

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The 2012 revised International Chapel Hill Consensus Conference (CHCC) classifies systemic vasculitis affecting small vessels into two groups, immune complex small vessel vasculitis and antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV). AAV is also categorised into three variants comprising microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA, also called Wegener's granulomatosis), and eosinophilic GPA (EGPA, also called Churg-Strauss syndrome).1 Since MPA is not reflected in the classification criteria proposed by the American College Rheumatology (ACR),2 MPA is currently classified by 2012 CHCC and the 2007 European Medicines Agency (EMA) classification,3 which includes 1) no fulfilment of the ACR classification criteria for GPA or EGPA,45 2) clinical and histologic features compatible with small vessels vasculitis, 3) no GPA surrogate markers, 4) myeloperoxidase (MPO)-ANCA or proteinase 3 (PR3)-ANCA positivity, and 5) renal limited vasculitis.
In contrast to MPA, GPA and EGPA can be classified by the ACR classification criteria.45 GPA commonly affects respiratory tracts and kidneys, while EGPA is characterized by allergic features such as asthma and eosinophilia. The methods to evaluate the vasculitis activity of AAV includes Birmingham vasculitis activity score (BVAS),6 BVAS for GPA,7 disease extent index,8 and five factor score [FFS (1996) and FFS (2009)].910 Among them, BVAS or BVAS for GPA is the most widely used to assess the vasculitis activity of AAV.
Red blood cell (RBC) distribution width (RDW) is a routinely measured value of heterogeneity in the size of circulating RBCs. RDW is calculated from the coefficient of variation of RBC volume distribution as follows: RDW=standard deviation of RBC volume distribution/mean corpuscular volume (MCV)×100. RDW is clinically used to differentiate between different types of anaemia.11 When RDW is elevated, low MCV suggests iron deficiency, while high MCV implies folate or vitamin B12 deficiency and immune haemolytic anaemia. When RDW in normal, normal MCV favours chronic disease, while high MCV represents aplastic anaemia.11 Meanwhile, RDW has been considered to be associated with disease activity or prognosis of various inflammatory diseases including rheumatic diseases.12131415 To our best knowledge, there have been no reports regarding RDW in patients with AAV to date. Hence, in this study, we investigated whether RDW could predict not only vasculitis activity based on BVAS or BVAS for GPA at diagnosis, but also poor prognosis during follow-up in 150 patients with AAV.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the electronic medical records of 150 patients with AAV registered in the Severance Hospital Autoimmune Vasculitides cohort according to the following inclusion criteria:16171819 1) patients who had been initially diagnosed with MPA, GPA, or EGPA from October 2000 to January 2017 at the Division of Rheumatology, Department of Internal Medicine, Yonsei University College of Medicine, Severance Hospital; 2) patients who had been follow-up for more than 12 weeks after the first diagnosis of AAV in our institute; 3) patients who had fulfilled the 2012 revised CHCC or the 2007 EMA algorithm for MPA13 and who had met the ACR 1990 criteria for the classification for GPA and EGPA;45 4) patients who had the initial results of MPO-ANCA or PR3-ANCA, but not ANCAs by immunofluorescence assay [IFA, perinuclear (P)-ANCA and cytoplasmic (C)-ANCA], and those who did not have both ANCAs; 5) patients who had not been accompanied by any medical conditions that would influence the positivity of MPO-ANCA or PR3-ANCA or RDW;112021 6) patients who had never received medications for medical conditions mentioned above upon searching by the Korean Drug Utilization Review (DUR) system at diagnosis; and 7) patients whose medical records contained accurate descriptions enough to calculate BVAS or BVAS for GPA and FFS (1996) and FFS (2009) on the same day of blood collection for laboratory tests at diagnosis.67910 This study was approved by the Institutional Review Board of Severance Hospital (IRB no. 4-2017-0673).
Clinical and laboratory information
We collected age, gender, and the follow-up duration as demographic variables, and the follow-up duration was defined as the period from diagnosis to the date of the current study. Overall clinical items were similar between BVAS and BVAS for GPA, although detailed differed. Thus, we obtained organ-based clinical information, such as general, cutaneous, mucous membrane and eye, ear nose throat (ENT), cardiovascular, gastrointestinal, pulmonary, renal, and nervous systemic manifestations.67 Laboratory data included white blood cell, haemoglobin, RDW, prothrombin time (international normalised ratio), fasting glucose, blood urea nitrogen, creatinine, protein, serum albumin, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, total cholesterol, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).
