

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common sustained arrhythmia, which reduces the quality of life, and is mainly associated with the major complication of stroke.12 Current practical guidelines recommend a risk-stratified approach using only oral anticoagulation treatment (OAC) based on CHA2DS2-VASc scores for the prevention of stroke occurrence.23 In a meta-analysis, warfarin significantly reduced the risk of stroke occurrence,456 and a new OAC had an additional significant benefit of reducing stroke occurrence, compared with warfarin.6 However, principally, a restored and maintained sinus rhythm with reduced AF burden is expected to reduce the risk of stroke and to offer good prognosis.7 Nevertheless, the superiority of rhythm control over the rate control strategy for AF management has not been proven as having a preventive effect for the occurrence of stroke.891011 A few studies have shown that the rhythm control strategy is associated with favorable outcomes and a significantly lower risk of stroke1213 beyond symptomatic care in AF treatment. Therefore, we investigated whether the rhythm control strategy prevents the occurrence of stroke and has more favorable outcomes, compared with the rate control strategy, in patients with AF in a prospective national cohort that adhered to current guidelines.
MATERIALS AND METHODS
Study design and enrolled patients
The COmparison study of Drugs for symptom control and complication prEvention of Atrial Fibrillation (CODE-AF) is a prospective, multicenter, observational study performed at 10 tertiary centers that encompass all geographical regions of Korea. The aim of the CODE-AF registry is to describe the clinical epidemiology of patients with AF and to determine the diagnostic and therapeutic processes (including the organization of programs for AF management) applied to these patients and their clinical outcomes. The registry was designed and coordinated by the Korea Heart Rhythm Society, which provides support to related committees, national coordinators, and participating centers. Data are entered into a common electronic database that limits inconsistencies and errors and provides online help for key variables. Each center can see its own data and data from all other participating centers. The study was approved by the ethics committee of each center (EMC 2016-05-003), and all patients provided informed consent for their inclusion. This study was registered at www.ClinicalTrials.gov (NCT02786095).
From June 2016 to April 2017, each center started to prospectively enroll 6000 patients with nonvalvular AF who were >18 years of age, attended an outpatient clinic, and were hospitalized on the same day for AF. Of these, 2508 (41.8%) patients were clinically followed up for over six months (Supplementary Fig. 1, only online). Finally, the CODE-AF enrolled patients who were clinically followed up consisted of 1134 (45.2%) patients treated with the rhythm control strategy and 1374 (54.8%) patients treated with the rate control strategy.
The CHA2DS2-VASc and Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile international normalized ratio, Elderly, Drugs/alcohol concomitantly (HAS-BLED) scores were calculated for all patients with nonvalvular AF. Chronic kidney disease was defined as a glomerular filtration rate less than 60 mL/min/1.73 m2 according to the Chronic Kidney Disease Epidemiology Collaboration.14
Oral anticoagulation strategy
According to the 2016 European Society of Cardiology and 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines for patients with AF,215 AF patients without clinical stroke risk factors are not to undergo antithrombotic therapy, whereas patients with stroke risk factors (i.e., a CHA2DS2-VASc score of 1 and 2 for men and women, respectively) are recommended to be prescribed OAC.
Rhythm and rate control strategies
For the rate-control strategy of AF treatment, beta-blockers, digoxin and diltiazem, or verapamil were selected to control the heart rate in patients with AF. For the rhythm control strategy of AF treatment, dronedarone, flecainide, propafenone, sotalol, and amiodarone were selected to maintain the sinus rhythm according to structure heart disease. For active rhythm control, electrical cardioversion and catheter ablation were considered in selected patients231617 at each center.
Clinical outcome
A follow-up visit was scheduled every 6 months, and a personal interview by phone was planned for those who could not make the follow-up visit, although no actual phone interviews were conducted during the study. We assessed the following outcomes at follow up: 1) all-cause death, 2) hospitalization, 3) myocardial infarction, 4) stroke, systemic embolization, or transient ischemic attack, and 5) bleeding.
