered questionnaire that measures “back-specific function” using 10 items, with six responses for each item. Each item is scored from 0 to 5, and the total score is subsequently converted to a 0–100 scale, with higher scores indicating more severe symptoms.20 The VAS and ODI scores were evaluated at 3, 6, 12, and 24 months after surgery.
Statistical analysis
The primary analyses were based on the intention-to-treat principle, and included patients who had undergone their assigned surgery and were followed-up for ≥2 years. Continuous variables are reported as means±standard deviations. Differences between the two groups were analyzed using the independent t-test (continuous variables) or chi-square test (categorical variables). Intra-group and inter-group changes in clinical outcomes (back VAS, leg VAS, and ODI) were analyzed using a linear mixed model for longitudinal data, which handled missing data. Measurement reliability was evaluated using an intra-class correlation coefficient [ICC (3,1)] with absolute agreement to assess the radiographic measurements. Intra-observer reliability for the radiographic parameters was evaluated in two measurement sessions at an interval of 8 weeks. The reliability results were reported as ICC values and 95% confidence intervals (CIs), with an ICC value of >0.75 considered excellent, 0.40-0.75 considered fair to good, and <0.40 considered poor. Statistical analysis was performed using IBM SPSS software (version 20.0; IBM Corp., Armonk, NY, USA) and STATA software (version 15.0; Stata Corporation, College Station, TX, USA). Differences were considered statistically significant at a p value <0.05.
RESULTS
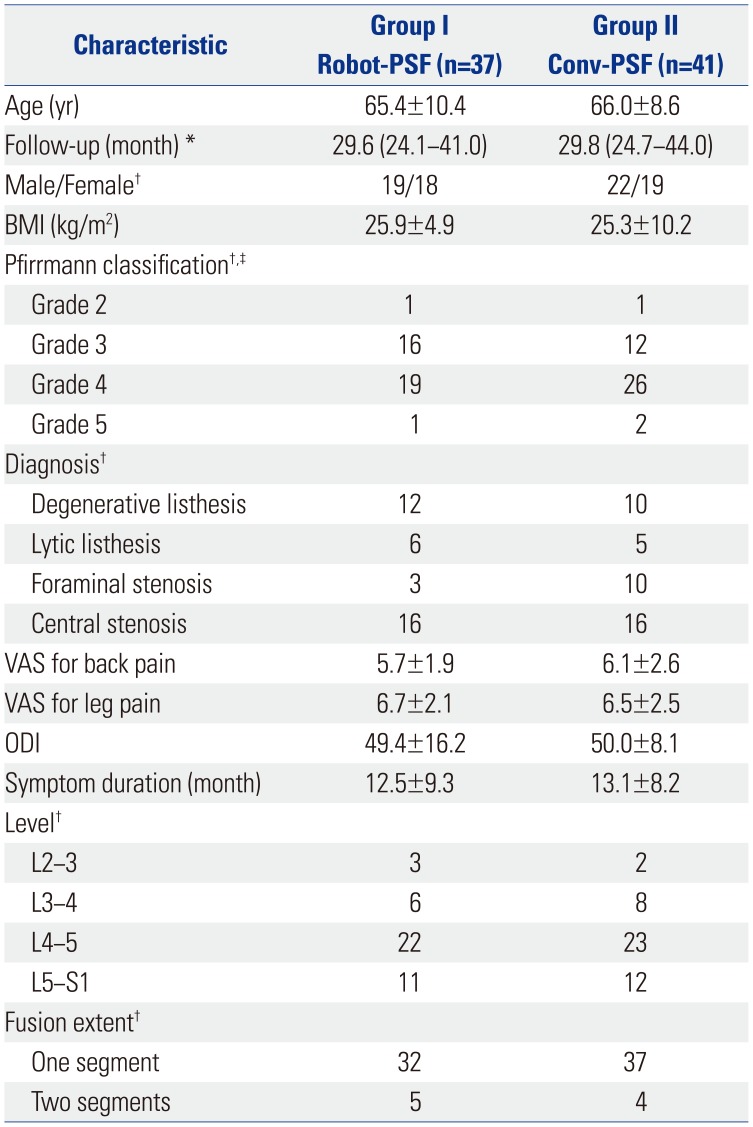
Between December 2013 and October 2014, the original trial enrolled 81 patients. The Robot-PSF group included 39 patients, although two patients subsequently did not receive their assigned treatment and were excluded. Among the 42 patients who were assigned to the Conv-PSF group, one patient withdrew from the trial. Thus, 37 patients completed the Robot-PSF procedure and 41 patients completed the Conv-PSF procedure. Two patients in the Robot-PSF group and four patients in the Conv-PSF group did not attend their 1-year follow-up, and a total of seven patients in the Robot-PSF group and 16 patients in the Conv-PSF group did not attend their 2-year follow-up. Therefore, the radiographic ASD and clinical outcomes were evaluated for 55 patients (30 patients in the Robot-PSF group and 25 patients in the Conv-PSF group). There were no significant differences in the two groups' preoperative demographic, clinical, and radiographic parameters (all p>0.05) (Table 1). The Robot-PSF group included 12 men and 18 women who had a mean age of 63 years (range: 34–80 years). The Conv-PSF group included 14 men and 11 women who had a mean age of 66.3 years (range: 53–77 years).
