

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intra-arterial therapy (IAT) using a stent retriever is safe and effective in acute stroke with intracranial proximal artery occlusion.12345678 However, despite successful reperfusion by IAT, some patients do not show clinical improvement. One of the plausible explanations for this futile reperfusion is rapid conversion of ischemic penumbra into irreversible infarct core.910 While patients who already have extensive areas of irreversible damage are usually excluded from reperfusion therapy,811 some salvageable areas can be converted to irreversible infarct core during the reperfusion treatment. However, there are few reports on infarct core progression in the hyperacute stage in patients with proximal artery occlusion, and its prevalence, related factors, and clinical significance are largely unknown.
Before the efficacy of IAT was proven, IAT was sometimes performed as a rescue treatment to patients who do not respond to intravenous tissue plasminogen activator (IV t-PA) after follow-up imaging study. By analyzing two consecutive computed tomography (CT) scans acquired before and shortly after IV t-PA, we investigated the change in the extent of the infarct core during IV t-PA treatment, its associative factors, and clinical significance.
MATERIALS AND METHODS
Study population
We included patients who were potential candidate for IAT due to persistent occlusion of intracranial proximal artery after IV t-PA (Actilyse, Boehringer-Ingelheim, Ingelheim, Germany) and who had two consecutive CT scans before and shortly after IV t-PA. This group was derived from a cohort that was developed to investigate the factors associated with thrombus resolution after IV t-PA.1213 In the cohort, two consecutive noncontrast CT (NCCT) scans were acquired before and shortly after IV t-PA infusion in the same scanner (LightSpeed Plus, GE Healthcare, Milwaukee, WI, USA or SOMATOM Sensation 64, Siemens Healthcare, Erlangen, Germany) (Supplementary Material, only online), and CT angiography (CTA) was taken with follow-up NCCT. For this study, we included patients who had unilateral intracranial proximal artery [internal carotid artery (ICA), middle cerebral artery (MCA) M1, or M2] occlusion on CTA between January 2009 and December 2014. We excluded patients who already had a large infarct core in the initial NCCT, indicated by an Alberta Stroke Program Early CT Score (ASPECTS) <6. Patients received IV infusion of t-PA within 3 hours of symptom onset until December 2012 and within 4.5 hours thereafter. Additional IAT was considered if patients did not show a satisfactory clinical response [<50% improvement as measured by the National Institutes of Health Stroke Scale (NIHSS) score] to IV t-PA infusion.
Image analysis
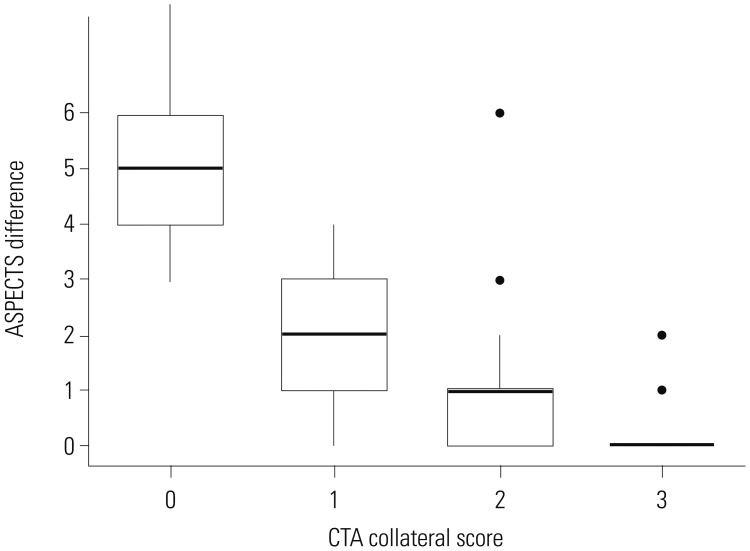
In this study, infarct core was defined as low-density area on NCCT and calculated based on the ASPECTS scoring system. ASPECTS was measured with NCCT using revised methodology, which does not account for isolated cortical swelling.14 Patients were classified into three groups: no, moderate, and marked expansion groups, defined based on a decrease of 0??, 2??, and ≥4, respectively, in ASPECTS between the two scans. The CTA-collateral score (CTA-CS) was measured with reconstructed maximum intensity projection CTA images as follows: 0=absence of collateral supply to the occluded vascular territory; 1=collateral supply filling <50%, but >0% of the occluded vascular territory; 2=collateral supply filling >50%, but <100% of the occluded vascular territory; and 3=collateral supply filling 100% of the occluded vascular territory.15 Two stroke neurologists, who were blinded to all clinical information, other than the side of the infarction, independently reviewed the CT scans and measured ASPECTS and CTA-CS. Disagreements between the two readers were resolved by consensus. Good collateral status was defined as CTA-CS ≥2.