Definition of bleeding
Major bleeding was defined as fatal bleeding, symptomatic bleeding in a critical area or organ, and bleeding causing a decline in hemoglobin level of 20 g/L or more or leading to transfusion of two or more units of whole blood or red cell.18 Non-major bleeding was defined as any sign or symptom of hemorrhage, including bleeding found by imaging alone, which does not fit the criteria for major bleeding.19
Statistical analysis
Continuous variables are expressed as means±standard deviations, and categorical variables are reported as frequencies (percentage). Multivariable Cox regression hazard models were constructed to assess the independent relationship of stroke and clinical outcomes adjusting for demographic variables. Statistical analyses were performed using SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA) and MedCalc (MedCalc software, version 12.3, Acacialaan, Ostend, Belgium). A p value <0.05 was considered statistically significant.
RESULTS
Baseline characteristics
AF patients treated with the rhythm control strategy were younger than those treated with the rate control strategy (65±10 vs. 70±10, p<0.001), and the proportions of men were 64.9% and 60.1%, respectively.
AF patients treated with the rhythm control strategy more frequently had hypertension, symptomatic paroxysmal AF, a shorter duration, electrical external cardioversion, and experienced catheter ablation, compared to those treated with the rate control strategy. However, AF patients treated with the rate control strategy more frequently had diabetes, dyslipidemia, chronic kidney disease, heart failure, and a larger left atrium size than those treated with the rhythm control strategy. The CHA2DS2-VASc score for patients treated with the rhythm control strategy was lower than in those treated with the rate control strategy (2.4±1.5 vs. 3.1±1.7, p<0.001) (Table 1).
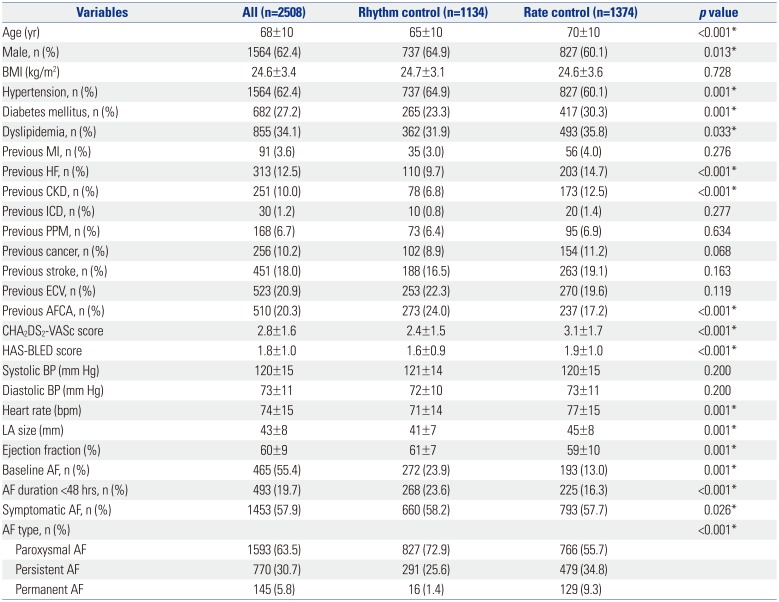
Table 1
Comparison of the Baseline Characteristics of Patients Treated with the Rhythm and the Rate Control Strategy
BMI, body mass index; MI, myocardial infarction; HF, heart failure; CKD, chronic kidney disease; ICD, intracardiac defibrillator; PPM, permanent pacemaker; ECV, electrical cardioversion; AFCA, atrial fibrillation catheter ablation; BP, blood pressure; LA, left atrium; AF, atrial fibrillation.
Data are presented as a mean±standard deviation or number (percentage).
*Statistically significant.
![]()
Oral antithrombotic agents and rate and rhythm control
The majority of patients were treated with one or more antithrombotic agents. Warfarin and a new OAC (17.3% vs. 57.8%) were the most prescribed antithrombotic agents, followed by an anti-platelet agent, all of which were similarly prescribed in both groups (Supplementary Table 1, only online). In the rate control strategy group, beta-blockers were the most commonly prescribed medication, followed by non-hydropyridine calcium channel blockers and digoxin. In the rhythm control strategy group, flecainide was the most commonly prescribed medication, followed by amiodarone and propafenone (Table 2).
