

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a typical systemic vasculitis involving small sized vessels. AAV mainly includes 3 variants, granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA).1 Despite several differences in genetic backgrounds, aetiologies, ANCA type and histologic findings between GPA and MPA, these AAV variants exhibit similar clinical manifestations such as kidney, lung, and ear nose throat (ENT) involvements.234 Meanwhile, EGPA exhibits allergic features including asthma and eosinophilia.25 In the pathogenesis of AAV, various endogenous and exogenous factors trigger pro-inflammatory environment via activating circulating Th17 cells and macrophages, leading to priming neutrophils.6 Also, natural (homeostatic) ANCA can be converted into pathogenic ANCA by impaired B and T cells as well as enhanced B cell stimulation by ANCA activated neutrophils.7 Primed neutrophils bound to pathogenic ANCA subsequently transmigrate into the vessel-adjacent tissues and provoke inflammation.8 At this phase, neutrophil might be consumed in the peripheral blood.
As the consumption of neutrophils increases, the number of immature granulocytes may be elevated. This is called the granulocytic shift to the left which usually reflects the enhanced production of granulocytes in bone marrow.9 In the clinical settings, the immature granulocytes count has been widely used for infectious conditions. Leukocyte sub-fraction has been manually counted, but currently is being automatically measured by subtracting the fraction of mature polymorphonuclear leukocytes from the sum of myeloperoxidase (MPO)-reactive cells, which is called delta neutrophil index (DNI).1011 DNI was reported to be associated with neutrophil-consumption such as disseminated intravascular coagulation (DIC) scores or the mortality of patients with sepsis.1213 Moreover, we previously proved the clinical implication of DNI in differentiating rheumatic diseases from infectious diseases.141516
In the pathogenesis of AAV, neutrophils and antibodies against neutrophils are important participants,7 and the immature granulocytes count can be theoretically elevated like DIC as AAV progress. Thus, it is reasonably speculated that DNI can reflect not only the extent of participation of neutrophil in the AAV pathogenesis, but also cross-sectional vasculitis activity of AAV. Furthermore, because the more neutrophils involved in the early phase of AAV may leave the more serious complications, we expected that DNI can predict poor prognosis of AAV during the follow-up. To the best of our knowledge, however, there was no report on the role of DNI in AAV. In this study, therefore, we first investigated whether DNI might be associated with Birmingham vasculitis activity score (BVAS) at diagnosis and could predict relapse during the follow-up in patients with AAV.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the electronic medical records of 97 patients according to the inclusion criteria as follows: 1) patients who had been first classified as GPA, MPA, and EGPA from January 2010 to January 2017 at Department of Internal Medicine, Yonsei University College of Medicine, Severance Hospital; 2) those who had the results of DNI, which had been reported since January 2010 at our institute; 3) those who met the 1990 American College of Rheumatology criteria for GPA and EGPA, and who were reclassified as the same or another AAV by the 2007 European Medicine Agency algorithm and the 2012 Chapel Hill Consensus Conference criteria for all AAV;1,345 4) those who had the results of both MPO-ANCA and proteinase 3 (PR3)-ANCA by the enzyme-linked immunosorbent assay (ELISA) at diagnosis. Perinuclear (P)-ANCA and cytoplasmic (C)-ANCA were excluded to increase reliability in this study;17 5) those who had documented medical records clear enough to assess BVAS or BVAS for GPA, five factor score (FFS) (1996), and FFS (2009) at diagnosis;18192021 6) those who had no concomitant or previous medical conditions to confuse AAV classification, such as malignancies and serious infections, confirmed by the 10th revised International Classification of Diseases; 7) those who had not received medications to affect ANCA positivity searched by the Korean Drug Utilization Review (DUR) system. Twenty patients (20.6%) had GPA, 58 (59.8%) had MPA and 19 (19.6%) had EGPA. This study was approved by the Institutional Review Board of Severance Hospital (4-2017-0673).
