

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Indwelling central venous catheters (CVCs) have the potential to cause bloodstream infections, and the prevention of central line-associated bloodstream infections (CLABSIs) can reduce adverse outcomes, such as excessive medical costs, risk of mortality, and long-term hospitalization.123 For these reasons, the importance of catheter management is emphasized throughout the literature.45678
In our hospital, a tertiary center in South Korea, the incidences of CLABSIs in patients of the intensive care unit (ICU) were 4.8 episodes per 1000 catheter days in 2008, 5.9 in 2009, and 7.8 in 2010. These values remain higher than those of other hospitals of similar scale.9
After providing new updated prevention guidelines in 2011 for intravascular catheter-related infections,10 working groups, including the Centers for Disease Control and Prevention (CDC), emphasized the importance of educating and training health care personnel in CVC placement, namely using maximal sterile barrier precautions (MBPs), chlorhexidine skin preparation, avoiding the femoral vein as an access site, avoiding routine replacement of CVCs, and using antiseptic/antibiotic impregnated short-term CVCs when inserting CVCs. Based on these guidelines, we previously began using chlorhexidine and antiseptic impregnated CVCs,1112 and in 2012, we modified our in-hospital instructions related to MBPs.
The most recent studies that have reported improvements in CLABSI rates have drawn their comparisons from data before and after specific interventions and have primarily targeted patients of the ICU.1314151617181920 In the studies that have included patients who were not from the ICU, only certain parts of the central line (CL) bundle had been included in the reported analyses.212223 To address these limitations, we evaluated CLABSIs according to the rates of completion of CL bundle components, rather than performing a comparison of rates before and after the intervention. In addition, we investigated CLABSI rates for multiple departments, including the ICU, general ward (GW), emergency room (ER), and operating room (OR).
The aim of this study was to evaluate the direct effect of completing all CL bundle components on CLABSI rates, according to the department, after modifying our in-hospital instructions based on updated prevention guidelines.10 In addition, we sought to identify commonalities among weak areas of CL bundle performance between departments. To the best of our knowledge, this is the first study to evaluate rates of CL bundle performance and CLABSIs according to individual hospital departments.
MATERIALS AND METHODS
Study populations and CL bundle components
Data were collected over 3 years (from August 2013 through July 2016) from patients who underwent new CVC insertions during the first week of every month. Patients less than 2 years of age or those with missing data were excluded from the study.
We measured CL bundle performance compliance according to a check list based on CDC guidelines.10 Among the CL bundle components, education and training were conducted uniformly for all medical personnel at our hospital.24 Education and training for infection control were conducted at least twice a year. We regularly promoted the CVC insertion and maintenance guidelines through e-mail. The missing bundle result was sent immediately to the physician who inserted the catheter by mobile text message, and bundle performance check list feedback was reported to the senior staff. Likewise, antimicrobial/antiseptic-impregnated catheters were used exclusively during the study period.
CL bundle performance monitoring consisted of the following four components: hand hygiene, use of MBPs, use of chlorhexidine skin preparation, and selection of an appropriate site for central venous access. All CVC catheters were inserted by a skilled physician, and a third-person nurse, who was not an assistant nurse, reviewed the checklist at the time of catheter insertion.
Definitions
We defined bloodstream infection (BSI) as newly developed primary BSIs without definite evidence of another infection based on the United States National Healthcare Safety Network (NHSN) system.25 In cases where blood cultures were positive for normal skin flora, the identification of the offending organism was based on at least two pairs of blood cultures and the presence of at least one of the following clinical symptoms: fever, chills, or hypotension. The CVC must have been present for at least two additional days, and the CLABSI was defined as the present CVC on either the date when the BSI occurred or the day before the BSI occurred, according to the Korean Nosocomial Infections Surveillance System (KONIS) definition.2627 Catheter day was calculated as the interval between catheter removal and insertion dates, and the CLABSI rate was expressed as the number of CLABSI episodes per 1000 catheter days (Episodes of CLABSI/total sum of catheter day×1000). We reviewed electrical medical records up to 48 hours after CVC removal.
