

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Colorectal cancer (CRC) is the third most common cancer in men and the second most common in women, making it the fourth most common leading cause of cancer-related deaths worldwide.1 Its incidence is rapidly increasing, especially in Asia.234 There is a growing body of evidence supporting the use of novel biomarkers for early detection of CRC.5 Several serum biomarkers have been found to be useful in the management of patients with cancer.6 Tumor markers, such as carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA 19-9), have been extensively evaluated for their efficacy in the diagnosis and management of CRC.6 CEA is the most widely used tumor marker for CRC, because it is expressed at low levels in normal intestinal epithelia but markedly upregulated in most CRC.6,7 CEA affects tumorigenesis by enhancing tumor cell survival and inducing tumor angiogenesis.8 Serum CEA is recommended as a prognostic biomarker for monitoring recurrence of CRC following curative resection, and it can be ordered preoperatively for assistance in staging, surgical planning, and predicting prognosis.9 However, CEA is not recommended as a screening test for CRC.9
CA 19-9 is an antigen defined by monoclonal antibody binding to CA 19-9, the tumor surface marker, Sialyl-Lewis A.10 Serum CA 19-9 is known to be elevated in subjects with various gastrointestinal cancers, such as pancreatic, gastric, hepatic, and biliary tract carcinomas, and it has also been used as a tumor marker of CRC in clinical practice, usually accompanied by CEA.11 Several previous studies have shown that significantly higher concentrations of CEA or CA 19-9 are found in adenoma tissue (which is a precursor of CRC), as well as CRC tissue, in comparison to normal mucosa.121314 A few studies have also investigated the associations between circulating serum CEA or CA 19-9 concentrations and colorectal adenoma.1516 However, these studies included very small sample sizes of fewer than 200 subjects (e.g., n=46–151) and have shown contradictory results.151617 Therefore, the current study aimed to evaluate whether elevated serum CEA and CA 19-9 levels are associated with the presence of colorectal neoplasia (CRN) and whether the levels of these antigens differ according to the severity of CRN in a very large sample of asymptomatic subjects.
MATERIALS AND METHODS
Study population
We retrospectively analyzed data obtained from a prospectively established cohort. The study population consisted of asymptomatic subjects who had undergone colonoscopy and serum CEA/CA 19-9 as part of a comprehensive health screening program at Kangbuk Samsung Hospital, Seoul, Korea, from 2010 to 2014 (n=172960). In Korea, the Industrial Safety and Health Law requires employees to participate in annual or biennial health examinations. About 80% of the participants were employees of various companies and local governmental organizations and their spouses, with the remaining participants registering individually for the program. Serum CEA and CA 19-9 have not been recommended as screening tests for CRC because the sensitivities of serum CEA and CA 19-9 for detecting CRC are very low. However, as part of their welfare policy, companies often subsidize comprehensive health exams including tumor markers, such as CEA and CA 19-9, regardless of current guidelines. Before subjects underwent colonoscopy, interviews were conducted by general practitioners to ensure that all participants were asymptomatic (i.e., no lower abdominal pain or hematochezia). Individuals with intestinal symptoms were urged to seek medical care.
For this analysis, the exclusion criteria were as follows: repeated data from subjects who underwent more than two colonoscopies (n=17923); poor bowel preparation (n=14088); lack of an adequate biopsy (n=229); history of CRC or colorectal surgery (n=428); history of other malignancy, including gastric cancer, liver cancer, lung cancer, thyroid cancer, prostate cancer, breast cancer, and cervix cancer, which could affect serum CEA and CA 19-9 levels (n=2198); history of inflammatory bowel disease (n=229); and missing data on serum CEA (n=13356) or serum CA 19-9 (n=22032). Finally, the total numbers of subjects eligible for the study were 124509 with measured serum CEA and 115833 with measured serum CA 19-9 (Fig. 1). Poor bowel preparation was defined as “large amounts of solid fecal matter found, precluding a satisfactory study; unacceptable preparation; <90% of mucosa seen.”18
This study was approved by the Institutional Review Board of Kangbuk Samsung Hospital.
