

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary flow reserve (CFR) is defined as the magnitude of increased coronary flow from the basal state to that achieved following maximal coronary vasodilation, and is recognized as an indicator of myocardial perfusion.1 Poor clinical outcomes have been found to be closely related with dysfunction of microcirculation perfusion, both in patients with satisfactory and those with unsatisfactory revascularization of the infarct-related artery.234 A large number of experiments have shown that myocardial infarction (MI) area and left ventricular function are largely affected by microcirculation function, which is closely related to recovery of left ventricular function and long-term left ventricular remodeling.567 About 25% of patients who have successfully undergone angioplasty still suffer from microvascular dysfunction.8910 It has been shown that microvascular dysfunction is not only in the infarcted myocardium but also in the non-infarcted myocardium. However, the clinical importance thereof has not been fully elucidated.1112
The purpose of this study was to evaluate the relationship between CFR in the non-infarcted myocardium and long-term clinical outcome in patients with acute myocardial infarction (AMI) and to analyze factors influencing the value of CFR in the non-infarcted myocardium.
Go to : 
MATERIALS AND METHODS
Study population
A total of 100 patients (74 males and 26 females) with first AMI and single-vessel disease who were undergoing primary percutaneous coronary intervention (PCI) within 12 hours after symptom onset were enrolled in the study and followed up for 12 months. The study protocol was approved by the Institutional Review Board of the Fourth Hospital of Harbin Medical University. Patients under unstable condition, severe extracardiac disease, or severe valve disease were excluded. Informed consent was obtained from all patients.
Serum parameter
As the levels of creatinine kinase or cardiac troponin I (cTnI) in serum are important parameters to diagnose AMI, cTnI levels were chosen for assay in this study, and were measured on admission and every six hours during the first 24 hours.
Percutaneous coronary intervention
PCI was performed with standard techniques and the stent was placed in all patients. All patients received aspirin (300 mg loading dose) and ticagrelor (180 mg loading dose) prior to PCI. A regimen of 180 mg ticagrelor per day was continued for at least 12 months after PCI, and 100 mg aspirin daily was prescribed indefinitely. Successful primary angioplasty was defined as a final thrombolysis in MI flow grade 3 in the infarctrelated artery and residual stenosis of <20%.
Two-dimensional echocardiography
Two-dimensional echocardiography (Philips iE33, Philips Healthcare, Andover, MA, USA) was performed one week after PCI to measure left ventricular end diastolic volume, left ventricular end systolic volume, and calculated left ventricular ejection fraction (LVEF).
Myocardial contrast echocardiography
Myocardial contrast echocardiography (MCE) was performed one week after PCI, using intravenous injection of sonovue at baseline and during hyperemia. Meanwhile, dobutamine was injected by intravenous infusion during hyperemia (at a starting dose of 5 µg/kg/min, followed by an increasing dose of 10 µg/kg/min up to a dose of 20 µg/kg/min in 3-minute stages). MCE images were acquired both at baseline and hyperemia. Sonovue (Bracco, Milan, Italy) was used as the intravenous contrast agent and administered by an infusion syringe-pump.13
CFR measurement
The left ventricular was divided into 17 segments. The non-infarcted myocardium far away from the infarcted myocardium was selected to ensure that there was no interaction between these two. Regions of interest (ROIs) were placed and tracked manually within the myocardium at baseline and after hyperemia. The software package automatically calculated the mean acoustic intensity of each ROI and generated time-intensity curves that were subsequently fitted to a monoexponentially function: y=A(1-e-βt)(q). Myocardial blood flow (MBF) was calculated as the product of A×β. Basal and hyperemic MBF was derived, and CFR (MBF at hyperemia/MBF at baseline) was calculated for each patient.141516 All images were independently analyzed by two experienced observers, who were blinded to the clinical data, angiographic results, and other respective imaging.
Clinical outcomes and definitions
The primary endpoint of this study was the 12-month commutative incidence of major adverse cardiac event (MACE). MACE comprised all causes of death, non-fatal MI, advanced heart failure, repeat target vessel revascularization, and ischemic stroke. All patients were divided into MACE and non-MACE groups according to the incidence of 12-month MACE.