Clinical data, BVAS, FFS and disease course
We obtained the demographic data such as age, gender, and the follow-up duration. We defined the follow-up duration as the period from diagnosis to the last visit of patients achieving remission without relapse. Meanwhile, we defined it as the period from diagnosis to the first relapse in patients with relapse. We collected organ-based items of BVAS or BVAS for GPA as clinical data, assessed BVAS and BVAS for GPA, and calculated FFS (1996) and FFS (2009).18192021 In our study, BVAS implied both BVAS and BVAS for GPA. We also collected medications administered, which could influence the risk of relapse of GPA and MPA such as glucocorticoid, cyclophosphamide, mycophenolate mofetil, azathioprine, calcineurin inhibitor, methotrexate, and rituximab, during the follow-up or just prior to relapse and compared those between patients with above and below the cut-off of DNI as described in Supplementary Table 1 (only online) by under the Korean Drug Utilization Review (DUR) system. Remission was defined as absence of disease activity attributable to active disease qualified by the need for ongoing stable maintenance immunosuppressive therapy. Relapse was defined as recurrence or new onset of disease attributable to active vasculitis after remission.2223
Laboratory data
We gathered laboratory data including white blood cell, haemoglobin, RDW, prothrombin time (international normalised ratio), fasting glucose, blood urea nitrogen, creatinine, protein, serum albumin, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, total cholesterol, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Clinical assessments were performed at the same day of blood tests. A specific type of automatic cell analyser (ADVIA 2120, Healthcare Diagnostics, Forchheim, Germany) was