

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial flutter (AFL) is associated with an increased risk of thromboembolism.12 Radiofrequency catheter ablation of AFL has a high success rate with rare complications. Thus, catheter ablation is generally accepted as a first-line treatment strategy for patients with typical AFL.3 Nonetheless, subsequent development of atrial fibrillation (AF) is common after AFL ablation. A prior meta-analysis reported that the overall incidence of AF after AFL ablation was 33.6%, with an average follow-up of 15 months; however, 3 years after ablation, the incidence of AF was up to 56.6%.4 If no atrial arrhythmias are apparent, the prevalent practice is to stop anticoagulation one month after successful AFL ablation.567 As a result, a subset of patients who undergo catheter ablation of AFL may be at risk for thromboembolic complications, including ischemic stroke. Risk assessment using readily available clinical variables is the key to identify patients at increased risk of postablation stroke. Previous studies suggested that old age and postablation AF were risk factors of stroke;78910 however, a predictor of stroke among patients with AFL who have undergone cavotricuspid isthmus (CTI) ablation have not been elucidated. No clear strategy addressing antithrombotic therapy after successful AFL ablation has emerged.
CHA2DS2-VASc score is a recommended risk stratification scheme for prediction of stroke or thromboembolism in nonvalvular AF patients. Recently, this scoring system has been validated to have predictive capacity for outcomes in patients in different clinical situations. The aims of this study were to investigate predictors of stroke and whether CHA2DS2-VASc score is useful risk assessment tool for ischemic stroke in patients following successful AFL ablation.
MATERIALS AND METHODS
Study population
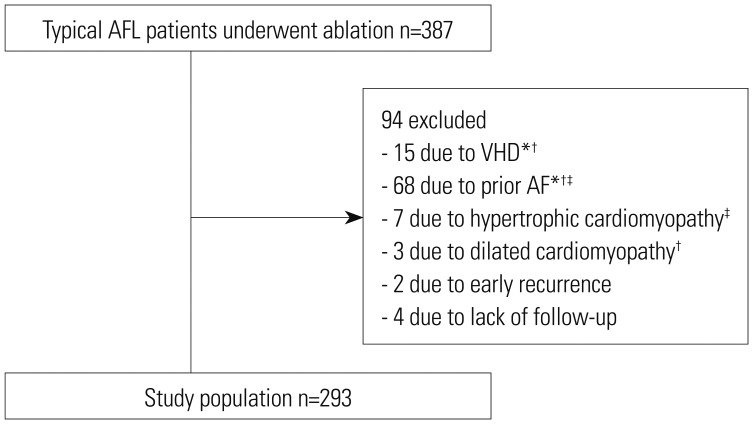
The subjects were consecutive patients who underwent successful catheter ablation for typical AFL at Severance Cardiovascular Hospital from October 2003 to January 2013. Typical AFL was diagnosed when a surface electrocardiogram (ECG) showed readily visible negative flutter wave in the inferior leads and positive flutter wave in lead V1 with a regular atrial rate.11 Of the 387 patients enrolled, exclusion criteria were prior history of AF (n=68), moderate-to-severe valvular heart disease (n=15), hypertrophic cardiomyopathy (n=7), dilated cardiomyopathy (n=3), early recurrence less than 3 months (n=2), and follow-up period less than 6 months (n=4) (Fig. 1). Patient data including age, sex, comorbidities, use of medications, electrocardiographic findings, echocardiographic features, result of the ablation procedure, and follow-up information were collected. The CHA2DS2-VASc scores [congestive heart failure, hypertension, age ≥75 years (doubled), diabetes mellitus, prior stroke or transient ischemic attack (TIA) (doubled), vascular disease, age 65 to 74 years, sex category] were calculated for each patient at the time of the ablation procedure. All signed written informed consent for the ablation procedures. Patients were enrolled prospectively in a longitudinal registry, and analysis was performed retrospectively. The study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System, Seoul, Korea (#4-2017-0937) and complied with the Declaration of Helsinki.