The 55 patients completed a minimum follow-up of 24 months (range: 24.1–44 months). No significant inter-group differences were observed in the radiographic ASD parameters, including UCLA grade, vertebral translation, angular motion, and loss of disc height (p=0.320). Table 2 shows the detailed results for radiographic ASD. The ICC for intra-observer reliability was 0.891 (95% CI: 0.858–0.924), which indicated excellent agreement.
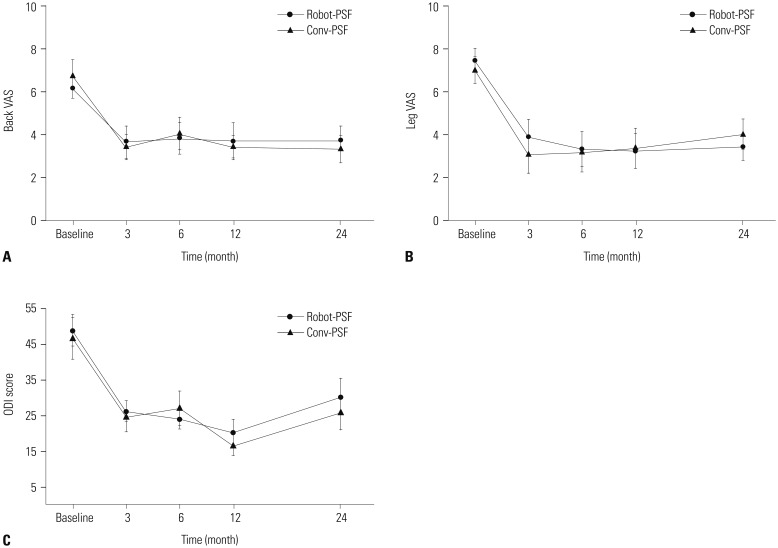
Both groups experienced significant improvement in their back VAS and leg VAS scores at the final follow-up (both p<0.001), although the inter-group differences at the final follow-up were not significant for back VAS (p=0.876) and leg VAS (p=0.429) (Fig. 2A and B). The ODI scores also significantly improved within each group at the final follow-up (p<0.001), although the inter-group difference was also not significant (p=0.952) (Fig. 2C). The back VAS, leg VAS, and ODI scores improved significantly in each group over time (p<0.001 for all variables at each follow-up compared to baseline), although significant intra-group increases in ODI score were observed at 24-month follow-up, compared to 12-month follow-up (p=0.012) (Fig. 2C).
Revision surgery was required for two of the 25 patients (8%) in the Conv-PSF group. Therein, revision surgery was performed after 15 months and 44 months at the proximal segment adjacent to the first fusion surgery (Fig. 3). No revision surgery was required in the Robot-PSF group.
DISCUSSION
The present study examined radiographic ASD and clinical outcomes from robot-assisted and conventional freehand pedicle screw fixation during posterior lumbar interbody fusion after at least 2 years. The results indicated that both techniques provide similar outcomes in terms of radiographic ASD at the proximal adjacent segment. Furthermore, there were no significant inter-group differences in improvements in back VAS, leg VAS, and ODI scores. However, two patients in the Conv-PSF group (8%) required revision surgery.