Statistical analysis
Statistical analysis was performed using SPSS 20.0 software (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as means±standard deviations, and were analyzed by Student's t-tests. Categorical variables are expressed as percentages and counts, and were analyzed by the chi square test. p-values less than 0.05 were considered statistically significant. Variables with a p value <0.05 in univariate analysis were included in the multivariate cox regression model, and results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). Multivariate cox regression analysis was performed to assess the independent predictors of MACE. A receiver-operating characteristic (ROC) curve was drawn to evaluate the diagnostic value of CFR in the non-infarcted myocardium and peak cTnI in MACE and to determine the optimum cutoff level for CFR. Survival analysis was conducted using Kaplan-Meier survival curves, and the differences were compared using the log-rank test.
Go to :
RESULTS
Patients
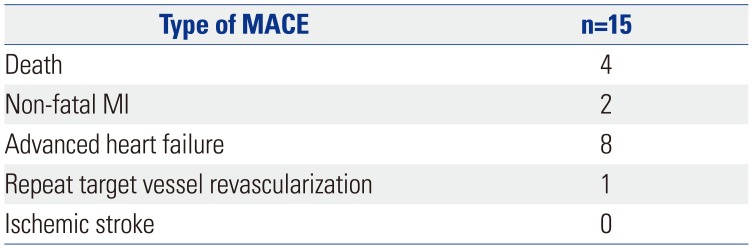
Among all patients in our study, MACEs occurred in 15 patients (15%) (all causes of death, n=4; non-fatal MI, n=2; advanced heart failure, n=8; repeat target vessel revascularization, n=1; and ischemic stroke, n=0)(Table 1).
Clinical variables in the MACE and non-MACE groups
Mean peak cTnI in the MACE group was significantly higher than that in the non-MACE group (23.67 vs. 12.71 µg/mL, p<0.001). Mean CFR in the non-infarcted myocardium in the MACE group was significantly lower than that in the non-MACE group (2.412 vs. 2.771, p<0.001)(Table 2). There were no differences in the other variables between these two groups.
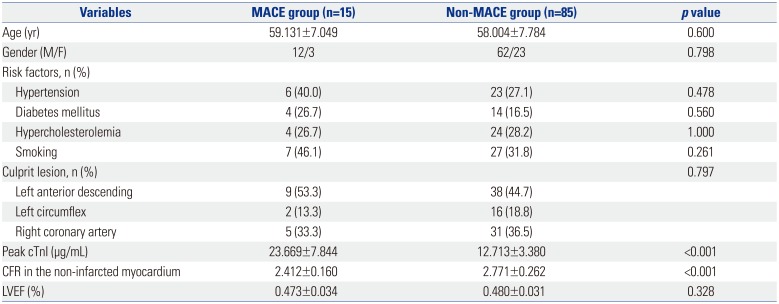
Table 2
Comparison of the Two Study Groups according to Clinical Variables (n=100)
![]()
ROC curve and cut-off values
When predicting MACE by ROC curves, the sensitivity and specificity of CFR <2.305 were 91% and 86%, respectively [area under the curve (AUC)=0.958], and the sensitivity and specificity of peak cTnI >18.50 were 80% and 94%, respectively (AUC=0.935)(Fig. 1).
 | Fig. 1The best cut-off values of CFR in the non-infarcted myocardium and peak cTnI were analyzed using ROC curves. CFR in the non-infarcted region (AUC=0.958), cut-off=2.305, sensitivity=0.91, specificity=0.86). Peak cTnI (AUC=0.935), cut-off=18.50, senstivity=0.80, specificity=0.94. CFR, coronary flow reserve; cTnI, cardiac troponin I; ROC, receiver-operating characteristic; AUC, area under the curve.
|
Predictive value of CFR in the non-infarcted myocardium on 12-month MACE
In univariate analysis, CFR in the non-infarcted myocardium and peak cTnI showed a significant association with 12-month MACE (p<0.001). These two factors with a p<0.05 were included in a multivariate cox regression analysis, and the interaction between the two factors was corrected. Therein, the risk of MACE in patients with high CFR (CFR≥2.305) was lower than that in patients with low CFR (CFR<2.305) (HR=0.093, 95% CI: 0.020–0.426, p=0.002)(Table 3).