Electrophysiology study and catheter ablation
Antiarrhythmic drugs were discontinued for at least 5 half-lives before ablation. Electrophysiological studies were performed in the postabsorptive state. Multipolar catheters were positioned as follows: 1) A duodecapolar catheter with 2-5-2 mm interelectrode was positioned in the right atrium (RA), parallel to the tricuspid annulus so that the distal pole was located in the medial region of the CTI. 2) A decapolar catheter was inserted within the coronary sinus, with the proximal bipole located at the ostium. 3) Quadripolar catheters were positioned at the His bundle and RA. Surface ECG and bipolar endocardial electrograms were monitored continuously and stored on a computer-based digital amplifier/recorder system with optical disk storage for offline analysis. Intracardiac electrograms were filtered from 30 Hz to 500 Hz and measured with computer-assisted calipers at a sweep. Ablation was typically started on the ventricular aspect of the CTI region, and sequential radiofrequency lesions were created extending from the tricuspid valve to the posterior aspect of the CTI. Ablation was deemed successful if AFL terminated during radiofrequency delivery, AFL was no longer inducible, and bidirectional CTI block was demonstrated.
Periprocedural anticoagulation strategy
Almost all patients were treated with warfarin to maintain an international normalized ratio between 2 and 3 for at least 3 weeks before the procedure, and continued to receive warfarin for at least 1 month after the procedure. After 1 month, decisions on continuing anticoagulation was determined at the physician's discretion, based on individual patient stroke risk factors. Antithrombotic drugs were administered according to characteristics of each patient.
Follow-up and clinical end point
The patients were monitored by continuous ECG recordings in a hospital for at least 24 hours. After discharge, all patients were followed up with clinical examination, 12-lead ECG, and 24-hour ambulatory Holter monitoring at 1, 3, 6, and 12 months after the procedure, and every 6 months thereafter. Subsequently, patients were seen every 3 to 6 months at our cardiology clinic. A successful outcome was defined as the absence of any atrial arrhythmia after the 3-month blanking period. New-onset AF was defined as symptomatic or asymptomatic AF documented by 12-lead ECG or ambulatory rhythm monitoring that lasted at least 30 seconds.12 The clinical endpoint was an ischemic stroke, which was defined as onset of a new neurologic impairment that occurred after the ablation. Diagnosis of a stroke was confirmed by a neurologist, and correlated with cranial imaging evidence (computed tomography and/or magnetic resonance imaging). Stroke severity at baseline was assessed with the National Institutes of Health Stroke Scale (NIHSS) score by a neurologist.13 Etiology of ischemic stroke was classified into five categories by the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification: 1) large-artery atherosclerosis, 2) cardioembolism, 3) small vessel occlusion, 4) stroke of other determined etiology, and 5) stroke of undetermined etiology.14 Patients were censored at death, loss of follow-up, or end of study, whichever occurred first.
Statistical analysis
Continuous data are expressed as mean±standard deviation, and categorical variables are expressed as counts and percentages (%). Normality tests were performed for each variable to determine whether a dataset was well-modeled by normal distribution. Univariate comparisons were performed using Student's t-test or Mann-Whitney U test for continuous variables, and chi-square test or Fisher's test for categorical variables. Cox proportional hazards model was performed to identify predictors associated with ischemic strokes. Due to the small number of stroke events, multivariate Cox regression was performed using variables that had significant association with the risk for stroke by univariate analysis. The predictive accuracy of CHA2DS2-VASc score and the optimal cutoff value in the prediction of stroke after AFL ablation were identified using receiver operating characteristic (ROC) curves and Youden index (sensitivity+specificity-1). Event free survival curves were plotted by the Kaplan-Meier method with the statistical significance tested by the log-rank test. Statistical significance was established at a value of p<0.05. Statistical analyses were performed with SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Clinical characteristics and predictors of stroke after AFL ablation
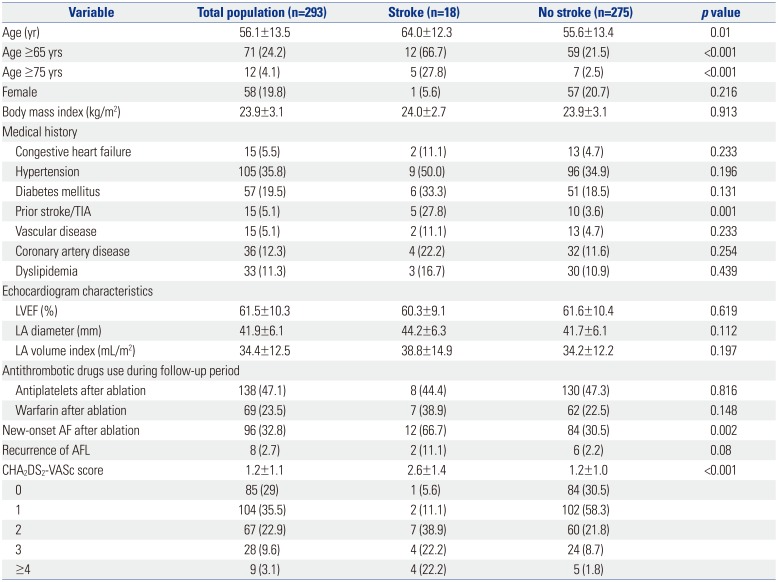
A total of 387 patients were enrolled; 94 patients were excluded from the present study. The study population comprised 293 patients who underwent successful catheter ablation for typical AFL (Fig. 1). During the follow-up period of 60.8±45.9 months, ischemic strokes occurred in 18 (6%) patients. Median time to stroke occurrence was 34 months (interquartile range, 13–65 months) after ablation, and median NIHSS score on admission for stroke was 2.5 (interquartile range, 1–6). Among 18 patients who developed stroke, the causes of stroke were as follows: cardioembolic stroke (n=15), large artery atherosclerosis (n=1), small-vessel occlusion (n=1), and undetermined etiology (n=1). No patients had hemorrhagic stroke during follow-up periods. The 1-year and 5-year successful outcomes defined as absence of atrial arrhythmias were 94.9% and 72.7%, respectively. New-onset AF was detected in 96 patients (32.8%) during the follow-up period, including 87 (90.6%) paroxysmal and 9 (9.4%) persistent AFs.
