

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that poses significant social, communication, and behavioral challenges. Many infants with ASD lack vocalization during the first year of life, and may impair communication during future development. Vocal behaviors play a key role in developing language and speech from six to twelve months after birth,1 and infants develop critical vocal behaviors, including canonical babbling and variegated babbling, as they fully develop nonverbal communication skills using gestures and vocalizations.2 As suggested by Patten, et al.,3 canonical babbling at around 10 months of age could be a key milestone in early vocal development of typically developing (TD) children, while children with ASD and those with developmental delays (DD) may fail to reach the initial critical stage of development.
Recent studies have reported that children with ASD exhibit problems with social interaction and motivation and struggle with social functions of language as a result of the very initial phase of language acquisition.4 In contrast, children with DD may or may not have language difficulties as they are often observed to have enough expressive language to communicate effectively, while being unable to articulate sounds correctly.5 Based on these findings, it was thought in the present study that behavioral markers in the social and communication realm would help distinguish children with ASD from those with DD.45 As well-known in the literature, the ability to express emotional and social functions is closely associated with the skills of joint attention (JA), which refers to the process of sharing one's experience of observing an object or event.6 The communicatively interactive behavior of JA is expected to be an early sign of social-communicative ability in TD children, beginning to emerge in the first six months of life and continues to develop through 3 years of age.6 During these pre-linguistic dyadic interactions, infants share emotions and imitate people's expressions, thereby promoting mutual awareness with their social partners.
It has been observed in recent studies that vocalizations in children with ASD are atypical phonations, such as squeals, growls, and yells, and lack JA. Scherer7 was one of the earlier proponents of affect vocalizations, reporting that toddlers with ASD used a significantly higher proportion of atypical and distress vocalizations than TD children and children with DD and further suggesting that most of these vocalization could potentially be considered as an early marker of ASD.38 Findings are conflicting with respect to the extent to which children with ASD express emotions through their vocal behaviors in engaging in emotional communication and empathizing with others.9 Individual variations in the symptoms of children with ASD are likely to reflect the common observation that ASD can range from mild and severe, as the symptoms affect children in different ways, with their severity potentially changing over time. Social-emotional abilities of children with ASD in their early vocalizations have been examined in a limited number of studies,1011 and this lack of research probably lies in the fact that ASD is diagnosed relatively late at around 3 years of age or even later.2 Our research will hopefully provide insight into the nature of atypical vocalizations in children with ASD and the development of screening and intervention programs.3
Our analyses were primarily concerned with the development of emotional and social intent and vocalizations in toddlers with ASD in comparison to those with DD. A set of issues represents a major concern in the analysis of vocalizations collected for this purpose. These issues relate to the frequency of vocalizations with a focus on 1) typicality, 2) emotional intent, and 3) social functions expressed as a JA. We supposed that these issues will allow us to address how the two groups of children may differ in rate and quality of various types produced through their vocalizations.
Go to : 
MATERIALS AND METHODS
Participants
Participants in the current study were recruited from Sewon Infant Child Development Center (SICDC) with informed consent for the research to collect data. This research was approved by the Institutional Review Board of Sogang University (SGUIRB-A-1703-10).
Two groups of children participated in our study: 1) 28 toddlers with ASD [27 male children and 1 female child; mean age=31.2 months; chronological age (CA) range=21–38 months; standard deviation (SD)=4.38 months] and 2) 18 toddlers with DD (16 male children and 2 female children; mean age=29.6 months; CA range=13–38 months; SD=6.87 months). Diagnosis of ASD was confirmed via prior diagnosis made by clinical psychiatrists based on Diagnostic and Statistical Manual of Mental Disorders-IV criteria.12 A set of additional diagnostic tests was conducted to evaluate ASD, such as the Social Maturity Scale, Mullen Scales of Early Learning (MSEL), and Childhood Autism Rating Scale.131415 Children with DD were diagnosed by a group of trained professionals in clinical and developmental psychology. DD in this research refers to the children whose MSEL scores did not reach two standard deviations below the mean in two areas or more out of five scales, including Gross Motor, Visual Reception, Fine Motor, Expressive Language, and Receptive Language. The DD group was matched to the ASD group on a measure of verbal IQ [mean (SD): 56.99 (±26.15), 54.45 (±20.10), respectively, t=−0.36, p=0.718]. This variable was computed from averaging age-equivalent scores on the MSEL Expressive Language and Receptive Language scale (Table 1).
