

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Contrast-induced acute kidney injury (CI-AKI) is a serious complication of percutaneous coronary intervention (PCI) and is associated with both short- and long-term poor outcomes.1234 Diabetes mellitus (DM), chronic kidney disease (CKD), and especially the use of high dose of contrast during PCI are well-known risk factors of CI-AKI.1567891011
The diagnosis and treatment of intracranial aneurysm generally require high dose contrast agent imaging studies. Further, aneurysmal subarachnoid hemorrhages (aSAHs) usually require urgent diagnosis and treatment. Therefore, high dose contrast agents are administered for a relatively short time period to enable rapid critical endovascular treatment. However, only a few recent studies have investigated CI-AKI in aSAH. Thus, the aim of this study was to investigate the incidence and clinical outcomes of CI-AKI after coil embolization in patients with aSAH.
Go to : 
MATERIALS AND METHODS
This retrospective study conducted at a single institution reviewed 225 consecutive patients with aSAH who were treated with coil embolization between January 2005 and March 2016. This study used the institution's neuroendovascular procedure database to systematically review emergency department logs, medical admission records, and the outpatient department's documentation. The patients' initial Glasgow Coma Scale (GCS) score, which was based on emergency department records or admission records, was divided into two groups for statistical convenience. The clinical cutoff point was between GCS 8 and 9, which is considered a severe classification of GCS.1213 To determine serial creatinine values and clinical course, a structured medical record review was performed. Thirty-three patients were excluded because of a lack of creatinine values within 72 hours after coil embolization and for having follow-up durations that were shorter than one year. CI-AKI was defined as an increase from the baseline serum creatinine concentration of >25% or >0.5 mg/dL within 72 hours after coil embolization.1 Estimated glomerular filtration rate (eGFR) was obtained using the equation from the Modification of Diet in Renal Disease formula: eGFR=175× serum creatinine−1.154×age−0.203×(0.742, if female).14
To evaluate outcomes of endovascular aSAH treatment, mortality and functional outcomes at one-year post-treatment were evaluated. One-year mortality was defined as any medically-related death within one year. The modified Rankin Scale (mRS) was used to evaluate functional outcomes. A mRS score of ≥3 at one year was considered poor.
In this study's treatment strategy, all aSAH patients with a cerebral aneurysm confirmed by computed tomography (CT) angiography or magnetic resonance angiography (MRA) received conventional angiography and coil embolization within 24 hours. Non-ionic low-osmolar agents (iopamidol) and an iso-osmolar agent (iodixanol) were used in all angiography procedures. All patients underwent diagnostic non-contrast brain CT and digital subtraction angiography (DSA) before coil embolization. For the brain CT angiography, 90–100 mL of Omnipaque 300 (iohexol) was administered.
This study was approved by Institutional Review Board of our hospital (No. 2017-05-162).
Statistical analysis
Continuous variables are expressed as a mean±standard deviation and were compared using Student's t-test and the Wilcoxon rank sum test. The Mann-Whitney U test was used for ordinary variables. Statistically significant non-categorical variables were dichotomized based on clinical cutoff points or median values. All dichotomized variables were analyzed with the chi-square test and Fisher's exact test. Variables found to be significant through univariate analysis were entered in a multiple logistic regression model based on clinical relevance. A model was constructed using a backward-stepwise multiple logistic regression, and included all clinically relevant variables with a p value <0.2 in the univariate analysis. For all analyses, results are reported as an odds ratio (OR) and 95% confidence interval (CI), and significance was set at a p value of <0.05. Statistical analysis was executed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Go to :
RESULTS
In this study, the mean follow-up duration was 47.1 months (range: 3 days to 143.7 months), and the average length of hospital stay was 27.7 days (range: 3 to 159 days). The mean age at admission was 56.9±13.7 years (range: 22 to 86 years), and 123 (64.1%) of the 192 patients were women. Twelve (6.3%) patients had DM, 70 patients (36.5%) had a history of antihypertensive medication use, and one patient had pre-existing renal disease. Forty-two (21.9%) patients presented with an initial severe GCS score (≤8). Among the included 192 patients, 14 developed CI-AKI (7.3%), and 178 (92.7%) underwent a diagnostic contrast-enhanced imaging study, such as a CT angiography or additional DSA, within 72 hours prior to coil embolization. Fourteen patients did not undergo studies with contrast before endovascular treatments because initial brain CT showed definite aSAH finding, or MRA was replaced with CT angiography. Baseline characteristics of the 192 patients are listed in Table 1.
