

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lung cancer is the leading cause of cancer-related death worldwide.1 Non-small cell lung cancer (NSCLC) is the most common type of lung cancer, accounting for approximately 85% of all cases.1 Since the discovery of oncogenic alterations in NSCLC, targeted therapeutic agents have been developed, resulting in improved survival in patients with treatable oncogenic alterations, including epidermal growth factor receptor (EGFR) mutation and anaplastic lymphoma kinase translocation.2 Development of sensitive and specific methods to detect treatable oncogenic alterations is therefore a meaningful endeavor,2 and a variety of methods for detecting oncogenic alterations in NSCLC have been developed.3
Direct sequencing (DS) is the traditional and standard method for detecting EGFR mutations, and remains the most useful validated method for testing.3 However, DS requires a complex procedure, including DNA extraction, PCR-based amplification, DNA sequencing, and sequence interpretation.3 In addition, the sensitivity of DS is low, as it can only detect mutant DNA that makes up at least 25% of the total DNA content.4 Thus, several other assays have been created to increase sensitivity. The peptide nucleic acid (PNA) clamping method was recently approved by the Korean Food and Drug Administration.5 PNAs are artificially synthesized polymers that can strongly bind to complementary DNA sequences.6 PNA probes suppress PCR amplification of wild-type sequences, allowing for greater amplification of mutant sequences.6 Indeed, PNA clamping can be used to detect mutant alleles, even when present at levels 100-fold lower than wild-type alleles, and is less technically complex than DS.7 However, the PNA clamping method has a weakness in that it can only detect mutations for which primers have been individually designed.6 Thus, PNA clamping is not useful for detecting novel mutations.6
Whether intratumoral heterogeneity in EGFR mutations is one of the mechanisms for resistance to EGFR-tyrosine kinase inhibitors (TKIs) remains controversial.891011 Since responses to EGFR-TKIs could be correlated with EGFR mutant content, molecular tests with high sensitivity for detecting EGFR mutations might help with discerning which patients would be unlikely to respond to EGFR-TKIs.
DS has low sensitivity and has not been directly compared with PNA clamping methods in a systematic manner with respect to predicting oncogenic alterations. Furthermore, it is not clear if the PNA clamping method is non-inferior to DS with respect to predicting patient responses to EGFR-TKIs based on mutation detection. Thus, the primary aim of this study was to investigate whether PNA clamping has a higher rate of detection of oncogenic alterations, compared to DS, in patients with NSCLC. We also assessed clinical responses to EGFR-TKIs according to EGFR mutation status identified using both of these detection methods.
MATERIALS AND METHODS
Data sources and search strategy
This meta-analysis was performed in accordance with the recommendations on the conduct and reporting of systematic reviews and meta-analyses outlined by the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement.12 To identify relevant articles eligible for this meta-analysis, we conducted a comprehensive search of three electronic databases (MEDLINE, EMBASE, and the Cochrane Central Register) up to September 01, 2017 using the following search terms: PNA clamping, DS, next-generation sequencing, pyrosequencing, lung cancer, lung adenocarcinoma, and NSCLC. As this study was a systematic review of published articles, neither informed consent nor ethics approval was required. The references listed in relevant review articles were also searched manually.
Inclusion and exclusion criteria
In order to be included in our analysis, studies had to meet the following inclusion criteria: 1) directly compared PNA clamping and DS; 2) included patients with a diagnosis of NSCLC; and 3) provided sufficient data to calculate absolute numbers of true-positive, false-positive, false-negative, and true-negative results. Studies published as full-length articles or letters in peer-reviewed English language journals were eligible for inclusion. Review articles, case reports, commentaries, and studies reporting outcomes but without raw data were excluded.
Data extraction and quality assessment
J-U.S. and J.L. independently conducted an extraction of potentially relevant articles, and reviewed each study in accordance with predefined eligibility criteria, after which data were extracted. Any disagreements that arose during the process of study selection or data extraction were resolved by consensus. A predefined form was used to extract data from each study. The information extracted from selected studies consisted of patient demographics, study design, and objectives.
