

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The fibroblast growth factor (FGF) family consists of 22 members with various biological functions, such as cell growth, development, angiogenesis, and wound healing.1 Among these members, FGF21 is primarily isolated from liver tissue and has recently been shown in animal models to have beneficial effects on glucose and lipid metabolism and insulin sensitivity.12 In human studies, high serum FGF21 levels have been observed in obese participants with insulin resistant states, such as dyslipidemia, coronary artery disease, non-alcoholic fatty liver disease, and polycystic ovarian syndrome.1345
Since multiple, favorable FGF21 effects on glucose and lipid metabolism and insulin sensitivity have been reported, FGF21 might be a biomarker that influences metabolic syndrome (MetS) and type 2 diabetes (T2DM) pathophysiology.36 It may also be a therapeutic agent for treating diabetes and other obesity-related metabolic disorders.5 FGF21 has also been shown to be a potent metabolic regulator.5789 In addition, research has shown that increased FGF21 levels are associated with MetS in Asian individuals.1011 Another report showed an association between genetic polymorphisms located within the FGF21 3′-untranslated region and the incidence of MetS in an Asian cohort study.12
MetS includes impaired glucose regulation, abdominal obesity, dyslipidemia, and high blood pressure. It is estimated that approximately one-fourth of the world's adult population suffers from MetS.2 MetS is a significant factor leading to a higher risk of cardiovascular disease and T2DM. MetS is distinguished by an atherogenic dyslipidemia comprising increased very low-density lipoprotein (VLDL), triglycerides (TG), decreased high-density lipoprotein (HDL)-cholesterol, and a predominance of small dense low-density lipoprotein (LDL) particles.13 Additionally, the Korean National Health and Nutrition Examination Survey reported the prevalence of MetS to account for about one-third of the total Korean population.1014 Because serum FGF21 levels have been implicated as a potential predictor for the early detection of MetS, we investigated the correlation between serum FGF21 level and the incidence of MetS in a population-based prospective study. However, no prior investigations have reported an association between serum FGF21 levels and the incidence of MetS in Korean longitudinal studies. Therefore, we hypothesized that high serum FGF21 levels would be a predictor for new-onset MetS.
MATERIALS AND METHODS
Study population
This prospective study was conducted using data from the Korean Genome and Epidemiology Study on the Atherosclerosis Risk of Rural Areas in the Korean General Population (KoGES-ARIRANG). We selected 221 random participants from this study. The Institutional Review Board of Wonju Christian Hospital approved the study design (IRB No. CR105024). All participants provided written informed consent to take part in this study. Further inclusion criteria included the absence of any other disorder or medication known to affect serum FGF21 level.
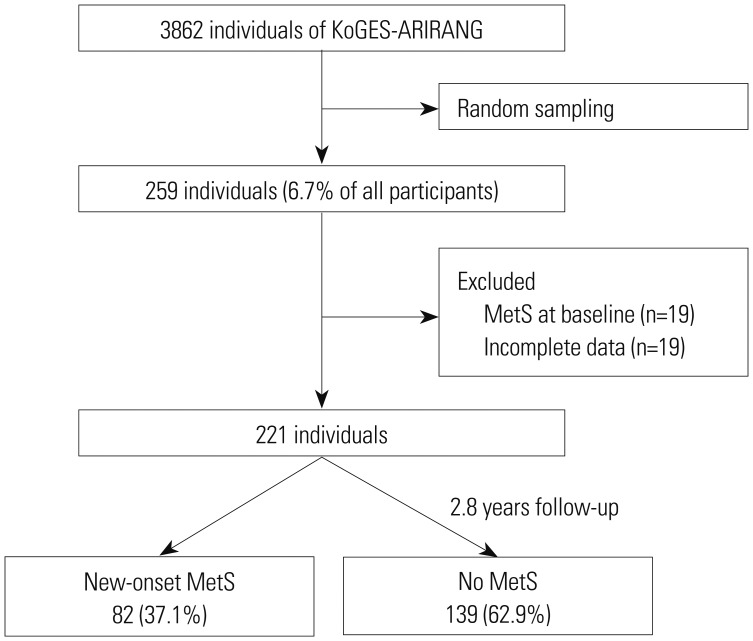
The KoGES-ARIRANG included participants from 40–70 years of age who resided in the Wonju and Pyengchang areas of the Republic of Korea. The baseline survey conducted from November 2005 to January 2008 included 5178 adults (2127 men and 3051 women). In the first follow-up survey (April 2008 to January 2011), 3862 people participated therein (74.6%). We randomly selected 259 individuals (6.7%) from these 3862 patients. We excluded 19 participants who were diagnosed with MetS at baseline and 19 participants with incomplete data, which left 221 participants without MetS, who comprised the final sample (Fig. 1).
