

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gustatory system mediates in sense of taste human. It is a fundamental sensory system that is essential for various factors such as nutrition and food selection, pleasurable and sensual aspect of food, efficiency of metabolism, and even a good quality of life. In Japan, approximately 240000 people visit health professionals annually to evaluate their changes in taste.1 As elderly people account for the fastest growing segment of the population, a significant number of them will encounter age-related sensory disorders.2 In addition, since sensory deterioration is known as an early marker in neurodege-nerative diseases,34 evaluation of gustatory function can be an ef-fective part of early diagnostic strategy for the older age group.
Although a significant number of olfactory function tests have been described, only a few valid gustatory function tests have been published.567 So far, no clinical protocol for testing gustatory function has been validated or adapted for a Korean population. The insights of aging, underlying diseases, and drugs on olfactory function are relatively well understood; however, there has been no similar understanding in the field of taste.
Umami, one of the five basic tastes, is considered to be on a different molecular basis compared to the other tastes: sweet, bitter, salty, and sour.89 Umami taste was first described a century ago by Ikeda,10 and is commonly added to some foods in the form of monosodium glutamate. Previous studies have shown significantly positive correlation between umami taste function and physical health condition, especially in elderly people.11 However, a reliable taste test of umami for Koreans has not yet been established. Therefore, we do not have detailed information about the taste of umami.
In most patients, self-reported gustatory function is not reliably correlated with psychophysical test results.12 Evaluation of patients with taste complaints is difficult without standardized quantitative methods of assessment. We, therefore, aimed to provide validated clinical scales, including those for umami taste, to develop and standardize methods and protocols for measuring the sense of taste in a Korean population, as well as to understand the impact of gustatory function and dysfunction on public health. Furthermore, we developed the test to identify modifiable risk factors and develop treatment strategies for clinically significant dysfunction.
Go to : 
MATERIALS AND METHODS
Subjects
Participants were selected upon reviewing the medical records of patients who had undergone septoplasty and/or rhinoplasty at Severance Hospital in Seoul, Korea, from January to August 2016. This study was approved by the Institutional Review Board (No. 4-2016-0706) of Yonsei University College of Medicine in Seoul, Korea. Informed consent was obtained from all participants. From 2015 onwards, patients who underwent planned nasal surgery at our institution were routinely examined by taste and smell tests (Korean Version of Sniffin' Stick, KVSS II13) preoperatively.
Eligibility criteria for this study were patient aged between 8 and 90 years, with normal self-rated taste and smell functions, and within the normal range of KVSS II. Patients with inflammation of the middle ear and paranasal sinuses, head and neck malignancies, history of previous middle ear and/or nasal surgery, as well as those taking drugs that might significantly affect the taste sensitivity14 were excluded from the study.
Finally, 297 patients (190 males and 107 females, mean age 44.96±19.73 years; age range 9–89 years) who had undergone evaluation at our institution were enrolled in this study. Subjects were instructed to refrain from drinking, eating, or brushing their teeth for at least one hour before the test.
Preparation of taste solutions
For assessment of gustatory function, liquid solutions were used. The test consisted of 30 taste solutions [six concentrations of five tastants; sweet (sucrose), bitter (quinine hydrochloride), salty (sodium chloride), sour (citric acid), and umami (monosodium glutamate)]. Solution with the highest concentration of each tastant was scored 1, and solution with the lowest was scored 6 (Table 1). Distilled water was used as the solvent. Successive stimuli concentrations were based on previous reports and a repetitive preliminary experiment for finding the appropriate range.151617 All solutions were administered from 30-mL medicine droppers of similar shape and color. Due to the light sensitivity of quinine hydrochloride, sample droppers were protected from light. Taste solutions were replaced every two months.