As recommended by the Cochrane Collaboration, we used the Quality Assessment of Diagnostic Accuracy Studies (QUADAS)-2 tool to evaluate the risk of bias in diagnostic test accuracy.13 The QUADAS-2 tool consists of the four following key domains: patient selection, index test, reference standard, and flow/timing of patient selection. Supplementary Fig. 1 (only online) summarizes the seven items selected to evaluate risk of bias and applicability. The possible answers to each item were “yes,” “no,” or “unclear,” corresponding to a low, high, and unclear risk of bias, respectively. If a study was judged as “low” on all domains relating to bias or applicability, then it was assigned an overall judgment of “low risk of bias” or “low concern regarding applicability.” If a study was judged “high” or “unclear” in one or more domains, then it was judged as either “at risk of bias” or having “concerns regarding applicability.” Discrepancies were resolved by discussion between the two authors (J-U.S. and J.L.).
Data synthesis and statistical analysis
The data are presented as mean values for continuous variables and as frequencies (%) for categorical variables. For diagnostic meta-analysis, we extracted the numbers of patients with true-positive, false-positive, false-negative, and true negative test results either directly or through a recalculation based on the reported measures of accuracy in combination with the prevalence and sample size of the included study. We calculated pooled sensitivity and specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), and area under the receiver-operating characteristic curve (AUC) as point estimates with 95% confidence intervals (CIs).14 We additionally constructed summary receiver-operating characteristic curves (SROCs). In order to compare clinical responses to EGFR-TKIs according to detection method, we calculated pooled risk ratios (RR) and 95% CI. Between-study statistical heterogeneity was assessed using I2 and the Cochrane Q test.15 Heterogeneity was assessed using I2 statistics on a scale of 0−100%. A fixed-effects model was used unless I2 was >50%, indicating a substantial level of between-study heterogeneity, in which case a random-effects model was used.15
If substantial heterogeneity was found, analysis via meta-regression was performed to explore potential sources of bias.16 Publication bias was evaluated by Deeks' funnel plot asymmetry test.17 A p-value<0.05 was considered statistically significant. Statistical analyses were performed with Meta-Disc software (version 1.4, Madrid, Spain), Stata statistical software (version 14.2, StataCorp LP, College Station, TX, USA), and Review Manager (version 5.3, Nordic Cochrane Centre, the Cochrane Collaboration, Copenhagen, Denmark).
RESULTS
Study search and characteristics and quality of included studies