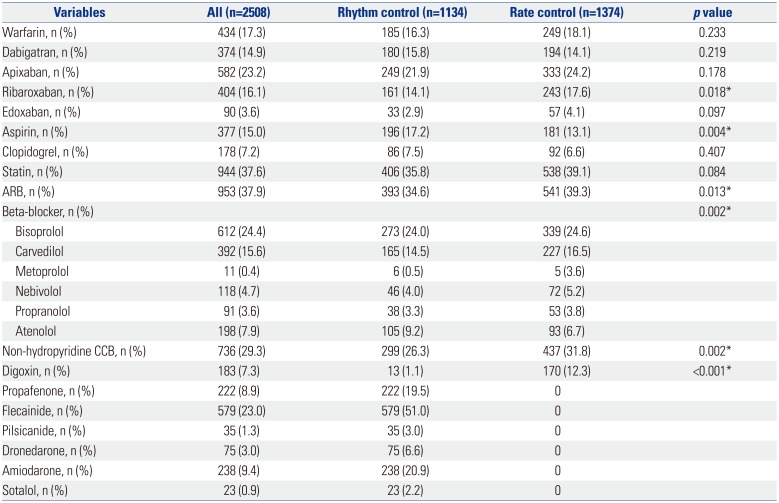
Table 2
Comparison of Treatments in the Rhythm and the Rate Control Strategy Groups
![]()
Comparison of clinical outcomes between the rate control and the rhythm control groups
The mean follow-up durations were 5.9±1.2 and 5.8±1.2 months in the rhythm control and the rate control groups, respectively. Significantly more patients treated with the rhythm control strategy maintained a sinus rhythm than those treated with the rate control strategy (73.2% vs. 31.6%). Clinical outcomes including hospitalization, myocardial infarction, and death and bleeding were similar between all patients treated with rhythm control and with rate control. However, the incidence of stroke in the rhythm control group was 0%, compared with 0.7% in the rate control group (p=0.015).
In Cox regression analysis, although non-rhythm control was associated with a higher risk of stroke [hazard ratio (HR) 9.04; 95% confidence interval (CI), 1.15−70.6] in univariate analysis, it was not associated with higher risk of stroke (HR 0.27; 95% CI, 0.03−2.33) in the multivariate analysis.
DISCUSSION
Main findings
In our study with an AF prospective cohort, although non-rhythm control was significantly associated with stroke in univariate analysis, it was not significantly associated with stroke in multivariate analysis.
Comparison of differences between the rate and the rhythm control strategies for cardiovascular mortality
Several trials have demonstrated that the rhythm control strategy offers no benefit on cardiovascular mortality in patients with AF, compared with the rate control strategy, and two meta-analyses reported overall risk ratios of 0.95 (95% CI 0.76−1.19) and 1.15 (95% CI 0.15−1.88).89202122 These negative results for the rhythm control strategy have been attributed to the inefficiency of the antiarrhythmic drugs to maintain a sinus rhythm and to the fact that the beneficial effects of antiarrhythmic drugs are offset by their adverse effects.7 Unlike previous designed rhythm control in AF treatment, our study showed that an active rhythm control strategy that included electrical cardioversion or catheter ablation applied to medically refractory AF patients or to patients with antiarrhythmic drug-related adverse events minimized the need for antiarrhythmic drugs and hence prevented antiarrhythmic toxicities. In real practice with guideline adherence,21523 a physician considers the optimal choice among the use of antiarrhythmic drugs and catheter ablation to minimize risk and to maximize benefits in order to restore and maintain a sinus rhythm. However, in our study, even though the rhythm control strategy group was younger, had a smaller proportion of heart failures and chronic kidney diseases, and was significantly superior for maintaining a sinus rhythm at follow-up (73.2% vs. 31.6%, p<0.001), the rhythm control strategy exhibited no benefit for cardiovascular mortality, compared with the rate control strategy, over a short-term follow up duration, as has been previously reported.81122
Comparison of differences between the rate and the rhythm control strategies for stroke
Two meta-analyses comparing the pharmacological rhythm and the rate control strategy reported that the incidence of stroke was found to be statistically similar between the two groups with an overall odds ratio of 0.99 (95% CI 0.75−1.30) and a risk ratio of 0.96 (95% CI 0.68−1.34).822 However, recent studies have demonstrated that the rhythm control strategy including catheter ablation was associated with lower rates of stroke among patients with AF.121324 This reduced risk of stroke associated with an optimal rhythm control including catheter ablation was implicated to maintain a sinus rhythm and to reduce the burden of AF.11225 In our study, patients with the rhythm control strategy showed a significantly lower risk of stroke, compared with those with the rate control strategy [1 (0%) vs. 10 (0.7%), p=0.015], at the short-term follow-up duration (Table 3). However, rhythm control group was associated with better prognosis due to better patient baseline characteristics in the rhythm control group (Tables 1 and 4).