used to determine DNI as previously described.141516 Our institution provides DNI as a part of routine complete blood count. MPO-ANCA and PR3-ANCA had been measured with ELISA kit for anti-PR3 and anti-MPO (Inova Diagnostics, San Diego, CA, USA) before 2013, and by the novel anchor coated highly sensitive (hs) Phadia ELiA (Thermo Fisher Scientific/Phadia, Freiburg, Germany) using human native antigens, performed on a Phadia250 analyser (Thermo Fisher Scientific/Phadia) after 2013.2425
Statistical analysis
All statistical analyses were conducted using SPSS software (version 23 for windows; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean±standard deviation, and categorical variables were done as number and the percentage. The correlation coefficient between DNI and other continuous variables was obtained by the univariate Pearson's correlation analysis. The standardised correlation coefficient between BVAS and other continuous variables was assessed by the multivariate linear regression analysis using variables with significant differences in the univariate analysis. In this study, the highest quartile of BVAS was 20 or greater, and we defined MPA or GPA having BVAS ≥20 as severe AAV. The optimal cut-off of DNI was extrapolated via calculating the area under the receiver operator characteristic (AUROC) curve and selected when its sum of sensitivity and specificity was maximised. The relative risk (RR) of DNI under the initial BVAS ≥20 was evaluated using the contingency tables and the chi square analysis. The Kaplan-Meier survival analysis was used to analyse cumulative relapse free survival rate. p-values less than 0.05 were considered statistically significant.
RESULTS
Baseline characteristics
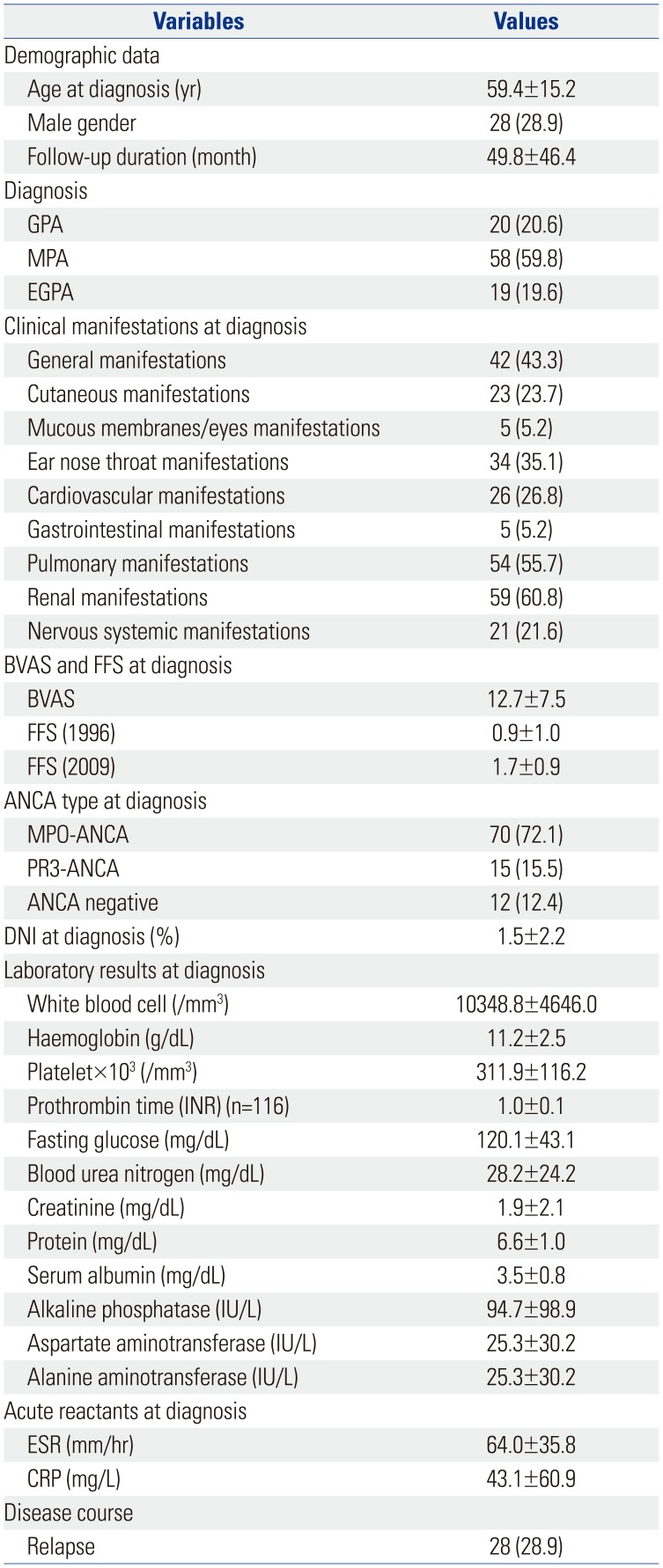