Clinical variables and outcomes
Stroke mechanisms were determined based on the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification. The initial stroke severity was assessed using the NIHSS, and the functional outcome was measured using the modified Rankin Scale (mRS) score at 90 days. The degree of reperfusion was graded by the Thrombolysis in Cerebral Infarction (TICI) scale in the final run of IAT. TICI scales of the patients who did not undergo IAT were graded with 24-hour follow-up MR angiography. We obtained outcome data and clinical variables, such as vascular risk factors, laboratory results, and time metrics, from the aforementioned prospective cohort. Successful reperfusion was defined as TICI ≥2b, and a favorable outcome was defined as mRS ≤2. Symptomatic intracranial hemorrhage (ICH) was defined as any hemorrhage associated with neurological deterioration, as indicated by a decrease of 4 points on the NIHSS within 7 days (European Cooperative Acute Stroke Study III definition).16 This study was approved by the Institutional Review Board of Severance Hospital (IRB No. 4-2013-0828), Yonsei University Health System, with a waiver of written informed consent from the patients or their qualified next-of-kin because of the retrospective nature of the study.
Statistical analysis
Values are presented as a number (%), mean±standard deviation (SD), or median [interquartile range (IQR)], as appropriate. We compared the baseline characteristics, treatment modalities, time parameters, and imaging characteristics between the mild, moderate, and severe infarct expansion groups. Analysis of variance or Kruskal-Wallis test, χ2 test, and Fisher's exact test were used, as appropriate. The Spearman's rank correlation coefficient was computed between the ASPECTS difference and the CTA-CS. Variables achieving p-values less than 0.1 in the univariate analyses with an ordinal association and clinically important time variables were adjusted for using multivariate analyses (ordinal logistic regression analysis). Univariate analyses (independent sample t-test or Wilcoxon rank sum test for continuous variables, and χ2 test or Fisher's exact test for categorical variables) were also performed to compare the baseline characteristics, treatment modalities, time parameters, and imaging characteristics between the favorable and unfavorable outcome groups. Variables achieving p-values less than 0.1 in the univariate analyses for favorable outcomes were entered for multivariate analyses (binomial logistic regression analysis). Inter-rater agreements were assessed using linear weighted κ statistics. Statistical analyses were performed using the R Statistical Software. Results with a two-sided p-value <0.05 were considered statistically significant.
RESULTS
Baseline characteristics
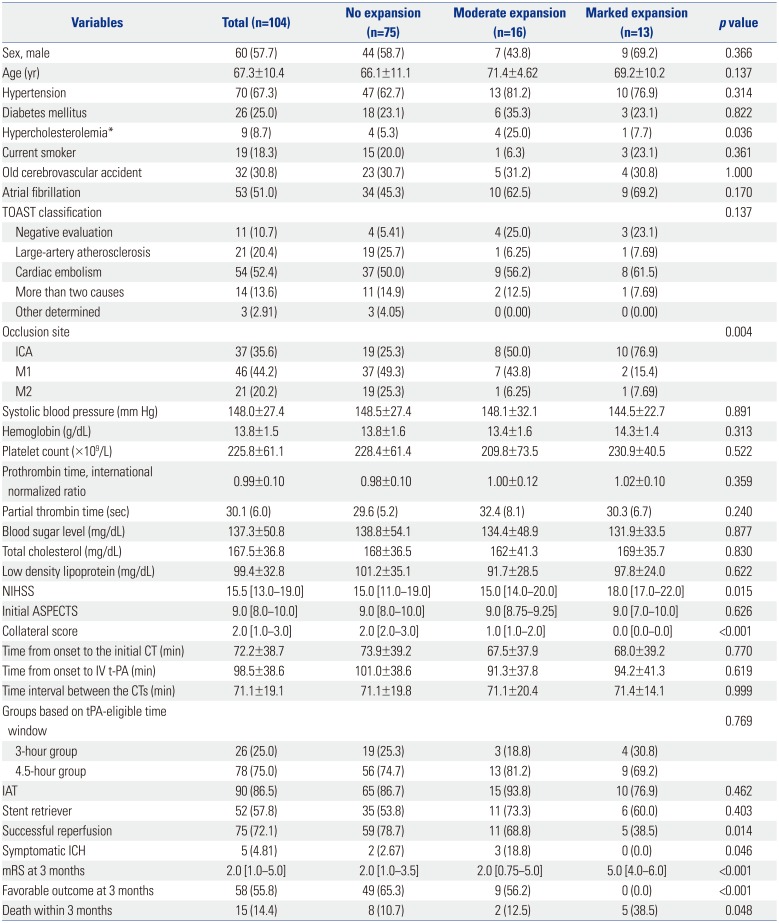
During the study period, 176 patients in the CT-based thrombus imaging cohort received IV t-PA treatment for an anterior circulation stroke with serial CT scans acquired before and after the IV t-PA treatment. After excluding 65 patients without proximal artery occlusion on CTA and seven patients with ASPECTS ≤6 on initial CT, 104 patients were included for this study. The mean age of the study patients was 67.3±10.4 years, and 60 (57.7%) of the patients were men. The median NIHSS score at admission was 16 (IQR, 