Measurements and definitions
Data on medical history and health-related behaviors were collected through a self-administered questionnaire, while physical measurements, such as height and weight, were obtained by trained staff members. Smoking status was categorized as never, formerly, or currently, and family history of CRC was defined as CRC in one or more first-degree relatives at any age. Self-reported use of nonsteroidal anti-inflammatory drugs (NSAIDs) (regular use over the previous month) was also assessed. History of colorectal polyps was defined as a self-reported experience in which subjects had undergone removal of one or more colorectal polyps.
Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or current use of antihypertensive medication. Diabetes mellitus was defined as fasting blood glucose ≥126 mg/dL, hemoglobin A1c ≥6.5%, or current use of insulin or antidiabetic mediations. Obesity was defined as a body mass index (BMI) ≥25 kg/m2, which is the proposed cut-off for the diagnosis of obesity in Asians.19 BMI was calculated by dividing the measured weight (kg) by the square of the height (m2).
The presence or absence of fatty liver was examined through abdominal ultrasonography (US). A diagnosis of fatty liver was made on the basis of four known criteria: hepatorenal echogenic contrast, liver brightness, deep attenuation, and vascular blurring.20 Abdominal US was performed using a 3.5-MHz transducer (Logiq 9; GE Healthcare, Madison, WI, USA) by experienced radiologists who were unaware of the study aims and blinded to clinical information.
The serum CEA and CA 19-9 levels were determined using an electrochemiluminescence immunoassay (Modulator E170; Roche Diagnostics, Tokyo, Japan). Abnormal (elevated) serum CEA and CA 19-9 levels were defined as levels above 4.7 ng/mL and 26.6 U/mL, respectively.
Colonoscopy and histologic examination
Colonoscopy was performed by experienced gastroenterologists, who had performed at least 1000 colonoscopies, using an EVIS LUCERA CV-260 colonoscope (Olympus Medical Systems, Tokyo, Japan). All participants took 4 L of polyethylene glycol solution for bowel preparation.
All specimens obtained from biopsy, polypectomy, or endoscopic mucosal resection were evaluated by experienced gastrointestinal pathologists via histopathological examination. Advanced adenoma was defined as the presence of one of the following features: >10 mm diameter, tubulovillous or villous structure, or high-grade dysplasia (HGD).21 High-risk adenoma was defined as advanced adenoma or three or more adenomas. 21 Advanced CRN (ACRN) was defined as a cancer or advanced adenoma, and overall CRN was defined as a cancer or any adenoma.
Statistical analysis
Data are expressed as a mean±standard or frequency (%). Comparison of the prevalence of colorectal lesions between subjects with normal and abnormal ranges of serum CEA and CA 19-9 was performed using chi-squared analysis.
To evaluate whether abnormal levels of serum CEA and CA 19-9 were independently associated with a higher risk of ACRN and overall CRN, multivariate logistic regression analysis was performed. We estimated the adjusted odds ratio (AOR) with 95% confidence intervals (CIs) for the association of abnormal levels of serum CEA and CA 19-9 with the presence of ACRN and overall CRN after adjusting for potential confounding variables, including age, sex, smoking status, family history of CRC, use of NSAIDs, obesity, fatty liver, hypertension, and diabetes mellitus.
The sensitivity, specificity, positive predictive value, negative predictive value, and corresponding 95% CIs of abnormal levels of serum CEA and CA 19-9 in predicting ACRN and cancer were calculated. The area under the receiver operating characteristic curve (AUROC) of abnormal levels of serum CEA and CA 19-9 for detecting ACRN and cancer was also calculated.
All of the reported p-values are two-tailed, and p values <0.05 were considered statistically significant. SPSS Version 21 (IBM Corp., Armonk, NY, USA) was used for statistical analyses.
