

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stress myocardial perfusion imaging using single-photon emission computed tomography (SPECT) is commonly used for risk stratification and therapeutic decision making in patients with coronary artery disease (CAD).123 Since ischemia is a strong predictor of adverse outcomes, such as death or myocardial infarction (MI),45 detecting ischemia is an important part of the diagnostic strategy for patients with stable CAD. In addition to the diagnostic and prognostic utility of myocardial perfusion SPECT, the extent of ischemia is one of the primary measures that drives decisions regarding revascularization.678 Patients with moderately or severely abnormal myocardial perfusion SPECT have significantly higher mortality rates if treated with medical therapy alone.57 Previous studies on myocardial perfusion SPECT have focused on the prognostic utility of stress imaging as the initial test for patients with CAD.89 However, there are only a few studies that show a relationship between the presence and severity of ischemia and prognosis during CAD treatment.101112 Therefore, according to the current guidelines and appropriate use criteria for follow-up of CAD, routine stress imaging is not recommended, except for special high-risk groups after coronary revascularization.1314 Hence, in the current study, we aimed to assess the clinical implications of serial myocardial perfusion SPECT in patients with CAD who were receiving either medication or revascularization therapy.
MATERIALS AND METHODS
Study population
We identified consecutive patients who underwent serial myocardial perfusion SPECT, had abnormal results on a first study [which was defined as summed stress score (SSS) ≥3],15 and had follow-up adenosine stress SPECT at an interval ≥6 months between the two studies that were performed between January 1, 2000 and June 31, 2014. Patients were also excluded if they had MI <3 months before initial SPECT, previous revascularization therapy, serious non-coronary heart disease, including cancer with a life expectancy less than one year, incomplete nuclear data, multiple coronary revascularizations between the two SPECT procedures, and no clinical follow-up information. As a result, a total of 1153 patients with serial SPECT studies were included (Fig. 1). Because of the retrospective nature of the study, a waiver for individual informed consent was granted by the Institutional Review Board.
Myocardial perfusion imaging
Thallium-201 (Tl-201) SPECT was the default stress myocardial perfusion imaging used during the study period. Images were acquired with a standardized protocol.16 Adenosine was intravenously administered at a rate of 140 mcg/kg/minute for 6 min. Three minutes after the initiation of the adenosine infusion, a dose of Tl-201 (range=92.5–148 MBq, as determined by the patient's body weight) was intravenously injected. Six minutes after adenosine infusion, post-stress myocardial perfusion images were acquired using two-head gamma cameras equipped with low-energy, all-purpose collimators. The specific acquisition parameters were dependent on the camera.
Image interpretation
Semi-quantitative visual interpretation was performed by independent expert interpreters, using 17 segments for the severity and extent of abnormalities on stress imaging.17 Each segment was scored using a 5-point scoring system (0=normal; 1=equiv-ocal; 2=moderate; 3=severe reduction in radioisotope uptake; 4=absence of detectable tracer uptake in a segment), as previously described.18 The score that was summed from the stress scan was defined as the SSS: SSS was determined by adding the scores of the 17 segments on the stress images. The SPECT study was considered to be abnormal if the SSS was 3 or greater. According to the result of follow-up myocardial perfusion SPECT, patients were categorized into normal and abnormal groups.
Procedure and follow-up
Coronary angiography was recommended for patients on the basis of their clinical presentation and the results of the noninvasive stress test. Significant stenosis on coronary angiography was defined as >50% stenosis in an epicardial coronary artery. In patients with significant stenosis, the decision to perform revascularization or medical therapy was at the discretion of the individual cardiologist. Percutaneous coronary intervention (PCI)19 or coronary artery bypass graft (CABG) surgery was performed using standard techniques.20 Medical treatment was performed with a medical regimen that consisted of at least antiplatelet, antianginal, and lipid-lowering therapies.3 After index myocardial perfusion SPECT, patients received either medical treatment or revascularization treatment.
Definitions
The primary outcome of interest was the occurrence of major adverse cardiac events (MACE), which was the composite of all-cause death, nonfatal MI, or unplanned revascularization after follow-up myocardial perfusion SPECT. When patients received multiple serial myocardial perfusion SPECTs, the first follow-up SPECT with an interval of ≥6 months after the index myocardial perfusion SPECT was selected for analysis. An MI was defined as elevated cardiac enzymes (troponin I or myocardial band fraction of creatine kinase) more than the upper limit of the normal value with ischemic symptoms or electrocardiography findings that were indicative of ischemia. After follow-up myocardial perfusion SPECT, any further PCI or CABG (excluding planned staged PCI) was considered an unplanned revascularization. Death, non-fatal MI, and unplanned revascularizations were verified by reviewing medical records.