Table 1
Concentrations of Taste Stimuli Used in g/mL (Solvent: Distilled Water), Separately for the Five Tastants: Sweet, Bitter, Salty, Sour, and Umami
![]()
Determination of taste detection threshold
The test was performed by filling in a questionnaire, and then measuring taste detection and taste recognition threshold in each patient. After the mouth was rinsed with tap water, one of the tastant solutions was administered as single drop (approximately 40 µL) and placed on the middle part of the anterior one-third of the tongue. Between the drops, patients were educated to rinse their mouths with tap water. Administration of taste solution was performed in random order of tastants, starting with the lowest concentration until the respective tastant was detected twice in a row. We then re-examined concentrations that were one level lower and higher, in order to confirm the exact threshold level. Detection threshold was defined as the lowest concentration of test solution that can be consistently perceived by patients as any taste, while determining the recognition threshold required to discriminate each taste. If patients did not perceive concentration score of 1, they received a score of 0.
Determination of taste recognition threshold
Taste recognition threshold was determined according to the same method used to determine taste detection threshold. However, the patients were asked to choose one of the six verbal descriptors to describe what kind of taste was contained in the tastant solution (“sweet,” “bitter,” “salty,” “sour,” “umami,” or “no taste”). Ultimately, we obtained the overall gustatory function using the number of detected and correctly recognized taste thresholds, which were summed up as the ‘taste score’ of each detection and recognition, with a range of 0–30. The complete taste test for the five tastants required approximately 20 min.
Test reliability
To calculate the test-retest reproducibility, taste test was repeated in 33 healthy subjects (24 men and 9 women, mean age of 34.12±11.54 years with range of 20–63 years) at two different time points (with approximately 2-week interval).
Statistical analyses
SPSS 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Descriptive statistics are expressed as mean±standard error of the mean. Statistical significance of the differences between subgroup scores was assessed using Student's t-test or analysis of variance where appropriate. Pearson statistic was used for correlational analysis. Reproducibility and internal consistency were assessed by intraclass correlation coefficient and Cronbach's alpha coefficient. Alpha level was set at 0.05.
Go to :
RESULTS
Normative values are listed in Tables 2 and 3. Mean values of each detection and recognition threshold for the five tastes in men were consistently lower than in women, while only bitter (p<0.001) and sour (p=0.03) detection threshold and bitter (p<0.001) recognition threshold in men were significantly higher than those in women. Based on the definition of hyposmia in previous studies that used a standardized method,1819 taste score at the 10th percentile recognition threshold was used to differentiate normogeusia and hypogeusia. In our study, therefore, subjects with recognition taste scores <12 were regarded as hypogeusia (Table 4).