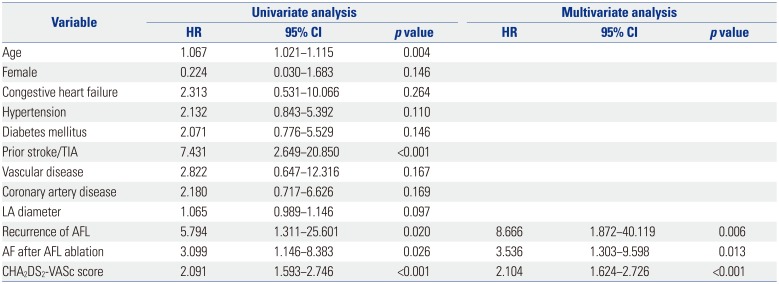
Baseline characteristics in relation to development of ischemic stroke after AFL ablation are presented in Table 1. Higher CHA2DS2-VASc scores, advanced age, prior history of stroke or TIA, recurrence of AFL, and occurrence of AF after ablation were significant univariate predictors for postablation stroke. In multivariate analysis, CHA2DS2-VASc score, relapse of AFL, and development of AF after ablation remained independent predictors for ischemic stroke after AFL ablation (Table 2).
CHA2DS2-VASc score for prediction of stroke after AFL ablation
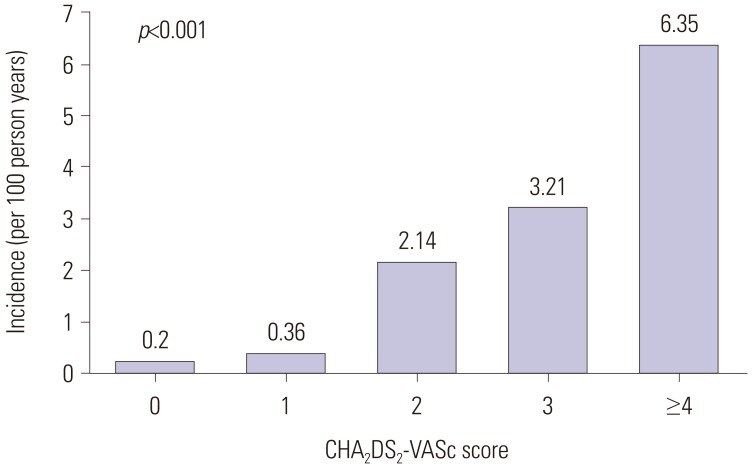
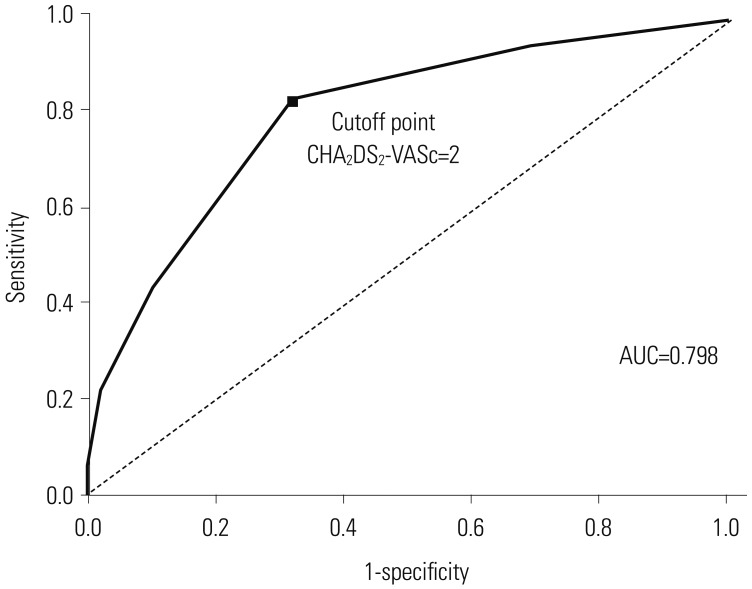
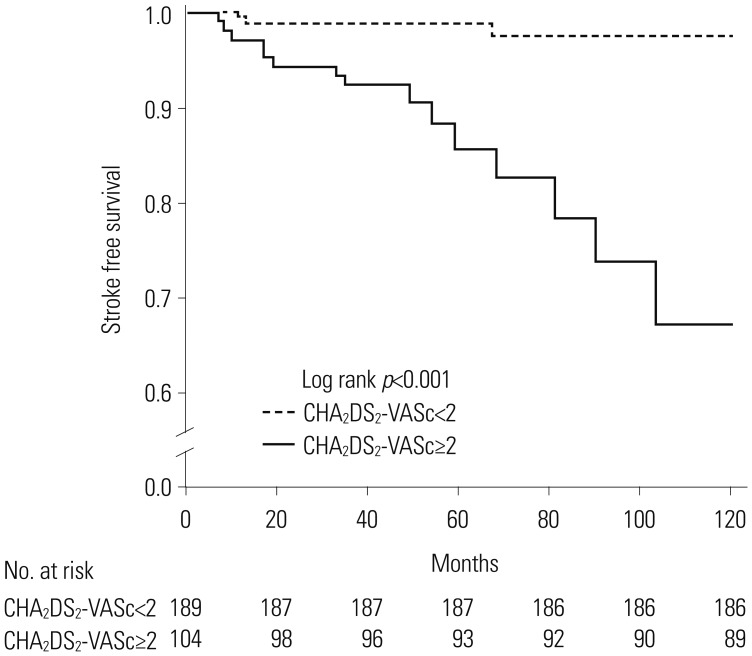
CHA2DS2-VASc score was the strongest predictor of s stroke event after AFL ablation for a 1-point increase. The incidence of stroke increased with increases in patients' CHA2DS2-VASc scores (Fig. 2). ROC curves for the performance of CHA2DS2-VASc score in predicting incident stroke after AFL ablation were drawn. The area under the curve for the CHA2DS2-VASc score was 0.798 (95% CI, 0.691–0.904). A cutoff point of 2 was identified using the ROC curve (sensitivity 83.3%, specificity 67.6%) (Fig. 3). The Kaplan-Meier survival analysis revealed that the cumulative incidence of stroke after AFL ablation was higher in patient with a CHA2DS2-VASc score ≥2 than in those with CHA2DS2-VASc score <2 (14.4% vs. 1.6%, p<0.001) during the follow-up period (Fig. 4).
DISCUSSION
Main findings
This analysis investigated the incidence and predictors of ischemic stroke events in patients undergoing successful catheter ablation of typical AFL. By utilizing CHA2DS2-VASc score, the risk of stroke after AFL ablation was revealed to be correlated with the score, with an increasing trend in stroke with ascending CHA2DS2-VASc score. The main findings of this study were as follows: 1) the incidence of ischemic stroke after AFL ablation was 1.15 strokes per 100 person-years; 2) CHA2DS2-VASc score, AFL recurrence, and postablation AF were independent predictors; 3) CHA2DS2-VASc score was useful for stratifying the risk of stroke after catheter ablation of AFL; and 4) a CHA2DS2-VASc score of ≥2 was associated with higher risk of stroke following ablation.