RESULTS
Baseline characteristics and colonoscopic/histologic findings of the study population according to serum CEA/CA 19-9 concentrations
Among 124509 participants with measured serum CEA levels, a total of 90 CRCs (0.1%) and 2282 ACRNs (1.8%), as well as 19932 overall CRNs (16.0%), were detected. Among 115833 participants with measured serum CA 19-9 levels, a total of 78 CRCs (0.1%) and 2027 ACRNs (1.7%), as well as 18233 overall CRNs (15.7%), were detected.
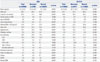
Comparisons of baseline characteristics and colonoscopic/histologic findings of the study population according to serum CEA and CA 19-9 concentrations are summarized in Table 1. The mean age was significantly higher in subjects with serum CEA in the abnormal range (>4.7 ng/mL) than in those with serum CEA in the normal range (≤4.7 ng/mL). The proportion of participants with male sex, status as a current or ex-smoker, and a history of colon polyps, obesity, fatty liver, hypertension, or diabetes mellitus was higher in subjects with serum CEA in the abnormal range than in those with serum CEA in the normal range.
For CA 19-9, mean age was higher in subjects with serum CA 19-9 in the abnormal range (>26.6 U/mL) than in those with serum CA 19-9 in the normal range (≤26.6 U/mL). The proportion of participants with NSAID use, hypertension, and diabetes mellitus was significantly higher in subjects with serum CA 19-9 in the abnormal range, whereas the proportion of participants with male sex, status as a current or ex-smoker, obesity, and fatty liver was higher in subjects with serum CA 19-9 in the normal range.
The prevalence of any adenoma (30.4% vs. 15.7%, p<0.001), low-grade dysplasia (LGD; 29.9% vs. 15.3%, p<0.001), HGD (0.2% vs. 0.1%, p=0.024), adenoma larger than 10 mm (4.4% vs. 1.7%, p<0.001), advanced adenoma (4.5% vs. 1.7%, p<0.001), high-risk adenoma (8.2% vs. 2.6%, p<0.001), cancer (0.4%, vs. 0.1%, p<0.001), ACRN (4.8% vs. 1.8%, p<0.001), and overall CRN (30.6% vs. 15.7%, p<0.001) was significantly increased in subjects with CEA in the abnormal range, compared to those with CEA in the normal range. In addition, the prevalence of HGD (0.2% vs. 0.1%, p=0.031), adenoma larger than 10 mm (2.5% vs. 1.6%, p=0.001), advanced adenoma (2.5% vs. 1.7%, p=0.001), high-risk adenoma (3.7% vs. 2.6%, p<0.001), cancer (0.2% vs. 0.1%, p=0.001), and ACRN (2.6% vs. 1.7%, p<0.001) was significantly increased in subjects with CA 19-9 in the abnormal range, compared to those with CA 19-9 in the normal range (Table 1).
Risk of colorectal neoplasm according to presence of abnormal serum CEA/CA 19-9 concentrations
We further performed multivariate logistic regression analysis to identify whether abnormal serum CEA/CA 19-9 concentrations were independently associated with the risk of CRN. In multivariate analysis adjusted for age, sex, smoking status, family history of CRC, NSAID use, obesity, fatty liver, hypertension, and diabetes mellitus, abnormal CEA concentration was identified as an independent predictor of both ACRN (AOR, 1.46; 95% CI, 1.18–1.80; p=0.001) and overall CRN (AOR, 1.31; 95% CI, 1.18–1.44; p<0.001). In addition, abnormal CA 19-9 concentration was identified as an independent predictor of ACRN (AOR, 1.33; 95% CI, 1.01–1.75; p=0.045) (Table 2).
To reduce errors in interpreting statistically significant results in this very large sampled data, we further performed a 1:1 case-control study (2457 subjects with abnormal CEA vs. 2457 subjects normal CEA and 2657 subjects with abnormal CA 19-9 vs. 2657 subjects normal CA 19-9), which matched sex and age (Supplementary Table 1 and 2, only online). The results were similar to those in the analysis of all participants.