Anthropometric and biochemical measurements
At baseline and follow-up examinations, study participants completed a standardized medical history and lifestyle questionnaire, as well as a comprehensive health examination that followed standard procedures. Clinical phenotypes for all participants, including weight, height, and waist circumference (WC), were assessed using a tape measure on a horizontal plane midway between the inferior margin of the ribs and the superior border of the iliac crest (SECA-200, SECA, Hamburg, Germany). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were taken twice using a standard mercury sphygmomanometer (Baumanometer, Copiague, NY, USA). Participant smoking status was also recorded.
A venous blood sample was obtained from the study populations following an overnight fast. Serum aliquots were stored at −80℃ until ready for further analysis. Fasting glucose was determined using a glucose oxidase-based assay, and fasting insulin was measured using a double-antibody radioimmunoassay RIA (Biosource, Belgium). Serum concentrations for LDL cholesterol, HDL cholesterol, and TG were analyzed with enzymatic methods (Advia 1650, Siemens, Tarrytown, NY, USA). Degree of insulin resistance was evaluated using the homeostasis model assessment of insulin resistance (HOMA-IR) as follows: fasting insulin (µIU/mL)×fasting plasma glucose (mg/dL)/405.
Serum FGF21 levels were assessed with a sandwich enzyme-linked immunosorbent assay (ELISA) (FGF-21 ELISA Kit, Cat. No. AG-45B-5001-KI01; Adipogen, Switzerland) according to the manufacturer's instructions. All of the serum samples were assayed in duplicate, and the mean value of the two measurements was used for analysis. A blood sample was obtained from the study participants following an overnight fast, and serum aliquots were stored at −80℃ until ready for further analysis. Median FGF21 levels were 113.21 with an interquartile range (IQR) of 123.7 (Q3–Q1=177.87–54.17). The ranges for each quartile were Q1 (≤54.17), Q2 (54.17–113.21), Q3 (113.21–177.87), and Q4 (≥177.87).
Endpoint
In accordance with previous studies,15 MetS was defined as the presence of at least three of the following components: 1) abdominal obesity or a WC ≥90 cm for men or ≥85 cm for women (following the Korean-specific cutoffs for abdominal obesity set by the Korean Society of Obesity);16 2) hypertriglyceridemia or a serum TG concentration ≥150 mg/dL (1.69 mmol/L); 3) low HDL cholesterol or a serum HDL cholesterol concentration <40 mg/dL (1.04 mmol/L) for men or <50 mg/dL (1.29 mmol/L) for women; 4) high blood pressure, an SBP ≥130 mm Hg, a DBP ≥85 mm Hg, or treatment with antihypertensive agents; and 5) high fasting glucose, a fasting serum glucose ≥100 mg/dL, or previously diagnosed T2DM.
Statistical analysis
Multivariate logistic regression was used to assess independent associations between baseline FGF21 levels and the presence of new-onset MetS. We used two models with progressive degrees of adjustment. First, we conducted an age- (continuous variable) and gender- (nominal variable: male and female) adjusted analysis. We then further adjusted for baseline levels of body mass index (BMI, continuous variable), LDL cholesterol (continuous variable), smoking status (nominal variable: current/former/never), and regular exercise (nominal variable: yes/no). Results are expressed as odds ratios (ORs) with 95% confidence intervals (CIs). All analyses were performed using the Statistical Package for the Social Sciences software, version 21.0 (IBM Corp., Armonk, NY, USA). p-values <0.05 were considered statistically significant.
RESULTS
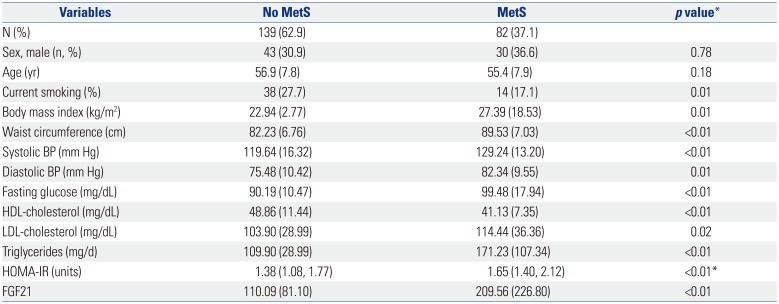
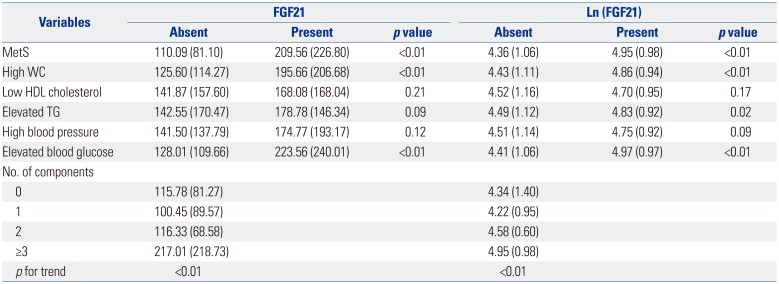
Over 2.8 years of follow-up, 82 (37.1%) new MetS cases were diagnosed. Initial BMI, WC, SBP, DBP, fasting glucose, TG, LDL, and HOMA-IR were significantly higher, while HDL cholesterol was significantly lower, in those who had developed MetS than in those who did not. The mean FGF21 level at baseline was significantly higher in individuals who developed MetS than in those who did not (209.56±226.80 vs. 110.09±81.10, p<0.01) (Table 1). Similar associations were observed between serum FGF21 level and each MetS component. Furthermore, serum FGF21 progressively increased as the number of MetS components increased over the follow-up period (all p for trend: <0.01) (Table 2).