The literature search process is shown in Fig. 1. A total of 4006 published articles were initially identified (1450 articles from MEDLINE, 2472 articles from EMBASE, and 84 articles from the Cochrane library). After removing duplicate articles, we screened 3206 potentially eligible articles. After reviewing titles and abstracts, 3164 search records were removed, and the remaining 42 articles were further evaluated by reading the full text. Thirty-two articles were excluded for the reasons shown in Fig. 1. Finally, 10 studies were included in our final analysis.571819202122232425
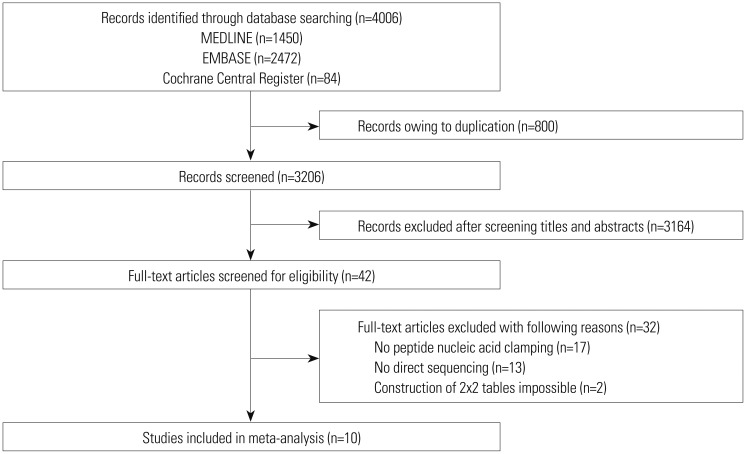
Table 1 summarizes the features of the included studies. Ten studies involving 924 subjects met the defined inclusion criteria, and the numbers of patients in each trial ranged from 20 to 240. All studies were published between 2011 and 2016. Eight studies included results from NSCLC patients,57192021222325 and two studies included results solely from lung adenocarcinoma patients.1824 The rates of lung adenocarcinoma in the studies ranged from 58% to 100%.571819202122232425 Eight studies were evaluated for EGFR mutations, and the detection rates of EGFR mutation ranged from 35% to 62%.57182021222425 Two studies reported on KRAS mutations, and the detection rate of KRAS mutation in those two studies was 16%.1923
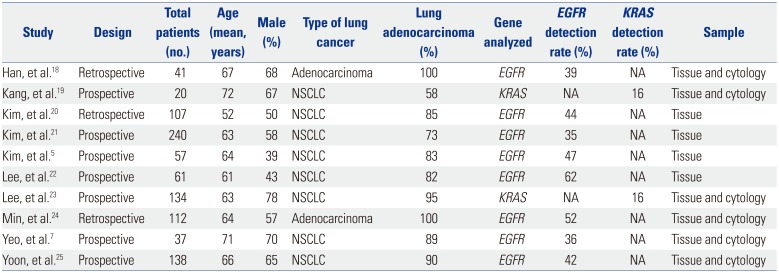
Table 1
Characteristics of the Studies Included in the Meta-Analysis
| Study | Design | Total patients (no.) | Age (mean, years) | Male (%) | Type of lung cancer | Lung adenocarcinoma (%) | Gene analyzed | EGFR detection rate (%) | KRAS detection rate (%) | Sample |
|---|---|---|---|---|---|---|---|---|---|---|
| Han, et al.18 | Retrospective | 41 | 67 | 68 | Adenocarcinoma | 100 | EGFR | 39 | NA | Tissue and cytology |
| Kang, et al.19 | Prospective | 20 | 72 | 67 | NSCLC | 58 | KRAS | NA | 16 | Tissue and cytology |
| Kim, et al.20 | Retrospective | 107 | 52 | 50 | NSCLC | 85 | EGFR | 44 | NA | Tissue |
| Kim, et al.21 | Prospective | 240 | 63 | 58 | NSCLC | 73 | EGFR | 35 | NA | Tissue |
| Kim, et al.5 | Prospective | 57 | 64 | 39 | NSCLC | 83 | EGFR | 47 | NA | Tissue |
| Lee, et al.22 | Prospective | 61 | 61 | 43 | NSCLC | 82 | EGFR | 62 | NA | Tissue |
| Lee, et al.23 | Prospective | 134 | 63 | 78 | NSCLC | 95 | KRAS | NA | 16 | Tissue and cytology |
| Min, et al.24 | Retrospective | 112 | 64 | 57 | Adenocarcinoma | 100 | EGFR | 52 | NA | Tissue and cytology |
| Yeo, et al.7 | Prospective | 37 | 71 | 70 | NSCLC | 89 | EGFR | 36 | NA | Tissue and cytology |
| Yoon, et al.25 | Prospective | 138 | 66 | 65 | NSCLC | 90 | EGFR | 42 | NA | Tissue and cytology |
![]()
The QUADAS-2 assessment results are summarized in Supplementary Figs. 1 and 2 (only online). Overall, the quality of the included studies was deemed satisfactory. However, the QUADAS-2 tool identified unclear blinding during interpretation of results and a lack of reporting interpretable results as potential sources of bias. In addition, reasons for withdrawal were not clearly explained in some studies, which could have also resulted in bias.