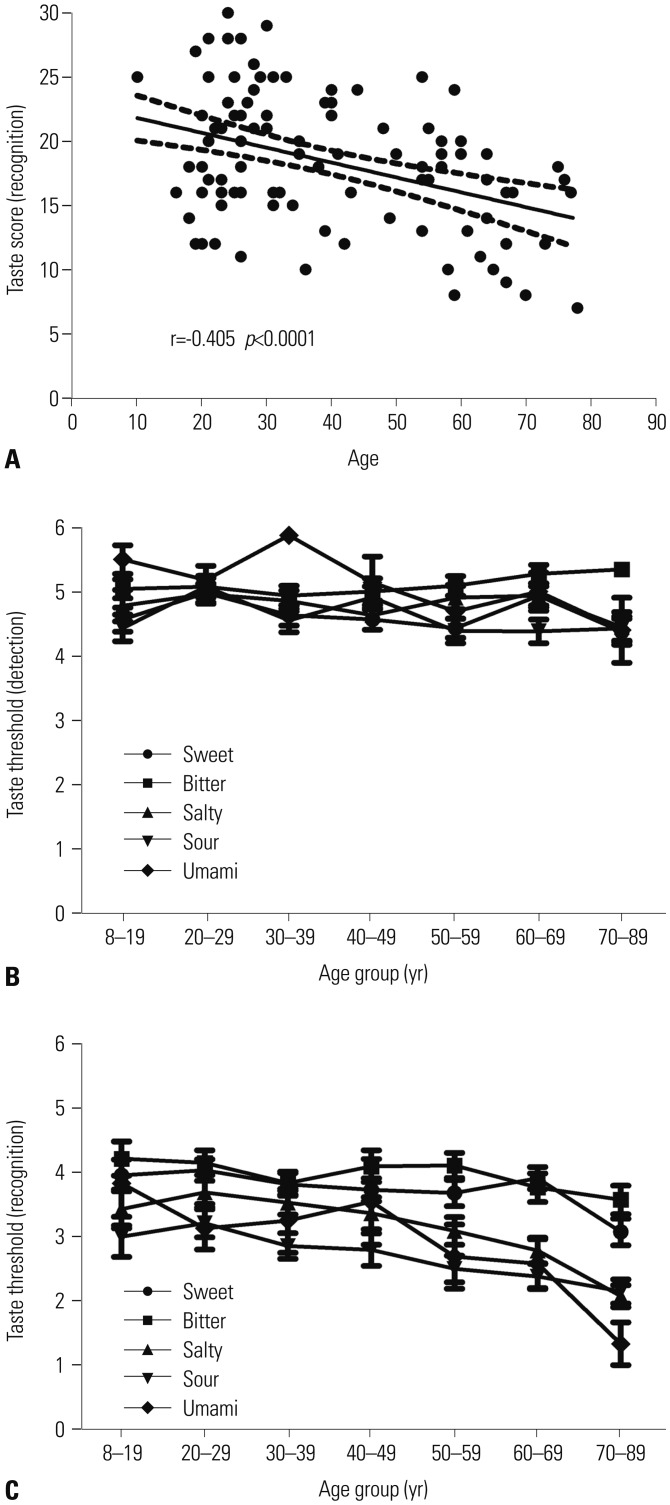
In subgroup analysis, total taste scores from recognition threshold revealed significant negative correlation with age, indicating lower scores for increasing age (r=-0.405, p<0.001) (Fig. 1A). However, the effect of age was not seen on the taste score from detection threshold. In regards to each of the five tastant groups investigated, none demonstrated a statistically significant relationship with age in detection thresholds (Fig. 1B). Interestingly, as shown in Fig. 1C, comparison of recognition threshold obtained for each age group (8–19 years of age, n=23; 20–29 years of age, n=64; 30–39 years of age, n=49; 40–49 years of age, n=30; 50–59 years of age, n=44; 60–69 years of age, n=47; 70–89 years of age, n=40) revealed significant differences with scores being lower with increased age (p<0.05).
Furthermore, the difference in taste function between smoking (n=48, mean age of 45.02±19.02 years, and range 19 to 81 years) and non-smoking (n=235, mean age of 46.67±19.89 years, and range 19 to 89 years) groups was analyzed. Average taste score for non-smokers was significantly higher than for smokers in the detection and recognition taste sensitivity (detection taste sensitivity: 26.16±3.54 vs. 22.58±4.19, p=0.002; recognition taste sensitivity: 19.46±4.57 vs. 11.33±2.54, p<0.001). In the patient study, patients with current and past smoking habits were significantly more likely to be male (44 men and 4 women with current/past smoking habits vs. 137 men and 98 women without such a history, χ2 test, p<0.001). However, alcohol consumption, denture use, serologic tests, body mass index, and baseline blood pressure revealed no relationship with all taste sensitivities.
The present study showed relatively high reliability, and intraclass correlation coefficients between test and retest were 0.61 (0.31–0.80, p<0.001) and Cronbach's alpha was 0.79.
Go to :
DISCUSSION
Any disturbance in taste function can hamper the quality of life by affecting their appetite, body weight, and psychological well-being.20 Taste disorders have been diagnosed by different modalities of gustatory function tests, and there is no consensus for diagnosis or treatment strategies. Although heterogeneous gustatory function tests have been developed over the past few decades, they mainly applied four basic tastes (sweet, bitter, salty, and sour), and not umami. These methods include whole-mouth method,21 filter paper disk method,6,22 threestimulus drop technique,23 and taste strip method.72425 Filter paper disk or taste strip methods use filter paper disk or taste strips that are impregnated with a known concentration of each taste quality. Filter paper disk or taste strip is placed on a specific part of the tongue or palate of the participant, and threshold of distinct area that is innervated by specific taste nerve can be measured. However, filter paper disk and taste strip methods may either lead to inaccurate assessment or cause subjective discomfort, especially for elderly patients with dry mouths.