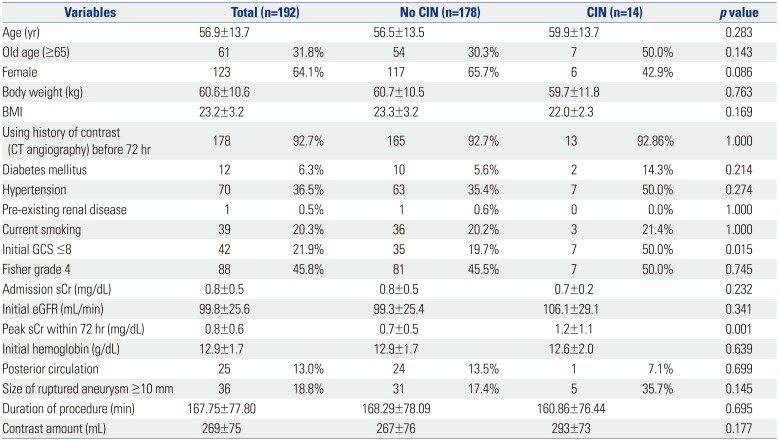
Table 1
Baseline Characteristics and Angiographic Findings
![]()
The CI-AKI group generally demonstrated more severe medical conditions. In the univariate analysis, patients in the CI-AKI group were more likely to have a severe initial GCS score (50.0% vs. 19.7%; p=0.015). In the multivariate analysis, the initial poor GCS score (p =0.013) in the CI-AKI group was statistically significant.
There were no statistically significant difference according to the amount (293±73 mL vs. 267±76 mL; p=0.177) and type (non-ionic low-osmolar 4.5% vs. iso-osmolar 11.3%; p=0.07) of contrast media, duration of the procedure (160.9±76.4 minutes vs. 168.3±78.1 minutes; p=0.695), marginally lower body mass index (22.0±2.3 kg/m2 vs. 23.3±3.2 kg/m2; p=0.169), and large aneurysms (maximal diameter ≥10 mm) (35.7% vs. 17.4%; p=0.145). The CI-AKI group contained more older adult (≥65-years-old; 50.0% vs. 30.3%; p=0.143) and diabetic patients (14.3% vs. 5.6%; p=0.214), although there were no significant differences between the groups.
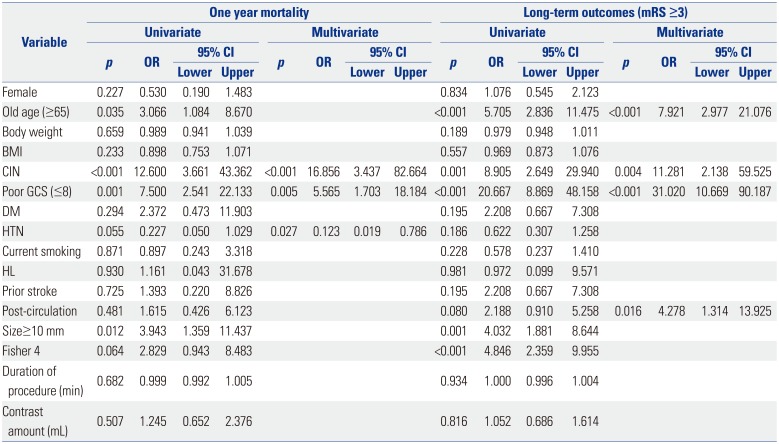
One-year mortality occurred in 16 patients (8.3%): 13 patients died of neuropathology, one patient died of cardiogenic problems, and two patients died of systemic infections. The CI-AKI group had a significantly higher incidence of mortality (37.5% vs. 4.5%; p<0.001) (Fig. 1), poor initial GCS score (62.5% vs. 18.2%; p<0.001), older age (≥65-years-old; 56.3% vs. 29.5%, p=0.028), and large aneurysm ≥10 mm (43.8% vs. 16.5%, p=0.007). In the multivariate analysis, one-year mortality was associated with CI-AKI (p<0.001, OR: 16.85) and severe GCS score (p=0.005, OR: 5.565). History of antihypertensive medication use (p=0.027, OR: 0.123) showed an inverse correlation with mortality (Table 2).