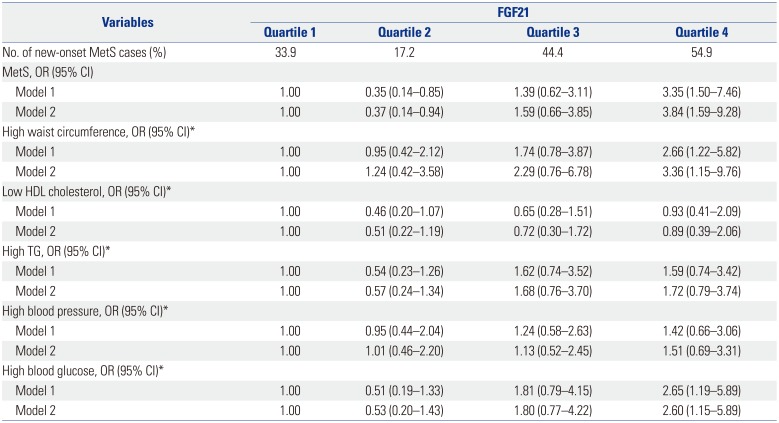
Multivariate regression models adjusted for baseline BMI, LDL cholesterol, smoking, and regular exercise revealed a significant association between serum FGF21 levels and the presence of new-onset MetS (model 2) (Table 3). The OR for MetS development was 3.84 (95% CI: 1.59–9.28) for the highest serum FGF21 quartile. Corresponding ORs (95% CI) for high WC, low HDL cholesterol, high TG, high blood pressure, and high blood glucose were 3.36 (1.15–9.76), 0.89 (0.39–2.06), 1.72 (0.79–3.74), 1.51 (0.69–3.31), and 2.60 (1.15–5.89), respectively. Receiver operating characteristic curves for FGF21 levels were drawn to predict the presence of MetS in Korean adults (AUC=0.650, p<0.001) (data not shown).
DISCUSSION
In this prospective study, we investigated whether increases in FGF21 are significantly associated with a higher risk of new onset MetS (OR: 3.84, 95% CI: 1.59–9.28). We noted a significant and progressive elevation in serum FGF21 levels as the number of MetS components increased among study participants over the follow-up period. Therefore, we suggest that high serum FGF21 levels might be a diagnostic predictor for MetS development. This study may be the first prospective epidemiological study to explore the association between serum FGF21 level and new-onset MetS in a Korean population.