The baseline characteristics are summarised in Table 1. The mean age of 97 patients [28 men (28.9%)] was 59.4 years, and the mean follow-up duration was 49.8 months. The most frequent clinical manifestation was renal involvement (60.8%), followed by pulmonary (55.7%), general (43.3%), and ENT (35.1%) manifestations. The mean initial BVAS, FFS (1996), and FFS (2009) were 12.7, 0.9, and 1.7, respectively. MPO-ANCA was detected in 70 patients (72.1%) and PR3-ANCA was found in 15 patients (15.5%). The mean DNI was 1.5%. The mean ESR and CRP were 64.0 mm/hr and 43.1 mg/L, respectively. Twenty-eight patients (28.9%) had relapse during the follow-up.
Correlation between DNI and other continuous variables in 97 patients with AAV at diagnosis
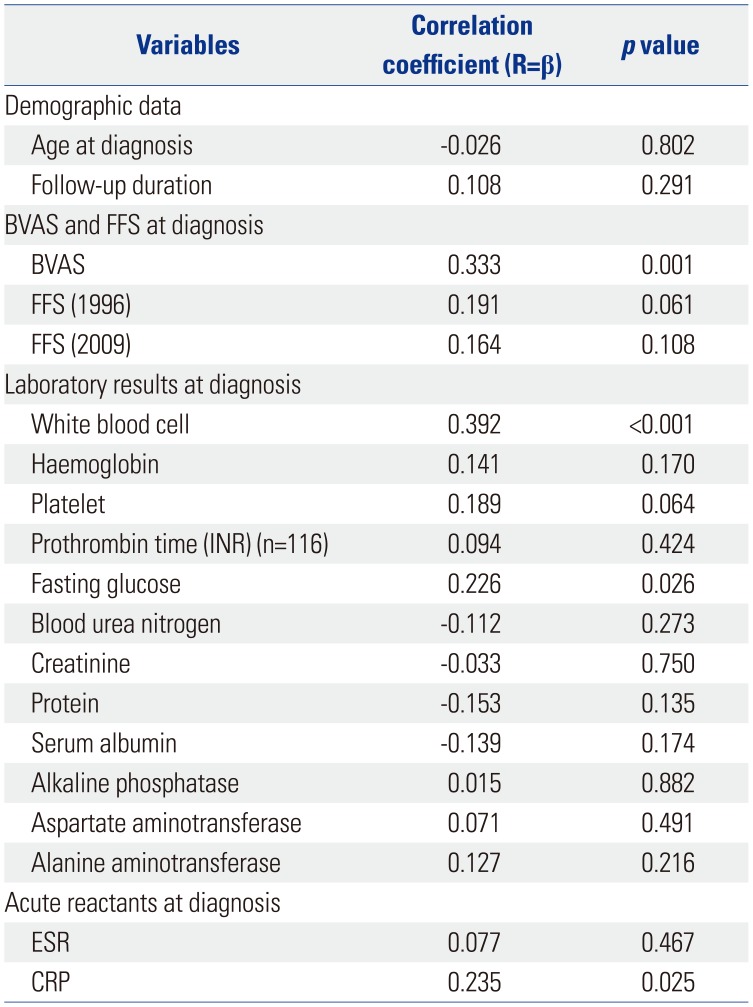
DNI was significantly related to BVAS at diagnosis (r=0.333, p=0.001), and DNI was also significantly linked to white blood cell (r=0.392, p<0.001), fasting glucose (r=0.226, p=0.026), and CRP (r=0.235, p=0.025) (Table 2).
Univariate and multivariate linear regression analyses of BVAS and other continuous variables in 97 patients with AAV at diagnosis
Univariate linear regression analysis showed that BVAS was significantly related to DNI (r=0.332, p=0.001). BVAS was also positively linked to blood urea nitrogen (r=0.251, p=0.013), creatinine (r=0.222, p=0.029), and CRP (r=0.239, p=0.023), and was negatively linked to haemoglobin (r=−0.213, p=0.036), protein (r=−0.313, p=0.002), and serum albumin (r=−0.357, p<0.001). Although BVAS was significantly related to FFS (1996) (r=0.386, p<0.001), and FFS (2009) (r=0.802, p=0.047), FFS was excluded in multivariate linear regression analysis due to the risk of multicollinearity between BVAS and FFS. Multivariate linear regression analysis indicated that only DNI among continuous variables was associated with BVAS with statistical significance in univariate linear regression analysis [β=0.312, 95% confidence interval (CI) 0.359–1.780, p=0.004] (Table 3).