We calculated the diagnostic performance and AUROC of CEA, CA 19-9, and combination of CEA and CA 19-9 for detecting ACRN and CRC. The sensitivities of CEA, CA 19-9, and combination of CEA and CA 19-9 for detecting ACRN were 5.1, 3.4 and 7.7%, respectively, and those for detecting CRC were 11.1, 7.7, and 19.5%, respectively (Supplementary Table 3, only online). The AUROCs of CEA for ACRN and CRC were 51.6 (95% CI, 50.4–52.8) and 54.6 (95% CI, 48.2–61.0), respectively. The AUROCs of CA 19-9 for ACRN and CRC were 50.6 (95% CI, 49.3–51.9) and 52.7 (95% CI, 46.0–59.4), respectively. The AUROCs of combined CEA and CA 19-9 for ACRN and CRC were 51.9 (95% CI, 50.6–53.3) and 57.9 (95% CI, 50.7–65.0), respectively.
Subgroup analysis according to severity of colorectal neoplasia among patients with colorectal neoplasia
We performed subgroup analysis according to severity of CRN among patients with CRN (Table 3). The proportions of abnormal serum CEA concentrations in patients with adenoma larger than 10 mm, three or more adenomas, and ACRN were significantly higher than in those with adenoma less than 10 mm, one or two adenomas, and non-ACRN, respectively. In addition, patients with adenoma larger than 10 mm, HGD, three or more adenomas, and ACRN had a higher proportion of abnormal CA 19-9 concentrations than those with adenoma less than 10 mm, LGD, one or two adenomas, and non-ACRN, respectively.
DISCUSSION
This large-scale study including 124509 and 115833 asymptomatic screened subjects investigated the association between serum CEA/CA 19-9 concentrations and the presence of CRN. We found that elevated serum CEA concentrations were associated with a higher rate of any adenoma, advanced adenoma, high-risk adenoma, ACRN, and overall CRN, as well as CRC. Additionally, we found that elevated serum CA 19-9 concentrations were associated with a higher rate of advanced adenoma, high-risk adenoma, and ACRN, as well as CRC. Further, elevated CEA and CA 19-9 levels were identified as independent predictors of ACRN, and elevated CEA was identified as an independent predictor of overall CRN. More importantly, subgroup analysis among patients with CRN showed that the proportions of elevated CEA and CA 19-9 concentrations were significantly higher in patients with ACRN than in those with non-ACRN. Both elevated serum CEA and CA 19-9 levels were correlated with larger lesion size and multiplicity of adenomas. In other words, serum CEA and CA 19-9 levels reflected the severity of CRN.
Serum CEA and CA 19-9 are elevated in patients with CRC, and they have been used as tumor markers for CRC.6717 In addition, a few studies have attempted to identify the association between serum CEA, CA 19-9, and colorectal adenoma, which is a precursor of CRC.1516 A German study including 32 patients with colorectal adenoma and 119 healthy subjects showed that neither the size of colorectal adenomas nor their histologic severity influences serum CEA concentration.15 However, a Croatian study including 46 patients with colorectal adenoma reported that elevated serum CEA concentrations were associated with larger adenomas, although they were not associated with multiplicity or degree of dysplasia.12 An Israeli study involving 93 patients with colorectal adenoma also demonstrated an increased association of elevated serum CEA with larger tumor size (>2.3 cm in diameter) and adenoma with villous component, but not with severe dysplasia or carcinoma in situ.16 However, the aforementioned previous studies included very small numbers of study participants (n<200). Hence, these studies showed inconsistent results and are limited in terms of the definite conclusions that can be drawn from them. The present study, which included a very large number of subjects, may provide more reliable results than these previous studies. In our study, both elevated serum CEA and CA 19-9 levels were significantly associated with larger lesion size and multiplicity of adenomas.