Vasculitis activity and definition of severe GPA and disease course
The vasculitis activity of MPA and EGPA was assessed using BVAS and that of GPA was done using BVAS for GPA.67 Also, we searched clinical and laboratory features belonging to items of FFS (1996), as well as FFS (2009).910 In this study, the highest quartile of BVAS for GPA was 7 or greater, and we defined severe GPA as BVAS for GPA ≥7. We previously reported that BVAS ≥9.5 at diagnosis is associated with refractory disease in Korean patients with GPA.17 However, because we focused on the potential of RDW to reflect cross-sectional activity of GPA, rather than predict refractory disease of GPA, we set the cut-off of BVAS for severe disease at 7, the highest quartile of BVAS for GPA. Remission was defined as absence of disease activity attributable to active disease qualified by the need for on-going stable maintenance immunosuppressive therapy. Relapse was defined as recurrence or new onset of disease attributable to active vasculitis. Refractory disease was defined as unchanged or increased disease activity in acute vasculitis after 4 weeks of treatment with standard therapy or lack of response or chronic and persistent disease after over 12 weeks of treatment.22
ANCA measurement
MPO-ANCA and PR3-ANCA were measured by ELISA kits for anti-PR3 and anti-MPO (Inova Diagnostics, San Diego, CA, USA) before 2013, and by the novel anchor coated highly sensitive Phadia ELiA (Thermo Fisher Scientific/Phadia, Freiburg, Germany) using human native antigens, performed on a Phadia250 analyser after 2013.
Statistical analysis
Continuous variables are expressed as means±standard deviations, and categorical variables are reported as numbers (percentages). Correlations between RDW and other continuous variables were analysed by univariate Pearson's correlation analysis. Standardised correlation coefficients between BVAS for GPA and other continuous variables were assessed by multivariate linear regression analysis using variables with significant differences in univariate analysis. The optimal