Correlation between DNI and other continuous variables in 78 patients with GPA and MPA at diagnosis
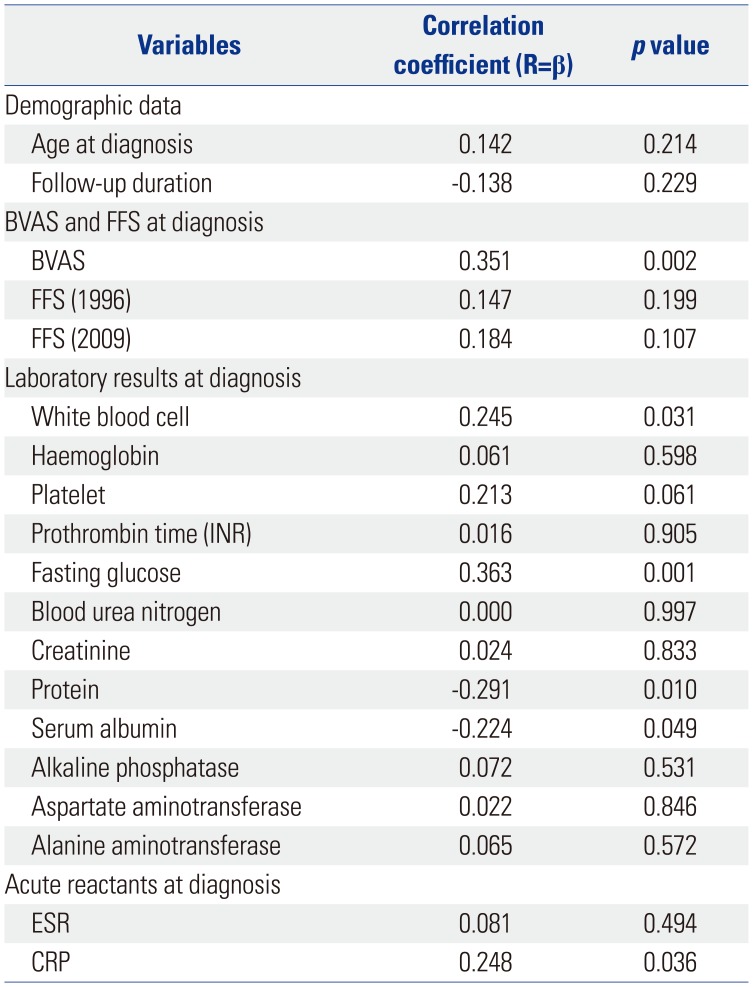
We conducted sub-group analyses in each variant of AAV. DNI was significantly related to BVAS in patients with GPA (r=0.730, p<0.001) and MPA (r=0.290, p=0.027), but not in those with EGPA (r=0.415, p=0.078). Therefore, we excluded patients with EGPA and reanalysed the association of DNI with BVAS at diagnosis in 78 patients with MPA and GPA. DNI was significantly related to BVAS (r=0.351, p=0.002). It was also significantly linked to white blood cell (r=0.245, p=0.031), fasting glucose (r=0.363, p=0.001), and CRP (r=0.248, p=0.036), and was inversely linked to protein (r=−0.291, p=0.010) and serum albumin (r=−0.224, p=0.049) (Table 4).
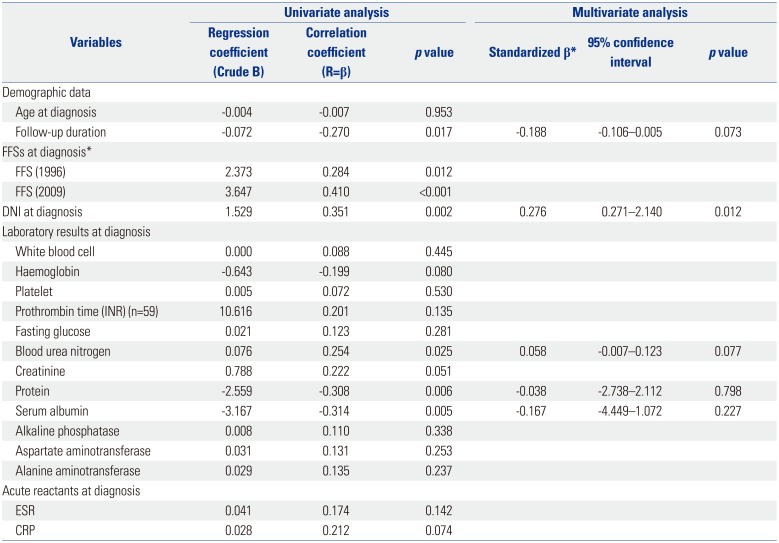
Univariate and multivariate linear regression analyses of BVAS and other continuous variables in 78 patients with GPA and MPA at diagnosis
Univariate linear regression analysis exhibited that BVAS was significantly related to DNI (r=0.351, p=0.002). BVAS was also positively linked to blood urea nitrogen (r=0.254, p=0.025) and was negatively linked to the follow-up duration (r=−0.270, p=0.017), protein (r=−0.308, p=0.006), and serum albumin (r=−0.314, p=0.005). However, BVAS was not linked to ESR or CRP. FFS was excluded in multivariate linear regression analysis due to the risk of multicollinearity between BVAS and FFS. Multivariate linear regression analysis indicated that only DNI among continuous variables was associated with BVAS with statistical significance in univariate linear regression analysis (β=0.276, 95% CI 0.271–2.140, p=0.012) (Table 5).