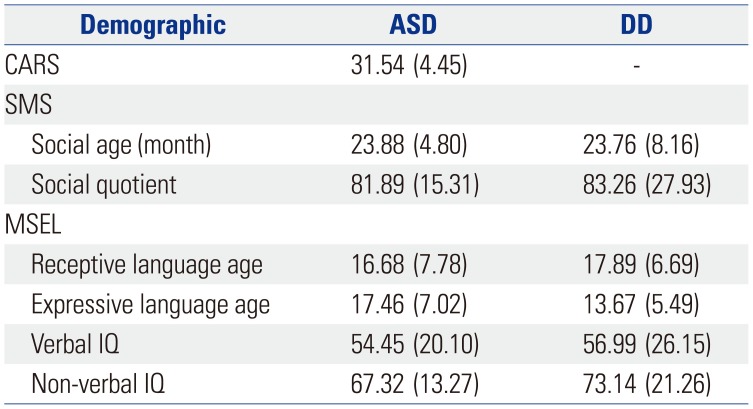
Table 1
Diagnostic Evaluation of the ASD and DD groups
![]()
Data collection
Caregiver-child dyads in both the ASD and DD groups were videotaped during a 10-minute free-play session that took place in the SICDC lab. The lab was soundproof and was designed for child research. It was equipped with a moving motion detector camera and a standard set of toys, such as dolls, cars, trucks, balls, books, and stuffed animals. Selected toys were believed to be suitable for the children's age (13–38 months), and any potential hazards were eliminated for safety purposes. Parents of child participants were instructed to respond naturally when their child sought an interaction and to play as they would at home. In cases where a child displayed a sign of emotional instability due to the unfamiliar environment (e.g., crying, trying to get out of the lab), time was not counted until he or she started to become calm and to show an interest in the lab setting.
Transcription
The 46 video clips were collected and all transcribers were blinded to the participants' group membership. All the 46 sets of verbal samples of the mother-child dyads were transcribed in standard Korean orthography. Phonetically unclear utterances and nonverbal vocalizations were written phonemically with an annotation describing the speaker's intention as related to the discourse context. Description of nonverbal contexts included spontaneous events (e.g., falling objects, sudden ringing), gaze behaviors, and gestures and actions (e.g., touching, reaching, stomping). Particular attention was paid to these categories as the present study aimed to observe the emotional and communicative intent of children's vocalizations. Transcripts were edited in accordance with the Codes for the Analysis of Human Transcripts (CHAT) coding system of the Child Language Data Exchange System.16
Coding system
For the purpose of this research, three categories of codes were developed and edited in the CHAT mode, as follows.
Vocalizations
Nonverbal sounds were categorized into five types in accordance with previous studies.317 Two types were identified as atypical vocalizations, including high-pitch squealing and yelling sounds. Babbling sounds refer to speech-like vocalizations in contrast to the atypical vocalizations.317 The remaining two types are laughter and distress sounds like crying, whining, or fussing.17
Emotion
For a closer examination of the vocalizations associated with affective expressions to be conducted, seven codes were developed to describe six types of basic emotions including happiness, anger, sadness, surprise, fear, and disgust.18 In addition, painfulness was included as reflected in reports that children with ASD are less responsive to others' pain and are less likely to express their own pain.19
Social interactions
The quality of social interactions during the production of vocalizations was evaluated in terms of JA. Social interactions were largely divided into two categories depending on whether the child's attention was jointly focused or not. Each instance of jointly attended vocalization was given closer investigation via sub-categorization into two types: dyadic and triadic JA.20 A dyadic JA is expected to occur when one looks jointly toward discourse topics, such as persons, objects, or events, with or without an active interaction with the interlocutor; meanwhile, a triadic JA is typically observed when one is jointly engaged in a discourse topic by actively interacting with or responding to the interlocutor.20
Interrater reliability
Reliability for all coding categories was assessed on the first 100 vocal samples from two children (77 from one and 23 from the other) by comparing codes that were rated individually by three trained coders. Degree of agreement was calculated based on generalized kappa statistics. Kappa coefficients exceeded 0.75 overall, and were highest for vocalization types (0.87), emotion (0.79), and social communication (0.76).