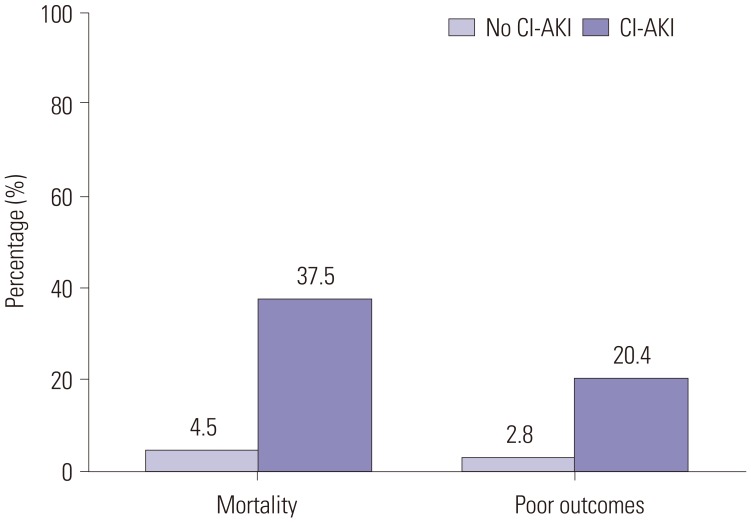 | Fig. 1Mortality and functional outcomes (modified Rankin Scale ≥3) in one-year after coil embolization in patients with aneurysmal subarachnoid hemorrhage. CI-AKI, contrast-induced acute kidney injury.
|
Table 2
Statistical Analysis for All-Cause Death and Long-Term Outcomes in aSAH after Coil Embolization
aSAH, aneurysmal subarachnoid hemorrhage; mRS, modified Rankin Scale; OR, odds ratio; CI, confidence interval; BMI, body mass index; CIN, contrast induced nephropathy; GCS, Glasgow Coma Scale; DM, diabetes mellitus; HTN, hypertension; HL, hyperlipidemia; Prior stroke, history of prior cerebral stroke; Post-circulation, ruptured aneurysm location in posterior circulation; Fisher 4, Fisher grade 4.
![]()
This study also investigated functional outcomes. Considering differences in follow-up duration, the mRS of survivors at one-year after coil embolization was compared with those with a poor functional outcome (mRS ≥3) at one-year after coil embolization for aSAH (49 patients), and was associated with CI-AKI (20.4% vs. 2.8%; p<0.001) (Fig. 1), older age (≥65-years-old; 61.2% vs. 21.7%; p<0.001), poor initial GCS score (63.3% vs. 7.7%; p<0.001), large aneurysm ≥10 mm (36.7% vs. 2.7%; p<0.001), and Fisher grade IV (73.5% vs. 36.4%; p<0.001). In the multivariate analysis, older age (≥65-years-old; p<0.001, OR: 7.921), CI-AKI (p=0.004, OR: 11.281), severe initial GCS score (p<0.001, OR: 31.020), and ruptured aneurysm (p=0.016, OR: 4.278) in posterior circulation were independently associated with a poor long-term outcome (Table 2).
Go to :
DISCUSSION
The reported incidence of CI-AKI after PCI ranges from 2% to 25% (overall, 3.3%) because of diverse pre-existing risk factors and difference in CI-AKI definitions.71516 Recently, known risk factors of CI-AKI have been reported to be DM, CKD, congestive heart failure, acute hypotension, advanced age, ST-elevation myocardial infarction, volume depletion, amount of contrast agent administered, type of contrast agent, and simultaneous use of nephrotoxic medications after PCI procedures.6915 The baseline characteristics of patients with aSAH varied from those of patients with coronary artery disease (CAD). Generally, patients with aSAH are healthy young people. The prevalence of comorbidities of DM, CKD, and heart failure in patients with aSAH is lower than that in patients with CAD.171819 Considering these differences between aSAH and CAD, the amount of contrast agent administered could be a more relevant factor in CI-AKI development in aSAH patients.