The optimal cut-off of DNI to identify severe AAV in 78 patients with GPA and MPA at diagnosis
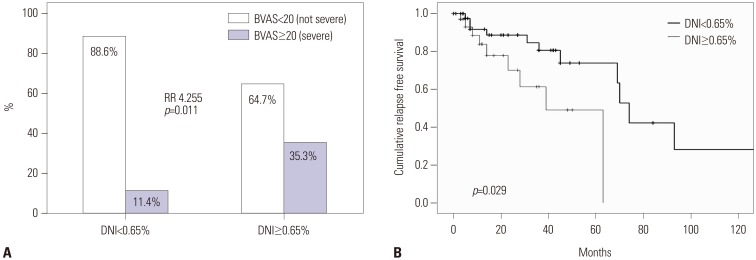
We divided patients with GPA and MPA into the two groups according to the cut-off of severe AAV. Seventeen patients (21.8%) had BVAS ≥20 and belonged to severe AAV group. We calculated the optimal cut-off of DNI to identify severe AAV, and found that 0.65% was a strong measurement of severe AAV (AUROC 0.664, 95% CI 0.516–0.813, p=0.039; sensitivity 70.6% and specificity 63.9%). We also divided 78 patients with GPA and MPA into the two groups according to the optimal cut-off of DNI. There were no significant differences in medications administered during the follow-up or prior to relapse between patients having DNI ≥0.65% and those having DNI <0.65% (Supplementary Table 1, only online). Severe AAV was identified more often in patients having DNI ≥0.65% than those having DNI <0.65% (35.3% vs. 11.4%, p=0.011) (Fig. 1A). Moreover, patients having DNI ≥0.65% had a significantly higher risk of severe AAV than those not having (RR 4.255, 95% CI 1.325–13.665).
DNI at diagnosis to predict relapse in 78 patients with GPA and MPA during follow-up
We evaluated whether DNI at diagnosis could predict relapse during the follow-up of patients with MPA and GPA. First, because DNI was significantly related to BVAS at diagnosis, and BVAS at diagnosis could predict poor prognosis during the follow-up in previous studies,2425 we calculated the optimal cut-off of DNI at diagnosis to predict relapse of MPA and GPA, however, we could find no optimal cut-off (AUROC 0.460, p=0.589). Second, we divided 78 patients with GPA and MPA into the two groups according to the presence of relapse, and compared DNI, BVAS, FFS (1996), and FFS (2009). Patients with relapse exhibited the higher mean BVAS and FFS (1996) than those without [17.5 vs. 10.8, p<0.001 for BVAS, and 1.3 vs. 0.7, p=0.013 for FFS (1996)]. However, DNI did not differ between the two groups (1.9 vs. 1.3, p=0.239). Last, because DNI ≥0.65% could identify severe AAV, we investigated its potential as a predictor of relapse using Kaplan-Meier survival analysis. Cumulative relapse free survival rate was depicted in Fig. 1B. According to DNI ≥0.65% at diagnosis, there was a significant difference in cumulative relapse free survival rates between the two groups (p=0.029).
DISCUSSION
In this study, we first reported that DNI was associated with BVAS at diagnosis and could predict relapse during the follow-up in patients with AAV. DNI was remarkably related to BVAS and furthermore, among continuous variables, only DNI could reflect BVAS at diagnosis in not only all patients with AAV, but also patients with GPA and MPA. However, because the association of DNI with BVAS was not apparent in patients with EGPA, we selected the results on patients with only GPA and MPA. In addition, we provided the optimal cut-off of DNI of 0.65% for identifying severe AAV based on BVAS, and found that patients having DNI ≥0.65% had significantly higher risk of severe AAV (GPA and MPA) than those not having (RR 4.255) at diagnosis. On the other hands, we applied DNI ≥0.65% to predict relapse of GPA and MPA during the follow-up, and found a significant difference in cumulative relapse free survival between the two groups according to DNI ≥0.65% (p=0.029). We, therefore, concluded that DNI could reflect BVAS at diagnosis and furthermore, DNI ≥0.65% could not only identify severe AAV at diagnosis, but also predict relapse during the follow-up in patients with GPA and MPA.
How can DNI reflect BVAS? Based on the pathogenesis of AAV, we assume the link between DNI and BVAS as follows: 1) various aetiologies drive T cells and macrophages to produce inflammatory cytokines, which can prime neutrophils, leading to an increase in adhesion molecules and ANCA antigens on their surface;262728 2) this inflammatory conditions also increase adhesion molecules on endothelial cells;29 3) the ANCA-mediated interaction between primed neutrophils and activated endothelial cells occurs, and activated neutrophils migrate beyond vascular walls;30 4) complement pathway also accelerates the ANCA-associated activation of neutrophils;3132 5) finally, activated neutrophils provoke vasculitis by reactive oxygen radicals and degranulation.7833 Therefore, neutrophils participating in inflammation may be gradually consumed and the number of immature neutrophils increases. With this hypothesis, we speculate that DNI can reflect BVAS of AAV.