Go to :
RESULTS
The main goal of this research was to examine the frequencies of vocalizations in children with ASD in comparison to children with DD in terms of typicality, emotional expression, and social functions produced in the context of JA. In order to address these questions, we began by describing the results of vocalizations in the two groups of children with ASD (n=28) and with DD (n=18) on each of the issues raised above. The Kolmogorov-Smirnov test in SPSS showed that the verbal IQ and the non-verbal IQ scores of both ASD and DD groups were normally distributed at the 95% confidence level. Thus, we adopted independent sample t-tests in SPSS (ver. 20, IBM Corp., Armonk, NY, USA) in order to compare the vocal performances of ASD and DD groups.
Overall frequencies of vocalizations were calculated to distinguish typical vocalizations from atypical instances in the two groups. As can be seen in Table 2, the mean number of atypical vocalizations was larger in children with ASD than in those with DD, with the difference being statistically significant (t=2.321, p<0.05). While there was no significant difference statistically, the number of typical vocalizations was larger in children with DD than in those with ASD.
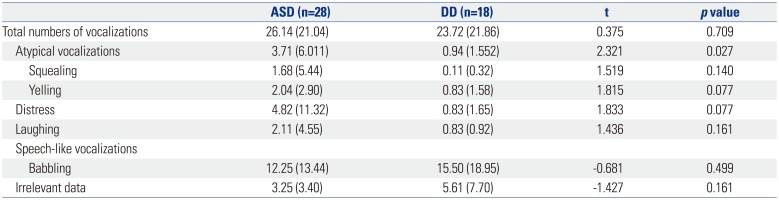
Table 2
Mean Frequencies of Typical Versus Atypical Vocalizations in Children with ASD and Those with DD
![]()
A t-test was also carried out on the frequencies of emotional types of vocalizations in children with ASD and those with DD. Table 3 shows that there was a statistically significant difference between the two groups with respect to emotional characteristics of vocalizations produced in the contexts of non-joint focus of attention (t=2.501, p<0.05). The frequency of emotional properties of the vocalizations in the non-joint focus of attention contexts in the children with ASD was greater than in the children with DD, while the total number was relatively small.
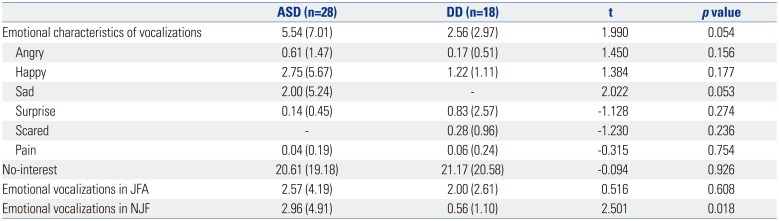
Table 3
Mean Frequencies of Emotional Vocalizations in Children with ASD and Those with DD
![]()
The social skills in the two groups of children were examined in regards to whether their behaviors of attention were jointly-focused and whether their jointly focused attentions (JFAs) were dyadic or triadic, if any. Concerning the first question, results of the data analyses indicated that, as shown in Table 4, JFAs were more frequent in the social behaviors of children with DD than in those of children with ASD. The number of non-JFAs (NJFs) was higher in the vocalizations in children with ASD than in those with DD, the difference being statistically significant (t=3.424, p<0.01). The children with ASD used significantly less babblings in their JFA behaviors (t=−2.121, p<0.05), while producing significantly more babblings in their NJF counterpart, compared to the children with DD (t=2.585, p<0.05).