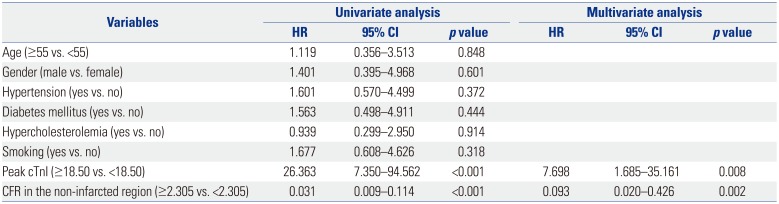
Table 3
Factors Associated with Major Adverse Cardiac Event in Univariate and Multivariate Cox Regression Analysis
![]()
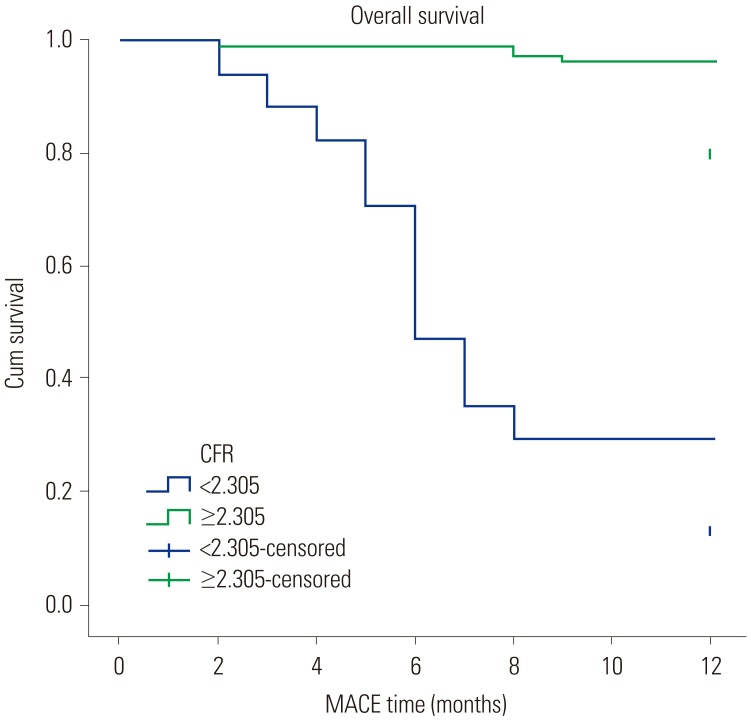
Kaplan-Meier curves of cumulative survival rate (one-year survival)
Kaplan-Meier curves revealed median survival times of 7.353 ±0.802 months in the CFR <2.305 group and 11.795±0.133 months in the CFR ≥2.305 group (p<0.001)(Fig. 2).
The impact factors of CFR
According to the CFR cut-off value of 2.305 in the non-infarcted myocardium, all patients were divided into two subgroups: Group I (CFR<2.305) and Group II (CFR≥2.305). Peak cTnI was higher in Group I than in Group II (p<0.001), while LVEF was lower in Group I than in Group II (p=0.001)(Table 4).