Statistical analysis
The continuous and categorical covariates are summarized as a mean±standard deviation or count (%). According to the follow-up myocardial perfusion SPECT results, all patients were divided into normal and abnormal groups. The baseline patient characteristics were compared between the two groups using the t test or Fisher exact test for continuous and categorical variables, respectively. The cumulative incidence of MACE for the normal and the abnormal groups was obtained using the Kaplan-Meier method and compared between the two groups using the log-rank test. To examine the effect of abnormal results on MACE and its individual events, the unadjusted and adjusted Cox proportional hazards regression models were fitted. Covariates that were statistically significant in univariate analysis and/or those that were clinically relevant were considered candidate variables for multivariate models. In the Cox model, the proportionality assumptions were assessed using the Scho-enfeld residual test, and no relevant violations were detected.
To reduce treatment selection bias and potential confounding, propensity score (PS)-matching analysis was performed. The PS of obtaining the abnormal myocardial perfusion SPECT results was estimated using the nearest-neighbor matching method with a caliper width of 0.2. The considered variables for the PS were age, sex, body mass index, hypertension, diabetes mellitus, current smoking, hyperlipidemia, prior revascularization treatment, chronic pulmonary disease, chronic renal failure, creatinine, total cholesterol, left ventricular (LV) ejection fraction <50%, and the use of beta blockers, calcium channel blockers (CCB), angiotensin converting enzyme inhibitor (ACEi), angiotensin receptor blocker (ARB) agents, or statins, which are listed in Table 1. In general, covariate balancing was considered to be achieved as long as the absolute standardized difference of the means or proportions was <0.25. In the PS analyses, no violations of covariate balancing were detected (Supplementary Fig. 1, only online). For the PS-matched cohorts, continuous variables were compared using the paired t test or the Wilcoxon signed-rank test, as appropriate, and the categorical variables were compared using the McNemar's or Bowker's test of symmetry, as appropriate. A subgroup analysis was performed according to the treatment groups. Furthermore, univariate and multivariate logistic regression analyses were performed to identify independent clinical predictors of having abnormal results on follow-up myocardial perfusion SPECT. In the multivariable logistic regression, we employed a backward variable selection approach based on the p values. The significance level for staying in the model was set to 0.05. All statistical analyses were performed using SPSS (version 19.0 software; IBM Corp., Armonk, NY, USA) and R software (version 2.13; R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org). Additionally, the R package MatchIt was used to conduct the PS analysis.21 All tests were two-tailed, and p<0.05 was considered statistically significant.
RESULTS
Overall population
Baseline characteristics
The median follow-up interval between the index and follow-up myocardial perfusion SPECT procedures was 474 days [interquartile range (IQR)=243–1107 days]. Abnormal results on follow-up myocardial perfusion SPECT were noted in 591 patients (51.3%). The baseline clinical characteristics and myocardial perfusion SPECT results, according to the results of the follow-up myocardial perfusion SPECT procedures and treatment strategy, are presented in Table 1. The patients in the abnormal group were more likely to be male and have a higher incidence of hypertension, diabetes mellitus, and a low ejection fraction. On myocardial perfusion SPECT, the abnormal group had greater baseline perfusion defects than the normal group. The revascularization therapy group was older and more likely to have diabetes mellitus, greater extent of CAD, and high perfusion defect on the initial myocardial perfusion SPECT (Supplementary Table 1, only online).
Clinical outcomes
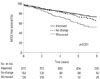
Patients were followed for a median of 6.3 years (IQR=3.7–9.1 years) after the follow-up myocardial perfusion SPECT. During the follow-up period, 188 patients died, 70 patients developed nonfatal MI, and 93 patients underwent unplanned revascularization (Table 2). The incidence of MACE was significantly higher in the abnormal group in the overall population and both treatment groups (Fig. 2), and there was also a significant difference in the clinical outcomes of patients according to the result of serial SPECT (Fig. 3). There was also a tendency for a higher risk of events in patients with abnormal follow-up SPECT in comparison with normal SPECT in all subgroups after adjustment using the multivariate Cox model, as indicated in Table 2.
Propensity-matched population
Baseline characteristics
After performing PS matching, 346, 112, and 212 matched pairs of patients in the overall population, medication alone, and revascularization groups were created, respectively (Table 3). There were no significant differences in the baseline clinical characteristics of the PS-matched patients, except the extent of CAD and the results of SPECT.
Clinical outcomes
In the matched patients, there were 177 MACE events within the median follow-up period of 6.6 years. With respect to the MACE in the matched cohorts, the abnormal group was associated with worse clinical outcomes in the overall population and the revascularization groups (Fig. 4). We noted a consistent pattern in that the abnormal follow-up SPECT group was at a higher risk of MACE and its individual events than the normal group in PS-matched overall patients, medication alone and revascularization groups (Table 4).