Central venous catheter
We used the ARROW® central venous catheterization set for this study (ARROWg+ard Blue® Catheter with Blue FlexTip®, ARROW International Inc., Reading, PA, USA). Catheters underwent external surface treatment using sulfa antimicrobials, chlorhexidine acetate, and sulfadiazine.
Ethics statement
The protocol for this retrospective study was reviewed and approved by the Institutional Review Board at the Gangnam Severance Hospital of the Yonsei University Health System in Seoul, Korea (Reg. No. 3-2017-0043). The board waived the requirement for informed consent. All procedures were conducted in accordance with the guidelines of the Declaration of Helsinki.
Statistical analysis
Statistical analyses were performed using SPSS statistics, version 23 (IBM Corp., Armonk, NY, USA). Categorical variables are expressed as the frequency and number of CLABSI episodes per 1000 catheter days. Statistical differences among infection rate trends were analyzed using the chi square test. Comparative analysis with the Poisson regression test was used to identify the most important factors associated with CLABSI rates. Results are described as relative risk (RR) with 95% confidence intervals (CIs). p-values <0.05 were considered statistically significant.
RESULTS
Overall CLABSI rates according to CL bundle performance rates
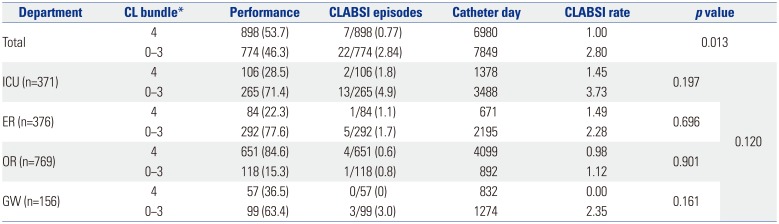
A total of 1672 patients (ICU, n=371; ER, n=376; OR, n=769; GW, n=156) were enrolled over the 3-year study period, and the median length of catheterization was 6.0 [interquartile range (IQR) 3–12] days. Our analysis included a total of 14829 catheter-days, of which we identified 29 (1.73%) CLABSI episodes. All four components of the CL bundle were performed on a total of 898 (53.7%) patients, while one or more components of the CL bundle were omitted for 774 (46.3%) patients. Among patients for whom all four components of the CL bundle were performed, there were 7 (0.77%) CLABSI episodes, with a CLABSI rate of 1.0. On the other hand, there were 22 (2.84%) CLABSI episodes among patients who missed a component of the CL bundle, with a resulting CLABSI rate of 2.80 (p=0.013) (Table 1).
Performance rates of each component of the CL bundle according to department
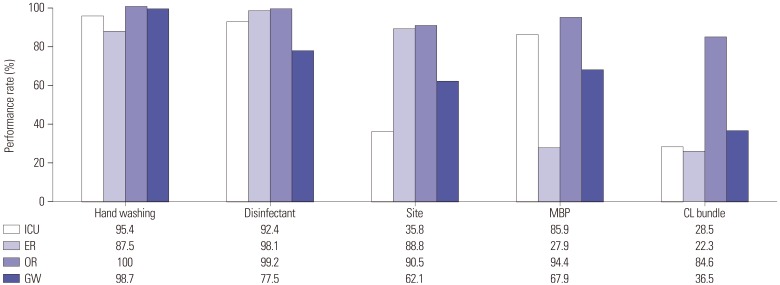
The department-specific rates of performance for each component of the CL bundle are shown in Fig. 1. Notably, the percentage of non-femoral site insertions was 35.8% in patients admitted to ICUs, and the percentage of full MBP compliance was only 27.9% in patients admitted to the ER. The percentages of patients for whom all four components of the CL bundle were performed were 22.3%, 28.5%, and 36.5% for the ER, ICU, and GW cohorts, respectively. Conversely, for the OR cohort, the rate of total compliance with the CL bundle components was 84.6% (Table 1).