The major advantage of the robot-assisted technique is in the guidance of screw fixation at a precise, pre-planned, ideal screw trajectory, helping to prevent pedicle screws from compromising the proximal facet joint. Our previous study recorded no proximal facet joint violations and a larger distance between pedicle screws and facets in the robot-assisted group, compared to the conventional freehand group.9 Additionally, in another study on the effects of robot-assisted pedicle screw fixation, we concluded that it alleviated stress increments at adjacent segments after fusion, compared to the conventional freehand technique.10 Furthermore, if a surgeon with little experience in pedicle screw fixation is educated about the surgical technique with the robot, the robot system will serve consistent pedicle screw insertion according to preoperative planning pathway, even in the early application period, making it a helpful method for less experienced spine surgeons. Nevertheless, the present study failed to detect significant differences in 2-year outcomes, which is surprising and different from the findings of our previous studies.
In contrast with the findings of our previous study,9 several studies regarding percutaneous pedicle screw fixation have revealed higher rates and grades of cranial facet joint violations, which is related to their reliance on intra-operative two-dimensional C-arm images for determining the screw's entry point and trajectory.2122 However, the incidence of adjacent segment disease is similar between the percutaneous technique and the open freehand technique.23242526 In this context, the C-arm or CT-guided navigation system and robot-assisted systems use the same percutaneous screws, although there are methodological differences. For example, C-arm or CT-guided navigation provides intraoperative images that require the surgeon's interpretation and imagination to determine the pedicle screw insertion point, while the robot-assisted technique provides screw trajectory guidance along the pre-planned path independent of the surgeon's ability and experience. This technical difference may explain the lower rates and grades of cranial facet joint violations during robot-assisted pedicle screw insertion.9 However, the robot-assisted or conventional techniques did not provide different ASD outcomes in the present study, and the difference in revision surgery (2 patients vs. 0 patients) was statistically insignificant. That outcome likely requires longer-term radiographic follow-up to detect significant differences. Furthermore, the insignificant difference is likely related to the high grade of preoperative disc degeneration at the proximal adjacent segment (Table 1). In this context, preoperative disc degeneration at the adjacent segment is related to the adjacent segment's disc stress,27 which would indicate that pre-existing degeneration has a greater effect than the screw insertion technique. Thus, the effects of the robotassisted technique would need to be evaluated in patients with nearly normal adjacent discs, although this situation would be extremely rare, as adjacent disc degeneration is strongly related to canal stenosis and spondylolisthesis. Accordingly, additional long-term studies are needed to determine if the robot-assisted technique can provide superior and clinically meaningful outcomes.
The present study demonstrated that the two surgical techniques provided similar improvements in back VAS, leg VAS, and ODI scores at 2-year follow-up. To the best of our knowledge, these are the first radiographic ASD, revision, and clinical outcome-related data regarding the robot-assisted technique, as previous studies have only examined the accuracy of pedicle screw fixation.1234579 Interestingly, our clinical outcomes were somewhat unexpected, and it is somewhat worrisome that the ODI increased slightly during the second year after surgery. Thus, additional follow-up data are needed to determine if the ODI scores continue to increase or subsequently decrease.
This study has several limitations. First, the dropout rate was higher than what we expected, with most patients being lost from the Conv-PSF group, compared to the Robot-PSF group. However, the characteristics of both groups were maintained, which suggests that our findings are meaningful. Second, we did not analyze distal ASD in this study. Our previous study indicated that the robot-assisted technique alleviated stress increments at the adjacent segments after fusion,10 although the present study failed to detect clinically meaningful differences in this context. Therefore, further follow-up is needed to examine long-term ASD. Third, data regarding health-related quality of life (using the Short Form-36 tool) were originally collected, although the data collection was sporadic during the follow-up, which precluded analysis of the quality of life data. Nevertheless, the back pain, leg pain, and disability scores indicated that the results were satisfactory at 2-year follow-up.
In conclusion, the present study did not reveal any significant differences in radiographic ASD or revision rates between the Robot-PSF and Conv-PSF groups, which was unexpected based on the predictions from our previous biomechanical study. Furthermore, the clinical outcomes were similar between the two groups and did not appear to change according to pedicle screw insertion technique. Therefore, the advantages of robot-assisted surgery (i.e., accurate pedicle screw insertion and minimal facet joint violation) do not appear to be radiographically and clinically significant.


 XML Download
XML Download