Many animal and clinical studies have emphasized the role of FGF21 in promoting metabolic disease development and progression.5 FGF21 was initially identified as a factor that increased glucose uptake in mouse 3T3-L1 and primary human adipocytes.5 In general, FGF21 has been found to be a metabolic regulator with potential anti-diabetic effects in studies using high throughput screening for agents efficient at increasing glucose uptake by 3T3-L1s.12 Recent studies have demonstrated that FGF21 is up-regulated by peroxisome proliferator-activated receptor-α (PPARα) in animal and human liver tissue and by proliferator-activated receptor-γ (PPARγ) in adipose tissue.1171819 FGF21 expression and secretion is induced in the liver during fasting, and fatty acids promote the expression and secretion of FGF21 in a PPAR-α-dependent manner.3 Furthermore, research has suggested a prominent synergy between FGF21 and the antidiabetic agent rosiglitazone, a PPAR-γ agonist, in stimulating glucose uptake.20 FGF21 signaling is mediated by the FGF receptor and the adapter molecule β-Klotho, whose expression is induced during adipogenesis.13 FGF21 has also been demonstrated to enhance pancreatic β-cell function and survival through the activation of extracellular signal-related kinase 1/2 and the Akt signaling pathway.21 Consequently, FGF21 signaling has been suggested to influence glucose, lipid, cholesterol, and bile acid mechanisms, transforming FGF21 into a plausible candidate that may directly affect MetS and T2DM pathophysiology.318 Therefore, several effects of FGF21 on glucose and lipid metabolism and insulin sensitivity have indicated that FGF21 could be used as a therapeutic agent for diabetes and other obesity-related MetS conditions.22
In this prospective study, we investigated elevated serum FGF21 levels in patients with MetS in comparison to control participants without MetS (Table 1) in a manner that was similar to those used in previous studies. Patients with coronary artery disease demonstrated significantly higher plasma FGF21 levels, which were positively associated with total serum cholesterol, TG, and HDL levels.232425 Recent results have shown that serum FGF21 levels are independently and significantly increased in participants with higher TG levels or a higher SBP in Japanese individuals.4 Additionally, serum FGF21 levels were significantly associated with SBP: a similar result was also found in this study (Table 3). Because factors such as TG and SBP are associated with MetS, these reports suggest that serum FGF21 levels could be a biomarker predicting metabolic disorders related to MetS.4 Compared to previous cross-sectional observations, a prospective cohort study similar to this study will likely be required to confirm FGF21 level as a predictor for metabolic disorders associated with MetS components, as well as MetS itself.8
Upon logistic regression analysis, participants in the second quartile of serum FGF21 had an OR of 0.35 (95% CI: 0.14–0.85, p<0.0001) for the association with MetS, compared to participants in the lowest quartile for serum FGF21 (Model 1) (Table 3). This OR remained statistically significant even after adjusting for potential confounders; however, this result also demonstrated a negative association between serum FGF21 levels and MetS (Table 3). Because previous studies have suggested that endoplasmic reticulum (ER) stress in the cell may contribute to obesity-associated metabolic disease and that FGF21 expression is elevated in obese patients and mouse models of obesity, prior studies have investigated the pathophysiological function of FGF21 in ER stress and metabolic alterations in obese mice.262728 Recently, Kim, et al.26 observed that FGF21 plays a crucial role in the adaptive response to ER stress- or obesity-induced hepatic metabolic stress, and also demonstrated that FGF21 induction plays a protective role in obesity-related ER stress and metabolic aggravation. This might be due to the protective effect of increasing FGF21 levels, to a certain extent, on MetS, although increased FGF21 might reflect FGF21-resistance.2930 Similar to this study, Bobbert, et al.3 suggested FGF21 is an independent predictor of MetS and T2DM in apparently healthy Caucasians, and these results may indicate FGF21 resistance precedes the onset of MetS and T2DM. There are some data in cross-sectional human studies showing a positive correlation between FGF21 values and obesity, T2DM, or MetS. Nevertheless, the pathophysiologic effects of FGF21 on glucose lipid metabolism are not well understood, especially because initial animal and in vitro studies proposed glucose-lowering effects and improved fat metabolism. We assumed that lower FGF21 serum expression had no role in obesity-related ER stress and metabolic effects; therefore, metabolic alterations were likely responsible for MetS in participants from the second quartile. However, no prior prospective studies have examined the development of MetS or performed a quantitative or qualitative analysis of FGF21 expression levels. As a result, it was difficult to predict the correlation between serum FGF21 level and the incidence of MetS in our follow-up cohort. Therefore, based on the results of this population-based prospective cohort study, it was reasonable to suggest that alterations in FGF21 level are surrogate markers for new-onset MetS.
This study had some limitations. Results were based on a single FGF21 level measurement, which was subject to random measurement errors, and may have undervalued correlation strength. The sample size was relatively small, and the follow-up period was short (only 2.8 years). Therefore, we could not estimate whether the association between serum FGF21 level and new-onset MetS would have been maintained over a longer period. Our findings may not be generalizable to other populations, especially different ethnicities, with higher levels of obesity or younger mean age. Additionally, we found no sufficient references to corroborate the association between serum FGF21 level and MetS onset found in this study.
In conclusion, this prospective cohort study demonstrated that FGF21 may be a significant biomarker predicting the development of MetS. MetS is a condition predicting risk of diabetes, hypertension, and dyslipidemia, which together become risks of atherosclerotic diseases. MetS has been shown to be associated with mitochondrial dysfunction, and FGF21 signaling has been suggested to influence glucose, lipid, cholesterol and bile acid mechanisms, transforming FGF21 into a plausible candidate that may directly affect MetS and T2DM pathophysiology. Therefore, FGF21 could potentially be of use as a therapeutic agent for diabetes and other obesity-related MetS conditions. Future biological mechanism studies should investigate MetS pathogenesis with respect to the bioenergetics pathway, including FGF21 signaling, in metabolic regulation. These future studies should provide new insights into the role of FGF21 as a biomarker for MetS management and suggest FGF21-based therapies that may effectively treat MetS.
 XML Download
XML Download