Department-specific CLABSI rates according to CL bundle performance
In the ICU, 1.8% of patients who underwent all four components of the CL bundle had a CLABSI, with a resulting CLABSI rate of 1.45. On the other hand, 4.9% of patients for whom one or more components of the CL bundle were omitted had a CLABSI, with a resulting CLABSI rate of 3.73 (p=0.197). A similar trend was noted for patients of the ER (CLABSI episodes; 1.1% vs. 1.7%, CLABSI rates; 1.49 vs. 2.28, p=0.696), patients of the OR (0.6% vs. 0.8%; 0.98 vs. 1.12; p=0.901), and patients of the GW (0% vs. 3.0%, 0 vs. 2.35, p=0.161). In general, CLABSI rates were highest in patients for whom one or more components of the CL bundle were not performed; however, among this subset of patients, there were no significant differences in CLABSI rates between departments (Table 1).
CLABSI rates according to performance of individual CL bundle components
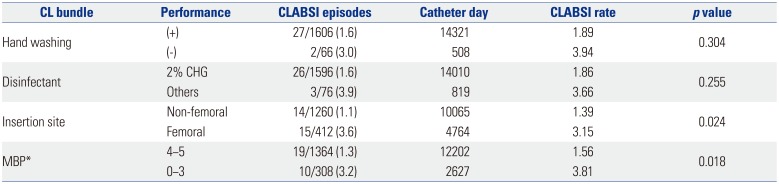
We next examined CLABSI rates according to the performance of each component of the CL bundle (Table 2). The CLABSI rate was lower in patients for whom complete hand washing than in patients for whom hand washing was not performed (1.89 vs. 3.94, p=0.304). Similarly, the CLABSI rate was lower in patients for whom 2% chlorhexidine was used compared to patients for whom another disinfectant was used (1.86 vs. 3.66, p=0.255). The CLABSI rate was also lower in patients with a non-femoral catheter insertion site than in patients with a femoral catheter (1.39 vs. 3.15, p=0.024). For this study MBPs consisted of five components, including a mask, gown, hat, gloves, and full drape. The CLABSI rate was lower in patients for whom at least four of the five MBP components was used than in patients for whom zero to three of the five MBP components were used (1.56 vs. 3.81, p=0.018).
Relative risk for variables associated with CLABSIs
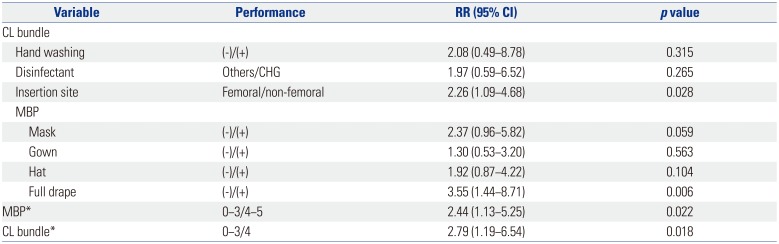
Lastly, the four components of the CL bundle were analyzed using the Poisson regression test. Among the bundle components, it was necessary to exclude gloves from the MBP analysis, which otherwise consists of a mask, gown, gloves, hat, and full drape, as no CLABSIs occurred among the four cases where gloves were not used (Supplementary Table 1, only online). An insertion site in the femoral area [RR, 2.26 (95% CI, 1.09–4.68); p=0.028], not using a full drape [RR, 3.55 (95% CI, 1.44–8.71); p=0.006], use of only zero to three MBP components [RR, 2.44 (95% CI, 1.13–5.25); p=0.022], and not performing all four components of the CL bundle [RR, 2.79 (95% CI, 1.19–6.54); p=0.018] were identified as significant variables associated with an increased risk of CLABSIs (Table 3).
DISCUSSION
While many previous studies on CLABSIs have focused on patients of the ICU,13141516171819 we also included patients from non-ICU departments in the present study. In addition, we analyzed individual components of the CL bundle, including the five components of MBP. The performance rate for completing all four components of the CL bundle was 53.7%, which was lower than expected, based on previously reported rates of 60–80%.282930 The performance rate for the CL bundle, when including cases where only one component was omitted, was 90.4%. However, post-hoc analysis showed that the CLABSI rates for cases wherein only three of the four CL bundle components were used, as well as in cases where only zero to two of the four components were used, were both twice as high as cases wherein all components of the CL bundle were used (Supplementary Table 2, only online). Therefore, in contrast to previous studies showing that CLABSI rates are reduced by partial compliance with the CL bundle,1421 our results suggest that physicians should perform all aspects of the CL bundle completely and without exception.