Diagnostic accuracy of PNA clamping and DS for detecting oncogenic alterations
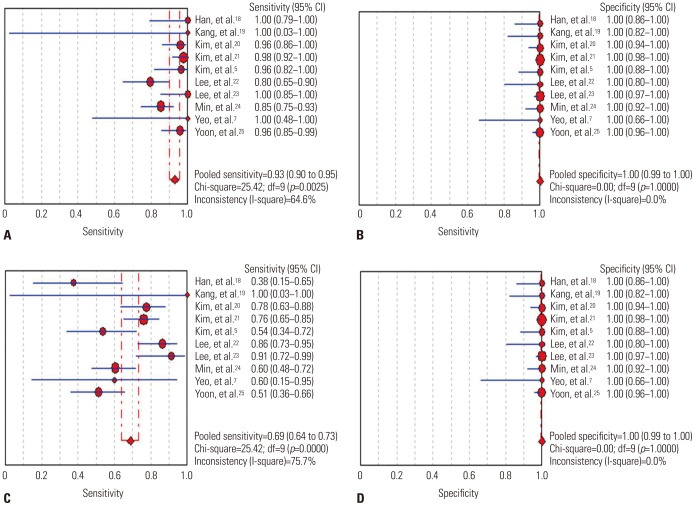
Oncogenic alterations were detected in 340 of 924 cases (36.8%) with PNA clamping and in 250 of 924 cases (27.1%) with DS. With respect to PNA clamping, the pooled sensitivity and specificity for oncogenic alteration detection were 0.93 (95% CI, 0.90 to 0.95; I2=64.6%, p=0.003) and 1.00 (95% CI, 0.99 to 1.00; I2=0%, p=1.000), respectively (Fig. 2A and B). The pooled PLR and NLR were 73.03 (95% CI, 30.50 to 174.85; I2=0%, p=0.885) and 0.08 (95% CI, 0.04 to 0.16; I2=68.9%, p=0.001), respectively. The DOR for PNA clamping was 1138.36 (95% CI, 396.94 to 3264.581; I2=0%, p=0.509). For DS, the pooled sensitivity and specificity for detecting oncogenic alterations were 0.69 (95% CI, 0.64 to 0.73; I2=75.7%, p<0.001) and 1.00 (95% CI, 0.99 to 1.00; I2=0%, p=1.000), respectively (Fig. 2C and D). The pooled PLR and NLR were 52.59 (95% CI, 21.84 to 126.65; I2=0%, p=0.856) and 0.34 (95% CI, 0.24 to 0.47; I2=76.5%, p<0.001), respectively. The DOR for DS was 184.66 (95% CI, 71.22 to 478.81; I2=0%, p=0.623).
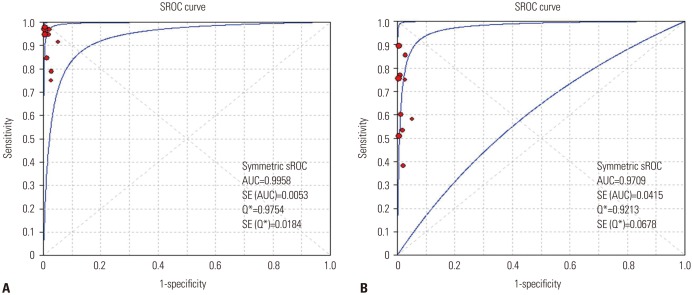
The SROC curves for the PNA clamping and DS tools with respect to predicting oncogenic alterations are shown in Fig. 3. The AUC was 0.996 [standard error (SE)=0.005] for PNA clamping and 0.971 (SE=0.042) for DS. Lastly, although Deeks' funnel plots showed asymmetric, there was no statistically significance of potential publication bias (p=0.07 for PNA clamping and p=0.15 for DS) (Supplementary Fig. 3, only online).