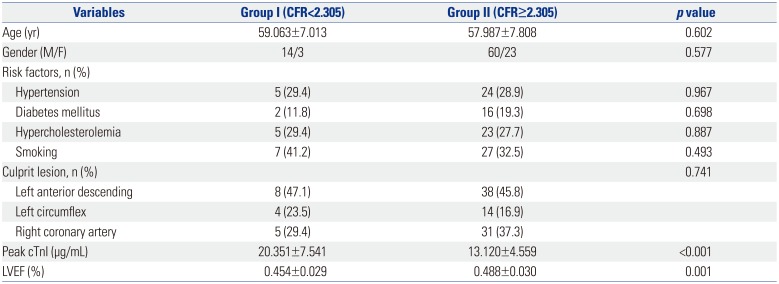
Table 4
Comparison of Clinical Variables (n=100)
![]()
Go to :
DISCUSSION
To the best of our knowledge, this is the first study to investigate the association between CFR in the non-infarcted myocardium and 12-month adverse clinical outcomes in patients with AMI undergoing PCI. The non-MACE group was more likely to have lower peak cTnI and higher CFR in the non-infarcted myocardium than the MACE group. Multivariate analysis identified CFR in the non-infarcted myocardium as an independent predictor of 12-month MACE after adjusting for multiple cardiovascular risk factors. Additionally, we found the mean survival time of the low CFR group (CFR<2.305) to be significantly shorter than that of the high CFR group (CFR≥2.305). Moreover, we further analyzed factors related with CFR value, among which only peak cTnI and LVEF were statistically significant. Thus, we inferred that CFR value is closely associated with the MI size and left ventricular function.
MCE is the gold standard method to assess myocardial microcirculation.17 The predictive value of CFR measured by MCE for no reflow phenomenon and left ventricular remodeling after PCI has been revealed by several clinical studies.618 Decrease in CFR in the non-infarcted myocardium was correlated with an increase in the extent of ischemia. Alterations in CFR in the non-infarcted myocardium had important clinical implications after revascularization.19 Furthermore, some relevant biomarkers and other easily available clinical parameters have also been studied to predict the incidence of MACE, such as mean platelet volume and neutrophil counts.20
Microvascular dysfunction is found not only in the infarcted region but also in the remote region, which has been discovered long before. In MI animal models, CFR and coronary resistance changes were found in the non-infarcted areas, which were independent of changes in hemodynamic parameters.21 Similar studies in humans also verified that coronary vasodilator responses decreased in patients with non-infarcted myocardium after PCI.2223 However, the etiology and clinical importance of microvascular dysfunction in the non-infarcted myocardium are not fully understood.
Several mechanisms for CFR in the non-infarcted myocardium seem to have a correlation with MACE. The decrease of CFR in the non-infarcted myocardium is representative of more extensive necrosis and deterioration of cardiac function, which was also proved in our study.24 Microvascular dysfunction in the non-infarct area is an indicator of enlargement of the ischemic range, which can reduce myocardial collateral circulation to the infarction area and increase the area of MI. Also, the cardiospecific overexpression of angiotensin II type I receptor and decrease in microvessel density in the non-infarcted myocardium may lead to some cardiovascular events, mainly cardiac remodeling and heart failure.25 Moreover, investigators have also suggested that alterations in CFR in the non-infarcted myocardium also could be attributed to increased sympathetic nervous system activity, leading to coronary vasoconstriction and decreased vasodilator reserve.26 Furthermore, some scholars indicate that microvascular dysfunction after MI is associated with impaired sympathetic innervation and function even in the non-infarcted myocardial tissues. Impaired sympathetic innervation might be associated with electrical instability. Adverse structural and electrophysiological remodeling at non-infarcted regions after MI are responsible for clinically ventricular arrhythmias, leading to sudden cardiac death eventually. Ventricular tachyarrhythmias are life threatening cardiac arrhythmias and the most common causes of sudden cardiac death.27
In our study, the incidence of MACE after PCI was 15%, slightly higher than that in other studies, which may be related to the small sample size of patients selected. Moreover, CFR was measured only once after PCI, and we could not evaluate changes in microvascular perfusion. Also, some problems in the examination of MCE are still difficult to figure out at present, such as a number of segments appearing as acoustic shadow and artifacts.28 In addition, the relevant mechanism between CFR in the non-infarcted myocardium and MACE is planned to be explored in future study. We should also draw more attention to apparently “normal” non-infarction regions for further understanding of the mechanism of sudden cardiac death.
In conclusion, our results clearly show that CFR in the noninfarcted myocardium is associated with prognostic significance for 12-month MACE in patients with AMI undergoing primary PCI. The use of CFR is advised in contemporary clinical practice.
Go to :
 XML Download
XML Download