A recent study reported that the incidence of CI-AKI after neuroendovascular procedures was 2.5% (4/158) only when the administered volume of contrast was greater than 250 mL.8 In two other studies, the incidence of CI-AKI in patients with aSAH who had undergone at least one contrast study (CT angiography, DSA, or perfusion study) was 2.9% (3/104) and 5.3% (4/75), respectively.2021 Recently, the number of coil embolization cases in patients with aSAH have rapidly increased; yet, there are few cases reporting CI-AKI as a single risk factor after coil embolization for aSAH. In this study, the incidence of CI-AKI after coil embolization was 7.3%, which was slightly higher than the previously published score. Although this study did not have access to the exact amount of contrast agent used in the diagnosis and treatment of aSAH, there were some indirect evidences related with the amount even if there was no statistical significance. Alexopoulos, et al.22 reported there was no difference in the incidence of CI-AKI undergoing a coronary procedure in patients taking non-ionic low-osmolar and iso-osmolar contrast agents. In this study, the incidence of CI-AKI receiving non-ionic low-osmolar versus iso-osmolar contrast media were 11.3% versus 4.5%, although there was no statistical significance for the difference (p=0.075).
According to the 2012 American Heart Association and American Stroke Association Guidelines and the 2013 European Stroke Organization Guidelines, diagnostic work-ups of aSAH include non-contrast head CT, CT angiography, and DSA.1723 These guidelines recommend early diagnosis and treatment to improve the prognosis of patients with aSAH. However, when undergoing endovascular treatment, patients are exposed to extremely high doses of contrast agent in just a few hours, which could lead to the development of CI-AKI. Oleinik, et al.24 reported that CT angiography does not lead to CI-AKI. Yet, the study did not evaluate the probability of subsequent contrast imaging on the increased risk of CI-AKI. In this study, none of the fourteen patients who did not undergo CT angiography developed CI-AKI.
In the cardiovascular field, many believe that the correlation between poor clinical outcomes and CI-AKI are connected with high comorbidity in patients with CI-AKI.6 However, it is doubtful that this explanation could be applied to patients with aSAH, who tend to have fewer underlying diseases. Zacharia, et al.25 reported that renal dysfunction in patients undergoing hospital stay is an independent prognostic factor of aSAH. They also announced that a consistently high relative risk is associated with kidney dysfunction, despite the adjustment for comorbid conditions and initial neurologic severity. Although the mechanism was unclear, additional kidney injury may aggravate the medical condition more than previously thought. Prevention of ischemic conditions with sufficient hydration is important in cases of CI-AKI.2627 The management of CI-AKI in aSAH is rarely reported. However, the usual treatment is hydration using normal saline.28 Although the direct association between CI-AKI and contrast agent usage could not be shown, reducing the total amount of contrast media used in the diagnosis and treatment of aSAH is important.
A premorbid history of hypertension is a known risk factor of aSAH; however, its role as a prognostic factor remains unclear.17232930 A recent study reported that premorbid hypertension is an independent risk factor for a 3-month functional outcome of aSAH.31 However, in this study, the prognostic power appeared weak and the definition of premorbid hypertension was ambiguous. In addition, whether the patients with hypertension were appropriately controlled with hypertensive medication was unclear. In another long-term cohort study, antihypertensive medication was reported to decrease the risk of aneurysm formation.32 In this study, premorbid hypertension was defined as previous treatment with antihypertensive medication and there was an inverse correlation with one-year mortality. Selection errors or varying definitions and criteria may have contributed to the contradicting results among studies. Further investigations are needed to confirm the relationship between premorbid hypertension and CI-AKI.
This non-randomized and retrospective study may have several errors or biases confounding the results. The small number of patients with CI-AKI may increase the possibility of type 1 error. A larger size study would increase the statistical reliability of the associated findings. Further, this study did not involve data on the actual amount of contrast agent used, merely the amount prescribed in the diagnosis and treatment planning.
CI-AKI was shown to be strongly associated with 1-year outcomes of aSAH after endovascular treatment. Further studies are needed to statistically confirm the results and to quantify the relationship between CI-AKI and the total administered contrast volume in patients with aSAH.
Go to :
 XML Download
XML Download