13??9). Ninety (86.5%) patients were treated with combined IV t-PA and IAT, while 14 (13.5%) patients were treated with IV t-PA alone. The reasons for not performing IAT despite the presence of occlusion on CTA were rapid improvement of clinical symptom in eight patients, early ischemic change in more than one third of MCA territory in four patients, presence of hemorrhage on follow-up CT in one patient, and active tuberculosis in one patient. The primary modality used in the IAT was the stent retriever in 52 (57.8%) patients, intra-arterial urokinase infusion in 31 (34.4%) patients, modified thrombus suction using a Penumbra catheter in four (4.4%) patients, and carotid stent placement in three (3.3%) patients. Baseline characteristics of the study group appear in Table 1.
Infarct core expansion
Follow-up CT scans were obtained at 71.1±19.1 minutes after baseline CT scan. On the follow-up CT scan, 75 (72.1%) patients showed almost no infarct core expansion. However, 16 (15.4%) patients showed moderate and 13 (12.5%) patients showed marked infarct core expansion (Table 1). Although we excluded patients with a baseline ASPECTS <6, there were 16 (15.4%) patients who had ASPECTS <6 in the follow-up scan (Fig. 1). Inter-rater agreements for the expansion of the infarct core [linear weighted κ, 0.641; 95% confidence interval (CI), 0.485–0.797], ASPECTS (linear weighted κ, 0.666; 95% CI, 0.609–0.723), and CTA-CS (linear weighted κ, 0.625; 95% CI, 0.530–0.721) were all good.
Factors associated with infarct core expansion
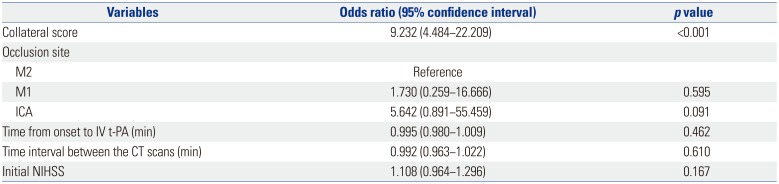
Univariate analyses revealed an association of the infarct core expansion with ICA occlusion, poor collateral status, and severe initial neurological deficits, but not with the time interval between the two consecutive CT scans. The proportion of patients with hypercholesterolemia was significantly higher in the moderate expansion group; however, there was no ordinal association between the history of hypercholesterolemia and infarct core expansion. In the ordinal logistic regression analysis, the infarct core expansion was significantly associated with collateral status (odds ratio, 9.232; 95% CI, 4.484–22.209; p<0.001) (Table 2). A significant correlation between the difference in ASPECTS on the consecutive CT scans, and CTA-CS (Fig. 2) (Spearman's rank correlation coefficient ρ=−0.733; p<0.001) was also noted.
Infarct core expansion and clinical outcomes
Fifty eight (55.8%) patients showed a favorable clinical outcome at 3 months. Infarct core expansion was associated with unfavorable clinical outcomes in the univariate (Supplementary Table 1, only online) and multivariate analyses after adjusting for confounding variables, such as sex, age, prothrombin time, time from onset to IV t-PA, initial NIHSS score, initial occlusion site, and successful reperfusion. None of the 13 patients with a marked expansion (≥4 point decrease in ASPECTS) of the ischemic core were independent at 3 months. In addition, only two out of the 16 patients with ASPECTS <6 on the follow-up CT showed a favorable clinical outcome. Although we could not perform multivariate analyses given the low numbers of symptomatic ICH and death events within 3 months, a significant association between infarct core expansion and symptomatic ICH and death within 3 months was observed in the univariate analyses (Table 1).