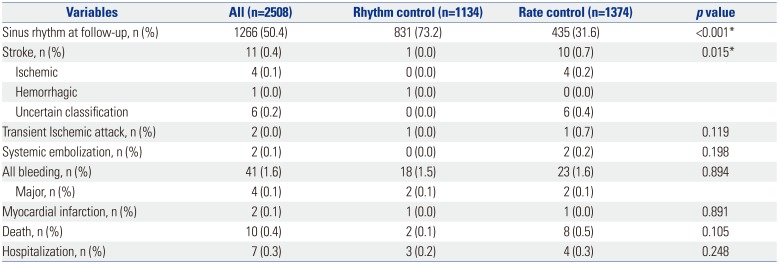
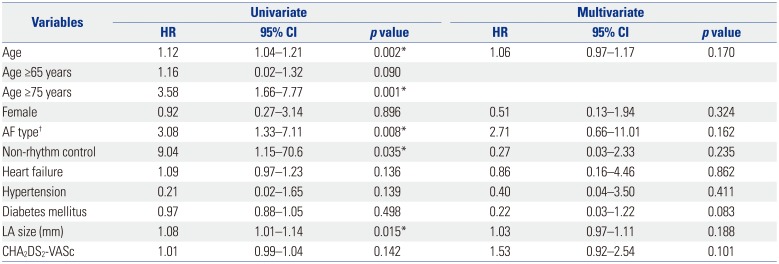
Table 3
Comparison of Clinical Outcomes for the Rhythm and the Rate Control Strategy Groups
![]()
Table 4
Cox Regression Analyses for the Prediction of Stroke Occurrence
![]()
OACs are the main contributor to the prevention of stroke.526 Warfarin reduced stroke overall by 60% to 70%, and new OACs have a beneficial effect on additional significant reductions of overall 20% relative to warfarin.6 In our study, a new OAC was mostly used (71%) and similarly prescribed between the patients in the rhythm control group and those in the rate control group among the 73% OAC-indicated study patients.
In the J-Rhythm registry with Japanese patients,27 the incidence rate of ischemic stroke was 13.4 per 1000 person-year. A previous stroke (HR 3.25), age ≥75 years (HR 2.31), and incr-eased CHA2DS2-VASc score were considered as independent risk factors for ischemic stroke in the multivariate analysis.27 Similar with other Western registries that compared the rhythm and the rate control strategy,2528 patients treated with the rhythm control strategy were younger in age and had a smaller proportion of underlying diseases and a lower CHADS2 or CHA2DS2-VASc score than those treated with the rate control strategy. In RECORDAF, significantly more patients in the rhythm control group had maintained a sinus rhythm than those in the rate control group (80% vs. 33%, p<0.001) and had a lower occurrence of stroke than those in the rate control group (1.7% vs. 2.8%, p=0.008) at the 1-year follow-up. However, in ORBIT-AF, the rhythm control group had a significantly smaller proportion of OACs than that of the rate control group (68% vs. 74%, p<0.001). However, the incidence of stroke was similar between the two groups [1.1% vs. 1.5%, adjusted HR 0.87 (95% CI 0.66−1.16), p=0.345].