Diagnostic accuracy of PNA clamping and DS for detecting EGFR mutations
We retrieved data on the PNA clamping and DS molecular tests for detecting EGFR mutations from eight trials.57182021222425
EGFR mutations were detected in 316 of 770 cases (41.0%) with PNA clamping and in 228 of 770 cases (29.6%) with DS. For PNA clamping, the pooled sensitivity and specificity for detecting EGFR mutations were 0.92 (95% CI, 0.89 to 0.95; I2=67.8%, p=0.003) and 1.00 (95% CI, 0.99 to 1.00; I2=0%, p=1.000), respectively (Supplementary Fig. 4A and B, only online). The pooled PLR and NLR were 70.70 (95% CI, 26.74 to 186.89; I2=0%, p=0.856) and 0.08 (95% CI, 0.04 to 0.16; I2=72.3%, p=0.001), respectively. The DOR was 1113.71 (95% CI, 359.34 to 3451.76; I2=0%, p=0.546). For DS, the pooled sensitivity and specificity of the detection of EGFR mutations were 0.67 (95% CI, 0.62 to 0.72; I2=75.8%, p<0.001) and 1.00 (95% CI, 0.99 to 1.00; I2=0%, p=1.000), respectively (Supplementary Fig. 4C and D, only online). The pooled PLR and NLR were 47.52 (95% CI, 17.84 to 126.62; I2=0%, p=0.820) and 0.36 (95% CI, 0.27 to 0.49; I2= 76.6%, p<0.001), respectively. The DOR was 145.69 (95% CI, 51.95 to 408.57; I2=0%, p=0.688). The SROC curves for predicting EGFR mutations in the two groups are shown in Supplementary Fig. 5 (only online). The AUCs were 0.993 [standard error (SE)=0.009] for PNA clamping and 0.951 (SE=0.072) for DS.
Meta-regression for PNA clamping in detecting oncogenic alterations
A substantial degree of heterogeneity was founded in the sensitivities and pooled LRs for both groups. Table 2 shows the results of meta-regression analyses for identifying potential sources of heterogeneity with respect to the diagnostic performance of PNA clamping for detecting oncogenic alterations in patients with NSCLC. Specifically, we investigated study design, sample size, age, proportion of males, type of lung cancer, rate of lung adenocarcinoma, and genes analyzed as probable sources of heterogeneity, and there were no significant factors identified.
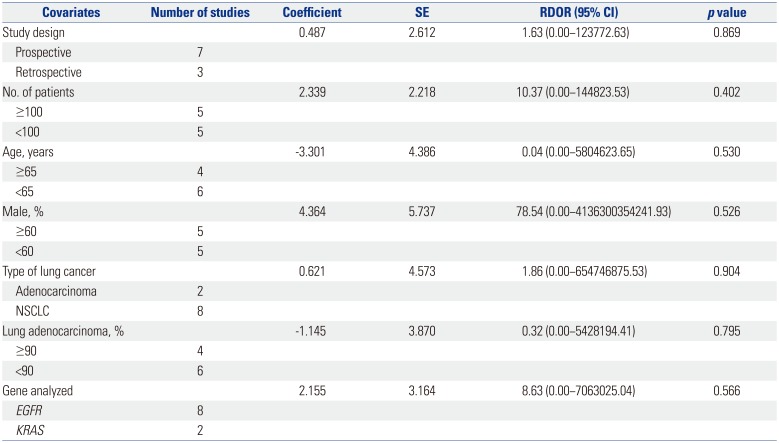
Table 2
Meta-Regression Analysis to Identify Potential Sources of Heterogeneity
![]()
Comparison of clinical responses to EGFR-TKIs according to EGFR mutations detected by PNA clamping and DS
We retrieved data on clinical responses to EGFR-TKIs from seven trials (Fig. 4).571820212225 Objective responses to EGFR-TKIs therapy for patients with EGFR mutations detected by PNA clamping were not significantly different from those of patients with EGFR mutations detected by DS (53.4% vs. 50.8%; RR, 0.99; 95% CI 0.83 to 1.19; I2=0%, p=0.874).