DISCUSSION
This study investigated the expansion of infarct core during IV t-PA treatment in patients with proximal artery occlusion. The study showed that 1) infarct core markedly expanded in about 12% of the patients with proximal artery occlusion at the end of IV t-PA infusion, 2) these patients had poor functional outcomes when they were treated with IAT after the infusion of IV t-PA, and 3) poor collaterals were predictive of a marked expansion of the infarct core.
IAT using a stent retriever is the treatment of choice in patients with intracranial proximal artery occlusion even if they already received IV t-PA treatment based on the recent results from randomized controlled trials.234,567,8 This study simulated the situation in which additional IAT is required after IV t-PA treatment, as we included patients who had proximal artery occlusion after IV t-PA. Indeed, the majority of the patients in this study population was treated with IAT. In patients who receive IAT on top of IV t-PA, IAT is sometimes performed after the infusion of IV t-PA is completed. However, our study demonstrated that infarct core could expand significantly during this time interval in some patients. In this study, 12% of the patients who did not have a large infarct core on the initial scan showed marked infarct core progression (decrease of ASPECTS ≥4). Despite a rescue IAT, none of these patients recovered to an independent life at 3 months. Although we do not know what the prognosis of these patients would be if they were to receive IAT as a combined therapy without waiting for completion of IV t-PA infusion or follow-up imaging, our results indirectly suggest that combined IAT with infusion of IV t-PA should be initiated as soon as possible and that patients who are expected to have infarct core expansion within an hour may not be an ideal candidates for combined IAT. While the poor outcomes in patients with infarct core expansion could be due to the higher failure of reperfusion in this group, the prognostic effect of infarct core progression was still significant after adjusting the successful reperfusion in the multivariate analysis.
We sought to identify factors associated with infarct core expansion and found that collateral status was one of its main associative factors. Collaterals are virtually the only source of blood supply in the presence of a proximal artery occlusion.1718 Collaterals help the tissues at risk to maintain their viability until final reperfusion is achieved. Previous studies have shown that the rate of infarct growth is determined by collateral status192021 and that better collateral status in the hyper-acute stage is associated with more favorable clinical outcomes.222324 The results of this study are in line with those of previous studies. Although the elapsed time would be another factor determining the infarct core expansion,192526 no definite association was observed between time between the two CT scans and the infarct core expansion in our study. This might be accounted for, in part, by the relatively constant time interval between the CTs, with a mean of ~70 minutes and an SD of ~14 minutes in this study. Nevertheless, our findings suggest that collateral blood supply might be more important than mere time.
We excluded patients who already have considerable infarct core in the initial imaging study (ASPECTS<6) based on recent clinical trial results811 because the primary aim of this study was to evaluate the infarct core expansion after the initial imaging. However, it should be acknowledged that the lack of evidence for clinical efficacy of IAT in patients with low ASPECTS does not necessarily mean that IAT should not be indicated in this group of patients. It is also difficult to provide specific suggestions regarding the use of collateral score in selecting an IAT candidate with this study because the patients in this study received IAT as a rescue therapy after waiting for IV t-PA response and that about 40% of the patients were not treated with a stent retriever, a currently standard modality of choice for IAT.8
There are several limitations to this study. First, occlusion sites and collateral scores were evaluated not in the initial imaging studies but in the follow-up studies after t-PA infusion because this study population was derived from the cohort for CT-based thrombus imaging. Since there is a slight chance of clot resolution and dynamic change of collateral status over the period of t-PA infusion, this should be considered as a limitation of our study. Second, patients who did not have proximal artery occlusion after IV t-PA treatment were not included in this study. Thus, the findings of this study cannot be applied to patients with successful recanalization after IV t-PA or those with distal artery occlusions. Third, while about 30% of patients had a history of previous stroke, data on pre-stroke mRS were not available. Therefore, this should be considered in the interpretation of outcome results. Finally, this study has a moderate sample size and a retrospective single-center design. Therefore, generalization of our results must be performed with caution.
In conclusion, our study revealed that some patients who received IV t-PA showed a rapid expansion of the infarct core during IV t-PA infusion, and they showed poor functional outcomes after rescue IAT. These patients with a rapid expansion of infarct core had poor collateral circulations. Our findings support the important role of collateral status for maintaining tissue viability and suggest that IAT should be started as soon as possible without waiting for completion of t-PA infusion.

 XML Download
XML Download