Although DNI at diagnosis ≥0.65% significantly reduced cumulative relapse free survival compared with DNI at diagnosis <0.65% in Kaplan-Meier survival analysis, we failed to obtain the optimal cut-off of DNI at diagnosis to predict relapse of GPA and MPA during the follow-up in AUROC analysis. We recently have reported the predictive value of BVAS at diagnosis for relapse of AAV and polyarteritis nodosa.242534 With this concept, we compared the potential of DNI with BVAS at diagnosis for predicting relapse of GPA and MPA during the follow-up. We calculated the optimal cut-off of BVAS at diagnosis to predict relapse using AUROC, and found that 15.5 of BVAS had the strongest predictive value (AUROC 0.746, 95% CI 0.618–0.874, p=0.001; sensitivity 66.7% and specificity 77.2%). Also, we found that patients having BVAS at diagnosis ≥15.5 had the lower cumulative relapse free survival than those not having (p<0.001). Moreover, we conducted a Cox Hazard model using DNI ≥0.65% and BVAS ≥15.5 at diagnosis to predict relapse. Before a Cox Hazard analysis, we investigated the multicollinearity between DNI ≥0.65 and BVAS ≥15.5 using a multivariate linear regression test, and found no significant multicollinearity (variance inflation factor was 1.140). When we performed a Cox Hazard model using those two variables, we found that only BVAS ≥15.5 showed the predictive significance for relapse (odds ratio 6.174, 95% CI 2.268−16.805, p<0.001). Although DNI ≥0.65% showed a significant predictive potential for relapse in Kaplan-Meier survival analysis, it could not surpass that of BVAS at diagnosis ≥15.5.
We studied the reason of why the predictive potential of DNI could not reach that of BVAS at diagnosis and suggested that DNI is the current progressive type, while BVAS is the current completion type. In the putative sequence of the pathogenesis of AAV, neutrophil priming and activation through loss of tolerance of T and B cells and ANCA autoimmune response initiates acute injury.733 At this phase, most participants are neutrophils.
Meanwhile, the next step switches on innate immunity responses, leading to either resolution or sclerotic progress including granulomatosis formation. At this phase, most participants are lymphocytes and macrophages.8 Because DNI is closely linked to the consumption of mature neutrophils, DNI might be predominantly associated with neutrophil-predominant phase, whereas BVAS might be predominantly associated with irreversible sclerotic phase. In addition, relapse begins new and acute autoimmune responses on the basis of established chronic sclerosis, fibrosis, and granulomatosis more often than on that of normal tissues. Not a few patients are classified as AAV at chronic irreversible sclerotic phase rather than at acute neutrophil-predominant phase. Thus, BVAS at diagnosis occupies larger phases in the putative sequence of the pathogenesis of AAV than DNI at diagnosis, and BVAS at diagnosis can predict relapse of GPA and MPA better than DNI at diagnosis. On the contrary, because the higher level of DNI at diagnosis implies more likely phase to heal and return to normal tissues, we suggests that patients having high DNI at diagnosis should receive more immediate and aggressive treatment.
Our present study has a strong advantage in that we first proved the association of DNI with BVAS at diagnosis and provided the optimal cut-off of DNI to predict relapse during the follow-up in patients with GPA and MPA. However, our study has also several limitations. First, we could not clarify the mechanism of the association of DNI and BVAS and its predictive value for relapse. Second, because DNI has been reported since January 2010, the number of patients was not large enough to enhance reliability. Last, due to a retrospective design of this study and lack of information on serial BVAS during the follow-up duration, we could not clarify the link between changes of DNI and BVAS over time. Thus, prospective studies with a larger number of patients are required to obtain more reliable information on the role of DNI in AAV
In conclusion, DNI could reflect BVAS at diagnosis and furthermore, DNI ≥0.65% could not only identify severe AAV at diagnosis, but also predict relapse during the follow-up in patients with GPA and MPA.

 XML Download
XML Download