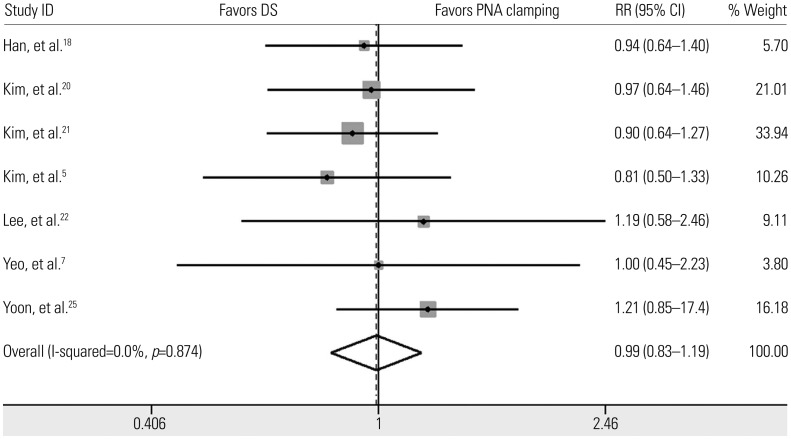
Fig. 4
Pooled results of the response to EGFR-tyrosine kinase inhibitors in EGFR activating mutation-positive non-small cell lung cancer detected by PNA clamping and DS. EGFR, epidermal growth factor receptor; PNA, peptide nucleic acid; DS, direct sequencing; RR, risk ratio; CI, confidence interval.
![]()
DISCUSSION
In the present study, we compared the effectiveness of DS and PNA clamping for predicting oncogenic alterations in patients with NSCLC using a systemic review and meta-analysis approach. Oncogenic alterations were detected in 340 of 924 cases (36.8%) with PNA clamping and in 250 of 924 cases (27.1%) with DS. We found that PNA clamping had a sensitivity of 93% for detecting oncogenic alterations, which was higher than the 69% sensitivity for DS. Subgroup analysis showed that PNA clamping had a sensitivity of 92% for detecting EGFR mutations, which was higher than the 67% sensitivity for DS. Although substantial heterogeneity was identified in the pooled estimates in both groups, potential sources of heterogeneity were not identified in a meta-regression analysis. In addition, there was no evidence of publication bias. Lastly, there was no significant difference in objective responses to EGFR-TKIs treatment between patients whose EGFR mutations were detected by PNA clamping or DS.
Molecular testing for oncogenic alterations has become an essential part of identifying patients eligible for treatment with targeted therapeutic agents. EGFR mutations are representative of treatable oncogenic alterations. Indeed, several randomized control trials have reported that NSCLC patients with EGFR mutations are more responsive to EGFR-TKIs and have a prolonged survival rate, compared to patients with non-mutated EGFR lung cancer.1 Thus, because EGFR mutation is a crucial prognostic biomarker for drug response, efficient detection of EGFR mutations is helpful for prolonging the survival of patients with NSCLC through targeted therapy.