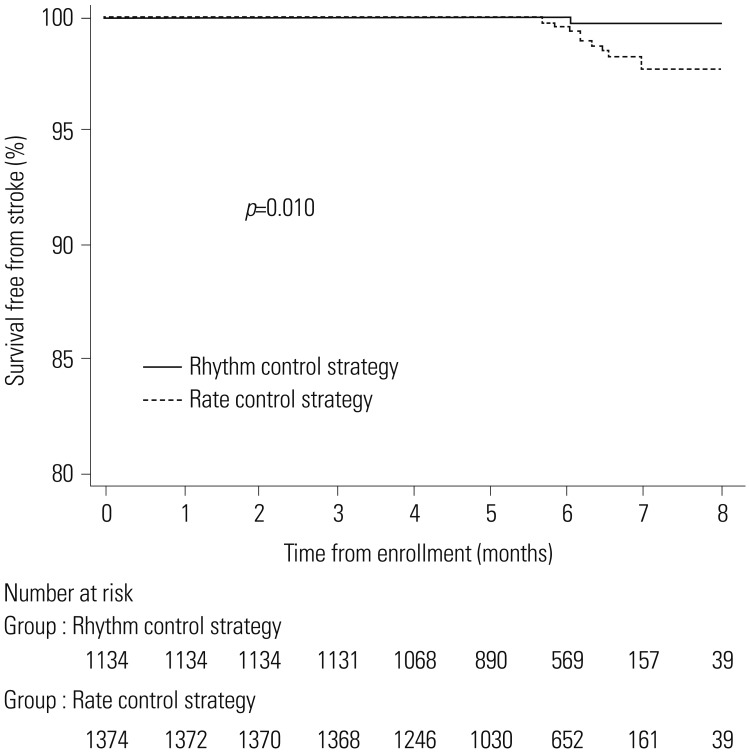
In our study, the incidence rate of stroke was 9.0 per 1000 person-years as previously reported by J-Rhythm registry. Patients treated with the rhythm control strategy were younger and had less underlying cardiovascular disease and stroke risk factors, while those treated with the rate control strategy were older and had more stroke risk factors, including diabetes, dyslipidemia, heart failure, and chronic kidney disease, and a higher CHA2DS2-VASc score. In addition, catheter ablation for anti-arrhythmic refractory AF rhythm control was more frequently undertaken in our study, compared with other previous registries. However, the rhythm control strategy might not be attributed to lower stroke, compared with the rate control strategy, in the multivariate analysis until the CABNA results are available (Catheter Ablation vs. Anti-arrhythmic Drug Therapy for Atrial Fibrillation Trial) for stroke prevention.124 In our study, the patients with rhythm control that included catheter ablation were younger, had a lower risk of stroke (mean of CHA2DS2-VASc score 2.8±1.6), and significantly more often maintained sinus rhythm at follow-up, compared with those treated with the rate control strategy. In the Kaplan-Meier curve (Fig. 1), patients treated with the rhythm control strategy seemed to be significantly associated with a higher stroke-free survival rate during over 6 months of follow up. However, in Cox regression multivariate analysis, only AF patients aged over 75 years was indicated as an independent risk factor for stroke occurrence (Table 4). We noted that 82% (9/11) of all stroke have occurred in the AF patients aged over 75 years and that the effect of rhythm control strategy could be offset by age. In addition, with the on-going CODE-AF trial, our data had only a short mean follow-up of 5.8 months, and a longer follow-up duration is needed to assess the differences between rhythm and rate control strategies in stroke prevention.
Our study has several limitations. First, our study has short follow-up duration and unknown confounding factors. Second, the data used for the analysis cannot quantify AF burden, which may have differed between the rhythm and the rate control strategy groups. Third, there are concerns for a sufficient power of association for stroke occurrence in this study.
In conclusions, in this prospective AF cohort with guideline adherence, the rhythm control strategy showed no benefit on cardiovascular mortality, but seemed to lower the risk of stroke compared, to the rate control strategy. However, only age, especially older than 75 years, was deemed an independent risk factor for the occurrence of stroke, regardless of which control strategy was applied.
 XML Download
XML Download