cut-off of RDW was extrapolated via calculating the area under the receiver operator characteristic curve (AUROC) and selected when the sum of sensitivity and specificity was maximised. In addition, relative risk (RR) of RDW under the initial BVAS for GPA ≥7 was evaluated using contingency tables and the chi square test. Significant differences in RDW between the presence and the absence of clinical manifestations and ANCA types were evaluated by the Mann-Whitney test. Due to the small number of subjects, we also applied univariate and multivariate Cox hazards models using variables with statistical significance to appropriately obtain RR. Kaplan-Meier survival analysis was used to analyse cumulative refractory disease free survival rate. All statistical analyses were conducted using SPSS software (version 23 for windows; IBM Corp., Armonk, NY, USA). p-values less than 0.05 were considered statistically significant.
RESULTS
Baseline characteristics of 150 patients with AAV
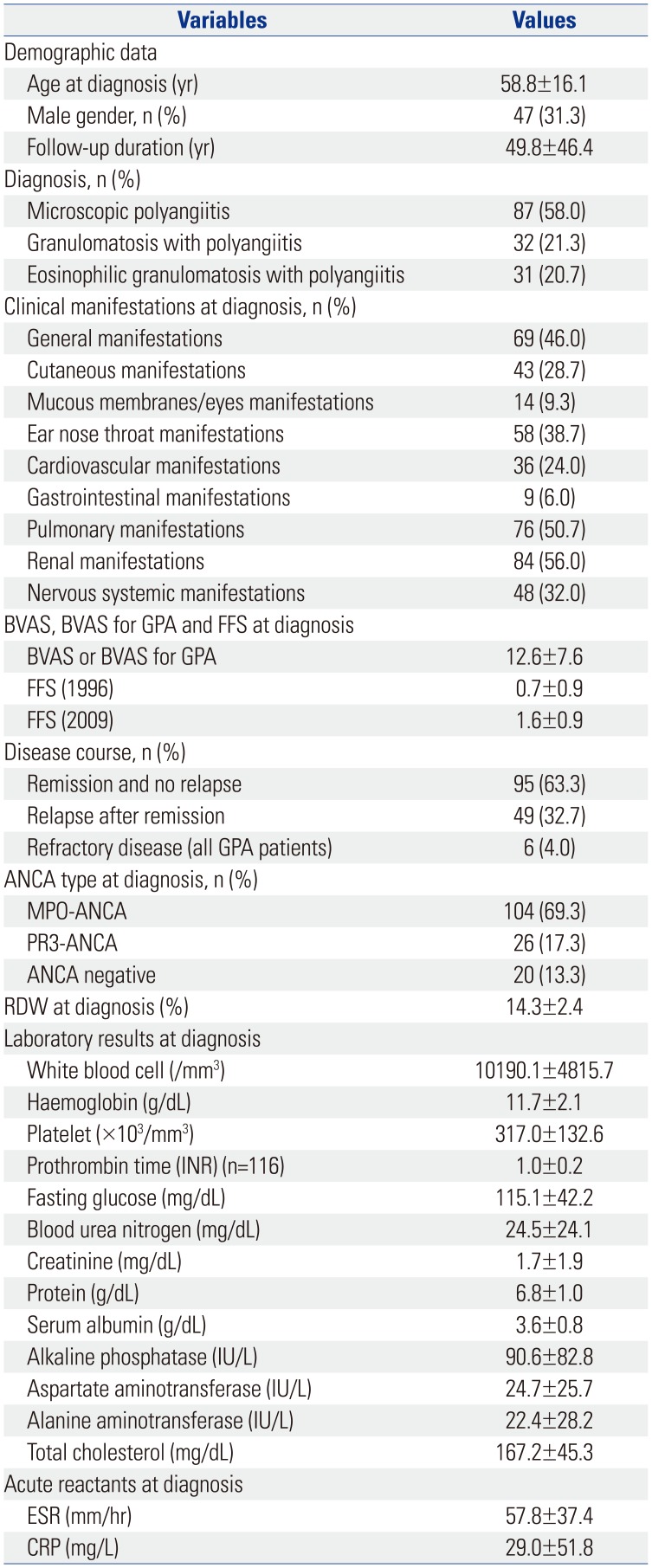
The baseline characteristics are described in Table 1. The mean age of the 150 patients [47 men (31.3%)] was 58.8 years old, and the mean follow-up duration was 49.8 months. Eighty-seven patients (58.0%) were classified as MPA, 32 (21.3%) as GPA, and 31 (20.7%) as EGPA. Renal manifestation (56.0%) was the most frequently observed manifestation at diagnosis, followed by pulmonary manifestation (50.7%), general manifestation (46.0%), and ENT manifestation (38.7%). The mean BVAS or BVAS for GPA was 12.6, and the mean FFS (1996) and FFS (2009) were 0.7 and 1.6, respectively. Ninety-five patients (63.3%) had achieved remission without relapse, while 49 patients (32.7%) had ever experienced relapse after remission. Also 6 patients (4.0%) with GPA had never achieved remission during the disease course. MPO-ANCA was detected in 104 patients (69.3%) and PR3-ANCA was found in 26 patients (17.3%). Twenty patients had neither MPO-ANCA nor PR3-ANCA. The mean RDW was 14.3%, and the mean ESR and CRP values were 57.8 mm/hr and 29.0 mg/L, respectively.