Predictors of abnormal follow-up SPECT
Table 5 lists the independent predictors of abnormal results on follow-up SPECT. The variables considered for inclusion in the multivariate models were sex, hypertension, diabetes mellitus, body mass index ≥25 kg/m2, current smoking, chronic kidney disease, history of previous revascularization therapy, LV ejection fraction <50%, treatment with CCB, ACEi, or ARB, and the treatment method. Low ejection fraction was a predictor of abnormal follow-up SPECT, the overall population, medication alone and revascularization groups. Revascularization therapy was a protective factor of abnormal SPECT.
DISCUSSION
In the present study, we evaluated the long-term clinical implications of follow-up SPECT during CAD treatment with comparisons of the clinical outcomes between patients with normal and abnormal follow-up SPECT results. The major findings of this study included the following: 1) abnormal results on follow-up SPECT were associated with worse clinical outcomes, as indicated by an increased risk of death, MI, or unplanned revascularization in the overall study population, and 2) low ejection fraction and medical treatment were independent clinical predictors of having an abnormal result on follow-up SPECT.
Previous randomized studies of serial myocardial perfusion SPECT demonstrated significant reductions in myocardial ischemia after diverse interventions, including the administration of medical therapy or coronary revascularization.2223 In the COURAGE sub-study, residual ischemia was an unadjusted predictor of events, although the noted association was not significant when adjusted for the treatment arm.10 Recent studies have further suggested that a reduction in ischemia on myocardial perfusion SPECT with either medical or coronary revascularization therapy may identify a patient at lower risk for a subsequent cardiac event.1024 Despite the potential advantages of follow-up myocardial perfusion SPECT, clinical practice guidelines and appropriate use criteria do not recommend routine serial testing due to the lack of evidence that supports the benefit of follow-up myocardial perfusion SPECT.1325 A report suggested that >5% worsening ischemia is an independent predictor of death or MI, irrespective of the treatment arm, such as medical therapy or revascularization.26 However, these previous studies were limited by small study populations or case-control designs. Our study, despite its retrospective, single-center, observational study design, is relatively stronger, because it includes a larger study population that was treated at a real-world practice with a longer follow-up period.
The present study demonstrates that follow-up ischemia is associated with adverse outcomes, such as death, MI, and unplanned revascularization. The association between mortality and follow-up ischemia is in line with a previous study that reported that revascularization reduces mortality in patients with an ischemic burden ≥10% on baseline myocardial perfusion SPECT.727 In our study, among the overall population and the revascularization group, abnormal results on follow-up SPECT demonstrated an increased risk of MACE, death, and MI. In the medical group, abnormal SPECT was also associated with a higher risk of MACE and unplanned revascularization. Due to the observational study design, unfavorable clinical factors, such as male sex and lower LV ejection fraction, may contribute to worse clinical outcomes in patients with abnormal follow-up SPECT. However, consistent findings after rigorous adjustment with PS matching support our hypothesis that the prognostic benefit of baseline myocardial perfusion SPECT could be applied to follow-up perfusion SPECT in order to predict long-term clinical prognosis. These results indicate that serial myocardial SPECT after receiving either medication alone or revascularization therapy may be helpful for predicting prognosis and subsequently determining the need for more aggressive treatment.
According to current guidelines, myocardial perfusion SPECT is considered appropriate when symptom recurrence, suspected incomplete revascularization, or ≥5 years after CABG.1328 Therefore, it is of interest to select appropriate patients who can receive myocardial SPECT as a risk assessment modality when they demonstrate the ambiguous presentation of symptoms. Our present findings indicate that abnormal myocardial SPECT results are common in patients with low LV ejection fraction and treatment with medication only. These factors may be indirectly associated with abnormal follow-up SPECT due to the risk of revascularization or decompensated symptoms of CAD.2930 Therefore, our analysis implies that patients with the risk factors for abnormal SPECT are potential candidates who could benefit from receiving follow-up SPECT in order to determine the appropriate treatment strategy.
Our study had some limitations. This was a single-center, observational, retrospective study with the biases that are inherent to this type of analysis. There were also significant baseline differences between patients with normal and abnormal follow-up myocardial SPECT. In addition, patients did not routinely receive serial myocardial perfusion SPECT; rather SPECT was performed at the discretion of the individual physician. Even after statistical adjustment therefore, unobserved confounders might have influenced the results. However, the patients in this study may be representative of a real-world population in daily clinical practice. Finally, due to the small study population, an ischemic threshold on follow-up SPECT for determining clinical prognosis was not evaluated.
In conclusion, abnormal follow-up SPECT results appear to have prognostic implications during CAD treatment in patients receiving either medication alone or revascularization therapy.








 XML Download
XML Download