According to individual departments, the CLABSI rate was the highest among patients in the ICU, where all components of the CL bundle were not performed perfectly, and the CLABSI rate was zero for patients of the GW, where all components of the CL bundle were performed. With respect to each component of the CL bundle, hand washing was generally performed well in all departments, especially in the OR, for 100% of patients. The performance rate of chlorhexidine skin preparation was relatively low in patients of the GW, compared to other departments, which was thought to be due to insufficient preparation and dissemination of information. The reason for the use of a femoral insertion site, which was most prevalent in patients of the ICU, was likely due to the ease of this approach for patients who were immobile and the desire to reduce the risk of pneumothorax.631 However, many previous studies have shown that the femoral approach is associated with a higher risk of CLABSIs, compared to subclavian or internal jugular approaches.6313233 Thus, the continued education of physicians to avoid femoral access for infection control over convenience of insertion is necessary. Lastly, the performance rate for MBPs was significantly lower in patients of the ER, compared to those in other departments.
Notably, among individual components of MBPs, the rate of gown (36.4%) and hat (30.8%) use was lower than the other MBP components. Indeed, the performance rate for using sterile gloves was 100% in all hospital departments except the ER, although the performance rate of this department was still relatively high (98.9%) compared to other MBP components (Supplementary Table 1, only online). In contrast, with respect to the overall performance rate of the entire CL bundle, the rate of compliance of patients of the OR was very high (84.6%). This result likely reflects characteristics of the OR department, which is sensitive to infection control. Based on these results, we believe that a customized strategy and education plan to address department-specific weakness will be useful (Fig. 1, Table 1).
The CLABSI rate according to individual components of the CL bundle confirmed that the site and use of MBPs were significant factors. Among the individual components of MBPs, failure to use a full drape carried the highest risk of CLABSI. Therefore, it is important to approach a non-femoral site6313233 when inserting a CVC and to always use MBPs,223435 especially a full body, sterile drape. Furthermore, it is important to make efforts to perform all aspects of the CL bundle, as doing so reduces the rate of CLABSIs.
There were some limitations to this study. First, there were very few CLABSI episodes (n=29) among the 1672 patients who were enrolled in this study. Owing to this low event rate, there were possibly no significant differences in CLABSI rates according to CL bundle performance. Thus, larger-scale studies that are capable of evaluating more CLABSI episodes will be necessary. On the other hand, because infection management has now become an apparent strength of our hospital, after modifying our in-hospital instructions and education in 2012, our results can serve as a baseline for comparison with other institutions and departments. A second limitation of this study was the relationship between variables. For example, a full drape was one of the components of MBPs, while MBPs were themselves a component of the CL bundle. Therefore, since many of the study variables were related to each other, a multivariate analysis could not be performed. A third limitation was that the factors that may affect CLABSI rates, such as severity of diseases, catheterization days, removal of unnecessary catheter, and catheter maintenance care, were not investigated. The median catheterization time in patients for whom the bundle was performed perfectly was 5.0 (IQR 3–9) days, while this duration was 7.0 (IQR 3–14) days in patients for whom at least one or more components of the CL bundle was not performed. This difference can affect the CLABSI rate, and we focused on the CL ‘insertion’ bundle rather than CL ‘maintenance’ bundle. These factors should be investigated in future studies.
During the 3-year period, we monitored physicians who inserted CVCs using checklists and provided feedback through mobile texts and e-mails. If the CVC was inserted at the femoral site in the ICU or if a gown and hat were not used in the ER, immediate feedback should be provided, and CLABSI rates can be improved through department-customized training.
In conclusion, the results of this study provide direct evidence that completing all components of the CL bundle perfectly in each patient is essential for preventing CLABSIs. Our results support the possibility that infection prevention can be improved through customized education and training of each department, according to individual areas of weak CL bundle performance.
 XML Download
XML Download