Correlation between RDW and other variables in all patients with AAV at diagnosis
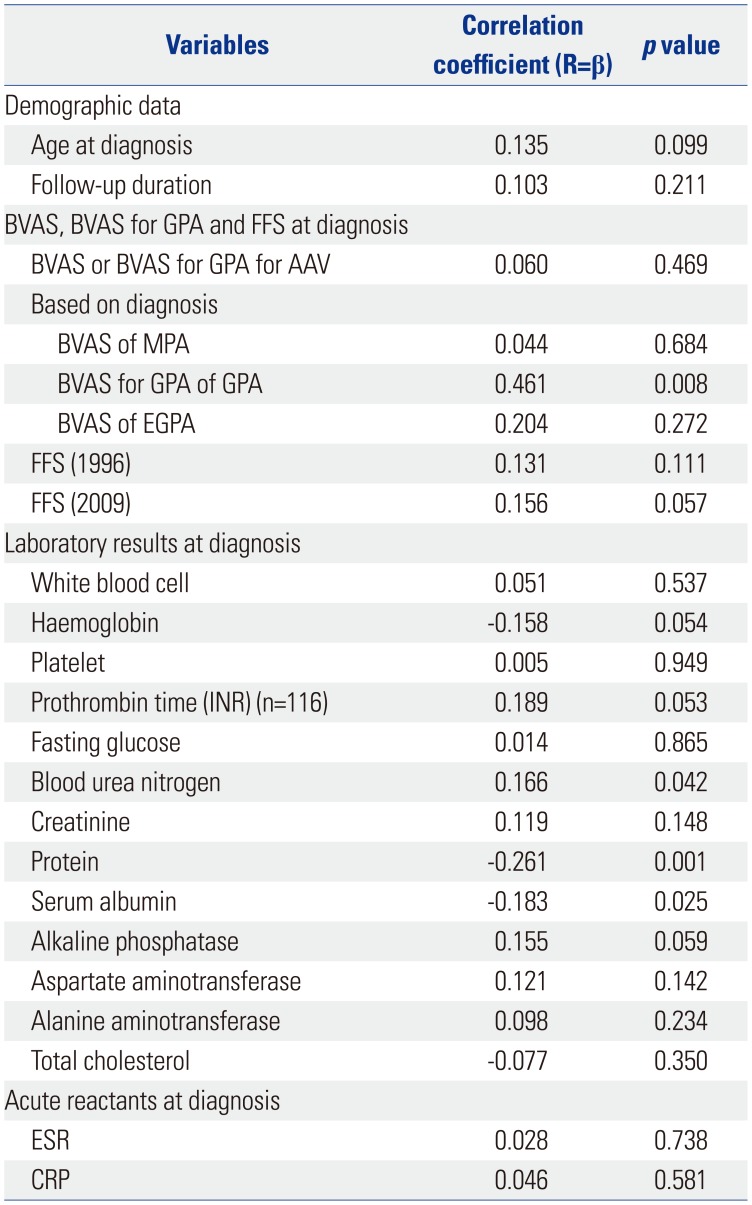
Overall, RDW was not correlated with BVAS or BVAS for GPA in all AAV patients. However, when we categorised them into each variant of AAV, RDW was significantly correlated with BVAS for GPA in only GPA patients (r=0.461, p=0.008). Among other laboratory results, RDW was negatively correlated with protein (r=-0.261, p=0.001) and serum albumin (r=−0.183, p=0.025) levels, while it was positively correlated with blood urea nitrogen (r=0.166, p=0.042). RDW tended to be correlated with haemoglobin, but was not significant. There was no significant correlation between RDW and ESR or CRP (Table 2).
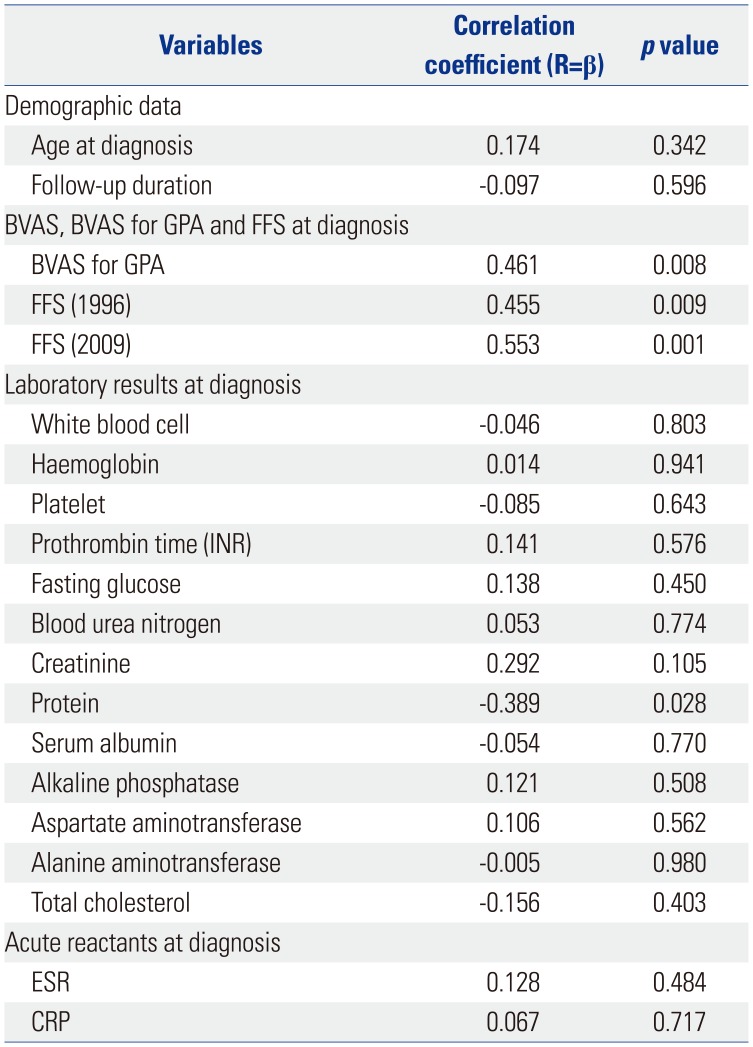
Correlation between RDW and other variables in patients with GPA at diagnosis
In GPA patients, RDW was significantly correlated with BVAS for GPA (r=0.461, p=0.008), and furthermore, it showed meaningful correlations with FFS (1996) (r=0.455, p=0.009) and FFS (2009) (r=0.553, p=0.001). Among other laboratory results, RDW was negatively correlated with protein (r=−0.389, p=0.028), but not with haemoglobin. Similar to all patients with AAV, GPA patients exhibited no remarkable correlation between RDW and ESR or CRP (Table 3).