Relationship among CHA2DS2-VASc score and stroke after catheter ablation of AFL
In the HRS/EHRA/ECAS Consensus Statement on the continuation of anticoagulation after AF ablation, CHA2DS2-VASc scores or CHADS2 are recommended for estimating stroke risk.12 No separate statements for the management of patients with AFL exist. The CHA2DS2-VASc score uses the primary risk factors in the CHADS2 scoring system, although it includes additional risk factors (65 to 74 years of age, female sex, and vascular disease) and has a broader score range. Recent studies reported that CHA2DS2-VASc score improved predictive ability for stroke and thromboembolism, compared to CHADS2 score.151617 There has been a marked shift in antithrombotic strategy for low-risk patients to improve outcomes by using CHA2DS2-VASc score. Both updated US and European clinical practice guidelines on AF recommend use of CHA2DS2-VASc score for assessment of stroke risk.1118 The role of CHA2DS2-VASc score has been extended beyond its initial purpose of estimating the risk of thromboembolism in patients with nonvalvular AF. CHA2DS2-VASc score has been indicated to predict clinical outcomes in various conditions, including thromboembolism risk after AF ablation,19 stroke risk in patients without AF,20 and left atrial thrombus risk among AFL patients.21 Besides, the components of the CHA2DS2-VASc score are associated with ischemic stroke regardless of heart rhythm. The Atherosclerosis Risk in Communities study reported that old age, hypertension, and diabetes were independent risk factor for all ischemic stroke subtypes involving cardioembolism,22 and heart failure was associated with increased risk of stroke and thromboembolism whether or not AF was present.2324 In addition, patients with high CHA2DS2-VASc scores have been shown to have higher risk of developing AF,25 which is common after successful AFL ablation426 and may contribute to subsequent ischemic stroke.727 It is logical that this scoring system may have clinical utility for risk assessment of stroke following AFL ablation. Nevertheless, in spite of these previous findings, there is little data about the relation between the CHA2DS2-VASc score and stroke after catheter ablation of AFL. As expected, higher CHA2DS2-VASc scores identified patients who are likely to develop stroke. The C statistics indicated CHA2DS2-VASc score had good discriminatory performance. To the best of our knowledge, this is the first study to evaluate the predictive ability of CHA2DS2-VASc score in assessing the risk for ischemic stroke in AFL patients who have received catheter ablation. Our results provide evidence for extending clinical value of CHA2DS2-VASc score to a risk stratification model for predicting stroke after typical AFL ablation.
Clinical implications
In the present cohort, over an average follow-up of 5 years after AFL ablation, ischemic strokes occurred in 6% of patients, amounting to an incidence of 1.15 strokes per 100 person-years. The stroke rate in our study was lower than what would have been expected from the natural history of chronic AFL (1.55 strokes per 100 person-years),28 but higher than that of the general population (0.53 strokes per 100 person-years).29 This result was consistent with those found in the earlier studies.7 Although patients had successful catheter ablation of typical AFL, patients were at continued risk of ischemic stroke. This raises concerns for the process of selecting patients for continuation of antithrombotic therapy after flutter ablation. Thus, appropriate selection of patients at high risk of stroke is an important for optimal risk-based therapeutic decisions. However, previous studies did not suggest useful methods to identify patients at risk of stroke after AFL ablation. CHA2DS2-VASc score is composed of commonly collected clinical variables and can be applied easily in clinical practice. The present study demonstrated the ability of CHA2DS2-VASc score to reliably discriminate between “high-risk” and “low-risk” patients for stroke following ablation of AFL. A CHA2DS2-VASc score ≥2 identified patients with absolute risk of ischemic stroke of >1% per year. In the general AF population, an annual risk of stroke of >1% often used to identify patients in whom the benefits of long-term oral anticoagulation may outweigh the risks of bleeding.30 Patients with a score ≥2 who have high absolute risk of stroke may benefit from continuation of anticoagulation, although randomized trial studies in direct support of this approach are still deficient. These findings may help physicians to identify patients at high risk of stroke and to perform closer follow-up after ablation. It would be reasonable to suggest that physicians make a decision about continuation of anticoagulation after AFL ablation based on the CHA2DS2-VASc score.
Study limitations
This study had several limitations. First, it was based on a single center experience, which could have caused site specific bias. Second, the study was performed in a cohort of predominantly male patients, which may limit generalizability. In the population-based investigation, AFL was 2.5 times more common in men than in women.31 However, the number of women was a fourth of those of men in this study. Third, patient follow-up was not uniform, but almost all patients underwent follow-up regularly. Fourth, the antithrombotic strategy was determined by the physicians responsible for treatment according to the individual characteristics of each patient. However, the management was based on the same principle for individuals with similar risk.
Conclusions
Patients undergoing successful catheter ablation of typical AFL remain at continued risk for ischemic stroke. CHA2DS2-VASc score is a useful predictor for ischemic stroke and in stratifying patients at risk of stroke after AFL ablation. This scoring system may be reliable in identifying high risk patients who may benefit from antithrombotic therapy.
 XML Download
XML Download