We designed our gustatory function test as a whole-mouth method that was easy to perform, affordable, and time-saving, with the capacity to self-produce and obtain reliable data. Taste solutions are readily available at any pharmacy at very low cost, and can even be considered to enable a more physiological taste test by better representing real edible stimuli. Although this method is convenient and versatile to use, it cannot assess local damage in the mouth. Since test substance becomes immediately diluted in saliva, values acquired with this method might represent sensation of the oral cavity as a whole. Since the aim of this study was to provide validated clinical data for subjects' gustatory function, regional taste test was not necessary. The taste test presented herein exhibited a good test-retest reliability of 0.79, and correlation coefficient was comparable with other extant taste tests.2426
When comparing recognition threshold values for the five tastants to those from other studies, our concentration was much lower than those obtained by filter paper disk method6,22 and taste strip method.72425 Recognition threshold from filter paper disc or taste strip method can only assess a small area; therefore, higher concentrations of each tastant should be presented in the saliva to reach the taste buds. This may be a small advantage of our study in that it offers a safer taste test.
In our study, detection score of umami taste was the highest in all tastes, whereas its recognition score was lower compared to sweet, bitter, and salty tastes (Tables 2 and 3). For each age group investigated, umami taste seemed to follow a similar pattern in subjects under age of 50 years (Fig. 1B and C). It was not surprising to observe higher total score in the retest session, as psychophysical tests usually tend to improve test results through training. Interestingly, this effect was most noticeable in the umami taste. Consequently, we can assume that umami taste is unfamiliar to younger subjects, as it is difficult to understand the exact concept of “umami.” Nevertheless, taste function of umami could be of great interest in regards to gustatory dysfunction or as a possible nutrition advice.272829 Decreased sensitivity to umami taste may induce loss of both appetite and weight, which can lead to poor overall health, especially in older age group.22


Table 2
Taste Detection Threshold in 297 Korean Individuals
![]()
Table 3
Taste Recognition Threshold in 297 Korean Individuals
![]()
Our present results provide validated clinical scales for routine clinical screening test of the gustatory function. In our subjects, recognition taste score at the 10th percentile was 12. Such data can be used as cutoff value for estimating individual gustatory ability. However, the 10th percentile does not define the border between normogeusia and hypogeusia in all age groups. For example, an 80-year-old individual scoring 11 may be in the 20th percentile, thus being considered “normogeusia” relative to his age group. Nevertheless, as description of absolute gustatory sensitivity should be based on the performance of all age groups, the term “hypogeusia” should be applied to all subjects with recognition taste scores <12.19
Like olfactory function, taste perception becomes somewhat impaired with normal aging. We noted lower score results with increasing age. Interestingly, this effect was most pronounced for recognition threshold. Detection thresholds remained relatively steady with increasing age. The reason for this age-related change is not clear. Furthermore, we observed increased taste score results in nonsmokers compared to smokers, as well as in females compared to male subjects. Anatomical data were consistent with gender differences, as females had more fungiform papillae and taste buds than males.30 Although the cause of such anatomical difference remains uncertain, it may be related to a hormonal factor as well as other dietary habits, smoking behaviors, and alcohol consumption.31 Accordingly, unpredictable bias could be involved in this study.
In light of the different eating habits among different ethnic groups that lead to differences in sensitivity of gustatory function, cross-cultural validation of a taste test is justified. Ribeiro, et al.32 found that a Portuguese population demonstrated lower taste scores than those previously observed in a German population, while Yang, et al.33 showed that a Chinese population did not demonstrate any variation with age or gender. The current study is the first to use a gustatory function test, including umami taste, in a Korean population, and the results may allow improvements in diagnosis, treatment, and follow-up of taste disorders.
One of the limitations of this study was its investigation of gustatory function using a clinical population. For additional information, inclusion of community-based subjects would be required to reach a more meaningful conclusion.
Many clinically encountered taste disorders occur due to factors such as surgery, tumors, inflammatory diseases, trauma, or radiation treatment; therefore, a gustatory function test is diagnostically valuable and facilitates interpretation of taste scores in routine clinical practice. Further studies using more normative data for a gustatory function test are in pregress, and their results will be presented in the near future.
Go to :
 XML Download
XML Download