Univariate and multivariate linear regression analyses of BVAS for GPA and other variables in patients with GPA at diagnosis
Univariate linear regression analysis showed that BVAS for GPA was significantly correlated with RDW (r=0.461, p=0.008), and inversely correlated with creatinine (r=0.349, p=0.049). BVAS for GPA was also positively correlated with FFS (1996) (r=0.734, p<0.001) and FFS (2009) (r=0.354, p=0.047). Because FFS (1996) and FFS (2009) items partly overlap with BVAS for GPA items, we did not include FFS (1996) and FFS (2009) in multivariate linear regression analysis. Multivariate linear regression analysis determined that RDW was the only independent predictor of BVAS for GPA [β=0.393, 95% confidence interval (CI) 0.041–0.584, p=0.025] (Table 4).
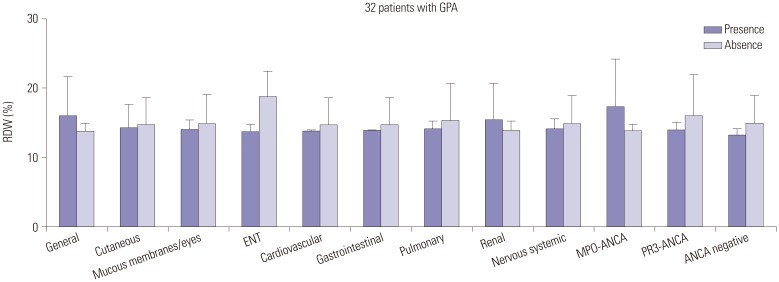
Comparison of RDW between the presence and absence of each clinical aspect and ANCA types in patients with GPA at diagnosis
Among organ-based clinical manifestations, only patients with ENT symptoms had a lower mean RDW than those without (13.9% vs. 19.0%, p=0.001). However, there was no significant difference in RDW between the presence and absence of PR3-ANCA (Fig. 1).
The optimal cut-off of RDW to predict severe GPA at diagnosis
In this study, we defined severe GPA as BVAS for GPA ≥7. We divided GPA patients into severe and not severe GPA groups according to it. Eleven patients were in the severe GPA group and 21 patients were in the not severe GPA group. The mean RDW of severe GPA group was higher than that of not severe GPA group (16.8% and 13.8%, p=0.032). We calculated the optimal cut-off of RDW to predict severe GPA, and we discovered that 15.4% was a strong predictor of severe GPA (AUROC 0.732, 95% CI 0.527–0.936, p=0.034; sensitivity 54.5% and specificity 95.2%) (Supplementary Fig. 1A, only online). We also reclassified the 32 GPA patients into two groups according to the optimal cut-off of RDW. Severe GPA (BVAS for GPA ≥7) was identified more frequently in patients having RDW ≥15.4% than those having RDW <15.4% (85.7% vs. 20.0%, p=0.001) (Supplementary Fig. 1B, only online). Furthermore, patients with RDW ≥15.4% had a significant higher risk of severe GPA than those without (RR 24.0, 95% CI 2.329–247.368).