DS can detect mutant DNA comprising ≥25% of the total DNA.26 However, the samples available for mutational analysis in lung cancer are frequently limited due to small tissue biopsy size or use of cytological specimens.18 Our results confirmed that the sensitivity of DS was low for detecting oncogenic alterations in NSCLC, and suggest the need for improved molecular testing methodologies. A number of sensitive detection methods have been developed based on the close relationship between treatable oncogenic alteration status and response to targeted agents. Among these methods, our pooled estimates demonstrated that PNA clamping was more sensitive than DS. In addition, PNA clamping is rapid and simple to conduct, and can detect mutant alleles comprising as little as approximately 1% of mutant alleles.6
Obtaining a sufficient amount of sample is critical for being able to perform both pathologic examination and mutation analysis. However, because many patients with NSCLC have advanced stage disease at the time of diagnosis, they frequently have inoperable disease and poor performance status. Thus, they often are not candidates for surgical treatment or invasive diagnostic procedures, which can often lead to a failure of obtaining a sufficient sample for analysis. Indeed, in some patients, the amount of diagnostic sample or cytological specimen is insufficient to permit additional molecular analysis after routine pathologic examination.19 Considering the frequency at which a very small amount of sample is obtained from NSCLC patients, PNA clamping has the potential to be very useful in clinical settings. Indeed, previous studies have revealed that the diagnostic performance of PNA clamping for detection of oncogenic alterations in NSCLC is favorable for cytology specimens, such as pleural effusions, as well as tumor tissue.719 However, to improve the rate of detection of oncogenic alterations, proper tissue handling, including timing of tissue sample acquisition, shorter fixation time, and DNA quality control, continue to be important.27
EGFR mutations can accumulate during tumor progression; thus, there is potential for heterogeneous EGFR status within tumors. In addition, multiple different EGFR mutations in a single tumor specimen have been reported; for this reason, heterogeneity of EGFR mutations has been suggested as one of the causes of resistance to EGFR TKIs.8910 Such intratumor heterogeneity of EGFR mutations could also partially explain why some patients with wildtype EGFR respond to EGFR-TKIs, whereas some patients with EGFR mutations fail to respond to EGFR-TKIs.18 A prospective study revealed that patients with heterogeneous EGFR mutation status do not respond well to EGFR-TKIs (gefitinib), and experience a significantly reduced time to progression and overall survival after gefitinib treatment, compared to patients with EGFR-mutant tumor cells.9 Because of the high sensitivity of PNA clamping, we were concerned that patients with a low burden of EGFR mutations detected by PNA clamping might also have a lower objective response to EGFR-TKIs than those detected by DS. However, according to pooled estimates, there was no significant difference in objective responses to EGFR-TKIs according to the method of mutation detection.
A recent prospective study reported that heterogeneity of EGFR mutations is extremely rare in lung adenocarcinoma, with the authors instead suggesting that reported findings of heterogeneity are better explain as “pseudoheterogeneity” attributable to mutant-allele specific imbalance and heterogeneously distributed EGFR amplification.11 In addition, because EGFR mutations can be detected in precancerous lesions, a large portion of invasive adenocarcinomas would contain EGFR mutations.11 The clinical implications of the difference between true heterogeneity and pseudoheterogeneity continue to be limited.18 Thus, further studies are needed to determine whether there are differences in other treatable oncogenic alterations detected by either DS or the PNA clamping method and if these are associated with differences in treatment responses to targeted therapy in NSCLC.
To the best of our knowledge, this is the first meta-analysis to compare PNA clamping and DS for predicting oncogenic alterations in NSCLC and to assess potential predictive biomarkers of response for EGFR-TKIs treatment. Our findings could be helpful for physicians implementing PNA clamping in clinical practice. However, there were some limitations to the present study that should be considered when interpreting our results. First, since our meta-analysis was based on a relatively small number of trials, our results should be interpreted with caution due to limited statistical power. Second, there was substantial heterogeneity among the included studies, although large heterogeneities are commonly seen in systematic reviews of studies on diagnostic test accuracy.28 Variations in baseline characteristics of the selected studies could have also potentially introduced heterogeneity. Third, 10 studies are too small to test for funnel plot asymmetry. Although there was no evidence of publication bias according to our analysis using the Deeks' test, the possibility could not be excluded. Considering of potential publication bias for small study effect, we additionally conducted the Begg's test and the Egger's test. For PNA clamping and DS, p-values of the two tests indicated that there also was no publication bias in the meta-analysis (0.592 and 0.691 for the Begg's test and 0.721 and 0.724 for the Egger's test, respectively).
In conclusion, PNA clamping was found to be able to detect oncogenic alterations in an additional 100 out of approximately 920 patients with NSCLC, compared to DS. We demonstrated that PNA clamping had higher sensitivity and accuracy than DS for predicting oncogenic alterations in NSCLC. With respect to objective responses to EGFR-TKIs therapy, there were no significant differences between patients whose EGFR mutations were detected by PNA clamping or DS. Our findings provide evidence that PNS clamping is more useful than DS among the current methods for molecular testing in NSCLC.
 XML Download
XML Download