Table 4
Mean Frequencies of Joint Focus of Attention and Non-Joint Focus of Attention in Children with ASD and Those with DD
![]()
As shown in Table 5, a statistically significant difference was present between the children with ASD and those with DD in the number of triadic types of JFAs. The children with DD were engaged in the triadic contexts of JFAs with a higher frequency than those with ASD (t=−2.411, p<0.05); both groups showed no difference in being engaged in the dyadic contexts.

Table 5
Mean Frequencies of Dyadic vs. Triadic Joint Focus of Attention in Children with ASD and Those with DD
| ASD (n=28) | DD (n=18) | t | p value | |
|---|---|---|---|---|
| JFA in vocalizations | 7.64 (7.42) | 17.39 (20.79) | −1.912 | 0.070 |
| Dyadic in JFA | 4.36 (5.00) | 4.06 (4.99) | 0.200 | 0.842 |
| Triadic in JFA | 3.29 (3.92) | 13.33 (17.40) | −2.411 | 0.027 |
![]()
Go to :
DISCUSSION
Three main questions were addressed in the present study with a focus on the production of vocalizations in children with ASD and those with DD with regard to the rate and quality of typicality, emotional intent, and social skills engaged in JA behaviors. It was discovered in this research that vocalizations in children with ASD were significantly more atypical, less focused jointly in triadic social contexts, and less emotional in behaviors of non-joint focus of attention than in children with DD.
The main results of this study confirmed previous studies reporting that few vocalizations with emotionally and socially appropriate behaviors in children with ASD. As observed in a number of studies, from infancy onward, individuals with ASD exhibit impairment of social gaze, failure of joint focus of attention, and the lack of expression and recognition of emotions.21222324
It is important to note that fewer instances of vocalizations were found in children with ASD in this study in association with the triadic types of JAs. Studies on sensitivity to triadic attention are extremely rare, and it is speculated that our main findings potentially will provide an insight into the development of early screening tools if it were the case that sensitivity to triadic attention begins to emerge by 3 months of age.21 Further studies on the triadic type of JA behaviors need to be conducted in light of the fact that triadic interactions are crucial for imitation, language development, and further learning as they involve a three-way monitoring, namely, an object of joint focus, the attention of another person as related to the self, and the attention of the other person toward the object.
In summary, we observed a set of distinctive properties of early vocalizations in toddlers diagnosed with ASD, compared to those with DD. One of the most prominent clinical features is the emotional and social deficit of ASD, and we have discovered specific forms along the similar lines in this study. The lack of social skills in triadic interactions of JA observed in the ASD group in this study could have an implication for early screening, considering that the development of triadic JA in children with ASD has hardly been examined.
It is speculated that social deficit as discussed above may be associated with a lack of ability to coordinate affective attunement with others.21 Given the impairment to perceive the functional significance of an event,2125 children with ASD would have difficulty recognizing and responding accordingly to the affective expressions of others. This points to a possibility that lack of perception of attunement with others in children with ASD could lead to impairment in their ability to socially interact in their behaviors of JA.26
Our study potentially has limited validity due to the relatively small sample. Part of this problem lies in the fact that this is retrospective research that largely depends on existing samples. To our knowledge, a number of vocalization samples available in children with ASD, as well as in TD children, did not employ the same methods of diagnostic measures, and were selectively used for the purpose of this research. As it turned out, the current number of children was the maximum size sufficient to participate in our investigation in terms of CA and diagnostic methods. It is hoped that prospective research has a larger set of data samples and participants with and without ASD in the near future, so that a contribution can be made to our understanding of the emotional and social functions of early vocalizations implicated in autism.
In closing, given different forms of communication in children with ASD in their emotional and social vocalizations as observed in our research, it would be essential to realize that quality care is provided efficiently with a successful communication style among children with ASD, primary caretakers, and healthcare practitioners. It is hoped that findings in this study will facilitate the development of the communication techniques for children with ASD and caregivers to adapt to in order to help communication breakdowns to be minimized.
Go to :
 XML Download
XML Download