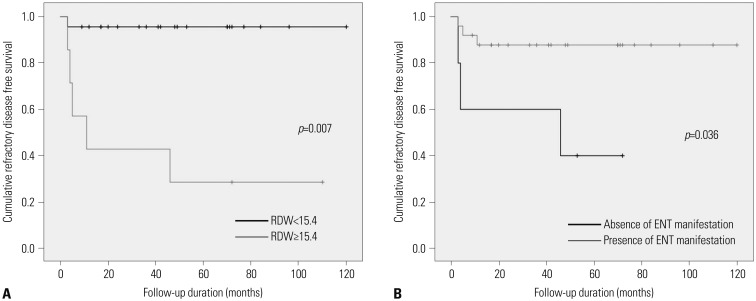
Predictors of prognosis during the follow-up duration
Since BVAS for GPA, FFS (1996), FFS (2009), and ENT symptoms were significantly related to RDW, we divided GPA patients into groups according to BVAS ≥7 or <7, FFS (1996) ≥1 or <1, FFS (2009) ≥1 or <1, RDW ≥15.4% or <15.4%, and the presence or absence of ENT manifestation based on our previous studies.161718 We used univariate and multivariate Cox hazards models to analyse the potential for predicting the prognosis of GPA in disease processes. In terms of relapse of GPA, there was no statistically significant predictor among them. In terms of refractory disease of GPA, univariate analysis showed that BVAS ≥7, FFS (1996) ≥1 and FFS (2009) ≥1 at diagnosis were not predicted thereof. Meanwhile, patients having RDW ≥15.4% and having no ENT symptoms at diagnosis exhibited a significantly increased risk of refractory GPA than those having RDW <15.4% and ENT manifestation (RR 19.527, 95% CI 2.271–167.905, and RR 0.177, 95% CI 0.035–0.890, respectively). Multivariate Cox hazards analysis showed RDW ≥15.4% to be the only significant predictor of refractory GPA (RR 17.573, 95% CI 1.701–181.586). There were significant differences in cumulative refractory disease free survival rates according to RDW ≥15.4% (p=0.007) and the absence of ENT manifestation (p=0.036) (Fig. 2).
DISCUSSION
In this study, we first demonstrated that RDW can predict vasculitis activity in patients with GPA. RDW was significantly correlated with BVAS for GPA in GPA patients, and furthermore, RDW was the only independent predictor of BVAS for GPA among other variables in multivariate linear regression analysis. We also found that an increase in RDW was associated with the absence of ENT symptoms, but not PR3-ANCA. In addition, we discovered that 15.4% of RDW was a strong predictor of severe GPA. Moreover, we found that patients having RDW ≥15.4% and having no ENT manifestation at diagnosis faced a significantly higher risk of refractory disease of GPA than those without these features during follow-up of at least more than 12 weeks. RDW ≥15.4% was the only significant predictor of refractory GPA in multivariate analysis. Taken together, we concluded that RDW can predict vasculitis activity of GPA and that RDW ≥15.4% at diagnosis not only increases the risk of severe GPA, but also predicts refractory diseases during follow-up.
RDW is clinically used to differentiate between different types of anaemia, particularly iron deficiency anaemia and anaemia of chronic disease.11 However, in this study, RDW was not significantly associated with haemoglobin. In order to reduce the effect of anaemia on the association of RDW with vasculitis activity of GPA, we excluded 5 patients with anaemia (haemoglobin<12.0 g/dL) and reanalysed the potential of RDW to predict vasculitis activity in 27 patients with GPA. RDW was positively correlated with BVAS for GPA, FFS (1996) and FFS (2009) and negatively correlated with protein (p<0.05 for all). However, RDW was not correlated with haemoglobin, ESR or CRP (Supplementary Table 1, only online). Univariate linear regression analysis showed BVAS for GPA to be significantly associated with RDW (r=0.470, p=0.013) and serum albumin (r=−0.388, p=0.045). Multivariate linear regression analysis revealed that RDW was the only independent predictor of BVAS for GPA (β=0.449, 95% CI 0.083–0.598, p=0.012) (Supplementary Table 2, only online). The highest quartile of BVAS for GPA for severe GPA was a score of 7 or greater, and therewith, the optimal cut-off of RDW to predict severe GPA was 13.7% (AUROC 0.735, 95% CI 0.522–0.946, p=0.045; sensitivity 80.0% and specificity 70.6%) (Supplementary Fig. 1C, only online). Patients with RDW ≥13.7% also had a significant higher risk of severe GPA than those without (RR 9.6, 95% CI 1.283–62.162) (Supplementary Fig. 1D, only online). However, RDW ≥13.7% could not predict refractory disease in GPA patients without anaemia. Taken together, we concluded that independent of concurrent anaemia, RDW can predict vasculitis activity of GPA at the same time, but not refractory disease during follow-up. Thus, in clinical settings, we suggest RDW ≥15.4% as a predictor of severe GPA and refractory disease development during the follow-up duration in GPA patients without anaemia.
In general, pro-inflammatory cytokines may be involved in the development of anaemia in a variety of diseases.23 In the early stage of GPA, large amounts of pro-inflammatory cytokines produced by macrophages and T cells, such as tumour necrosis factor-α and interleukin-6, stimulate and prime neutrophils, and primed neutrophils are subsequently activated by PR3-ANCA. Activated neutrophils migrate into adjacent tissues and predominantly induce inflammation primarily through innate immune responses. However, in the sclerotic progression stage of GPA, macrophages and autoreactive lymphocytes rather than activated neutrophils participate in the formation of pathergic necrosis and necrotising granulomatosis.24 Therefore, the effect of the pathophysiology of GPA on the development of anaemia at the time of diagnosis of GPA might be theoretically reduced compared to the early stage of GPA. The lack of correlation between RDW and ESR or CRP in this study might support this assumption. Furthermore, this explain about the discrepancy between this study and previous studies with relatively urgent diseases with much inflammatory burden including acute myocardial infarction, sepsis, and cancer.252627 We hypothesised that large amounts of pro-inflammatory cytokines may induce anaemia and increase RDW, along with ESR and CRP, in rapidly progressive inflammatory diseases, while small amounts of pro-inflammatory cytokines may induce subclinical anaemia and increase RDW, but not ESR or CRP in slowly progressive diseases like GPA. This hypothesis may be supported by our findings among which RDW was significantly associated with BVAS for GPA after excluding anaemic patients and RDW, instead of ESR and CRP, at diagnosis could predict refractory GPA during follow-up.
Since PR3-ANCA is known to play the most important role in the pathogenesis of GPA, it was thought that PR3-ANCA should be related to vasculitis activity of GPA. However, in this study, PR3-ANCA was not correlated with BVAS for GPA, and furthermore, it could not predict refractory disease during the follow-up duration. Although the significance of PR3-ANCA positivity in the rate of relapse or refractory disease of GPA has been debated, PR3-ANCA seems to be closely associated with poor prognosis in the disease course.282930 However, our study could not clarify the contribution of PR3-ANCA to poor outcome of GPA. Ethnic differences may affect differences in factors that affect the poor prognosis of GPA.31
In addition to RDW, RDW to platelet ratio has been recently reported to be associated with severity in several conditions.3233 We investigated the association between RDW to platelet ratio and vasculitis activity of GPA by univariable linear regression analysis. RDW to platelet ratio exhibited a tendency to be correlated with BVAS of GPA, but it was not statistically significant (r=0.325, 95% CI −3.230–78.145, p=0.070).
The strengths of our study are as follows: first, we first demonstrated that RDW is the only independent predictor of BVAS for GPA. Second, we first suggested the optimal cut-off of RDW to predict severe GPA (the highest quartile of BVAS for GPA) and demonstrated that the optimal cut-off of RDW at diagnosis reflects an increased risk of refractory disease in GPA patients during follow-up. Our study also had several limitations. First, the optimal cut-off of RDW to predict severe GPA was changed according to the presence of anaemia, which might reduce the clinical usefulness of RDW in clinical settings. Second, serial measurements of RDW and BVAS for GPA were not available. Third, this study has limitations as a retrospective study, with a small number of patients with GPA. If future studies can prospectively enrol a larger number of GPA patients and serially measure RDW and BVAS for GPA, they may reveal a dynamic correlation between RDW and vasculitis activity of GPA, and propose more reliable factors with which to predict the prognosis of GPA.
In conclusion, RDW may be an independent predictor of BVAS for GPA regardless of anaemia, and predict refractory disease of GPA during follow-up in patients without anaemia. Therefore, we suggest that general physicians can use RDW of more than 15.4% as a predictor of high vascular activity and poor prognosis in patients with GPA.

 XML Download
XML Download