The underlying biologic mechanisms for increased CEA and CA 19-9 in colorectal adenoma are not fully understood. Fischbach and Mössner13 revealed an increase in tissue concentrations of CEA and CA 19-9 progressing from normal colonic mucosa through colorectal adenomas to carcinomas. They also showed that, in the adenoma group, CEA concentrations increase with increasing villous component and with the extent of cellular atypia present, reflecting their special position in the adenoma-carcinoma sequence. These results supported the biological significance of CEA and CA 19-9 in carcinogenesis of CRC and its precursors. Previous studies have suggested that release of tumor antigens out of tumor tissue may be associated with tumor vascularity, extent of tumor necrosis, the activity of tumor cells as measured by the number of mitotic figures, or tumor differentiation.13 Increases in vascularity, the extent of necrosis, and the degree of cellular atypia in malignant transformation process may explain the noted increases in serum CEA and CA 19-9 in colorectal adenoma. Given that the risk of malignant transformation is associated with size, the extent of villous component, and the degree of cellular atypia of adenoma,22 serum CEA and CA 19-9 levels may be also associated with these factors. Indeed, our study showed that both elevated serum CEA and CA 19-9 levels were correlated with larger lesion size and multiplicity of adenoma.
CEA and CA 19-9 have not been recommended as screening tests for CRC.9232425 The main reason is that the sensitivities of serum CEA and CA 19-9 for detecting CRC are very low.11242526 In the present study, the sensitivities of CEA, CA 19-9, and combination of CEA and CA 19-9 for CRC and ACRN were very low, with results comparable to those in previous studies.1124252627 Additionally, the AUROCs of CEA, CA 19-9, and combination of CEA and CA 19-9 for CRC and ACRN were low. These results support that CEA and CA 19-9 should not be recommended as screening tests for CRC. Although serum CEA and CA 19-9 have not been recommended as screening tests for CRC,9 serum CEA and CA 19-9 testing is frequently conducted as part of a health screening program in Korea. In fact, upon completing the screening program, it is not uncommon for asymptomatic subjects with elevated serum CEA and CA 19-9 levels to be referred to tertiary hospitals for further evaluation, and in this clinical situation, clinicians agonize about whether they should recommend confirmatory colonoscopy for these individuals. Given that the probabilities of ACRN in patients with elevated serum CEA and CA 19-9 levels were only 5.1% (117/ 2282) and 3.4% (68/2027), respectively, it may be unreasonable to recommend confirmatory colonoscopy for all patients with elevated serum CEA or CA 19-9 concentrations. However, the present study showed that elevated serum CEA and CA 19-9 levels were independent predictors of ACRN. Although CEA alone or CA 19-9 alone is inappropriate as screening tests for CRC, they may be useful as an adjunct to other screening methods, such as fecal immunochemical test or clinical risk scoring. Further studies are needed to determine whether serum CEA and/or CA 19-9 are useful as an adjunct to cancer or ACRN detection.
In our study, the average age of the subjects was 41 years, and a relatively large group of young subjects were included. Given that the incidence of CRC is increasing in younger individuals aged <50 years,2829 who have been found to reports concerns for primary screening with colonoscopy and its low cost-effectiveness, tumor markers such as CEA or CA 19-9 may be useful as an adjunct to CRC screening for some young adults at high risk for ACRN.
In the current study, patients with elevated CA 19-9 concentrations had a significantly higher rate of ACRN, but not overall CRN. Meanwhile, patients with elevated CEA concentrations had a significantly higher rate of both ACRN and overall CRN. These results suggest that serum CEA better reflects the presence of overall CRN, compared with serum CA 19-9.
There are several limitations in the present study. First, this was a retrospective study with a corresponding potential bias in design. However, we think that there may be minimal selection bias, because our cohort was established prospectively. Second, our cohort was recruited at two medical examination centers in Korea. Therefore, there was likely some degree of selection bias.
In conclusion, both elevated serum CEA and CA 19-9 levels were associated with the presence of ACRN, as well as CRC. Elevated CEA levels were also associated with the presence of overall CRN. Elevated serum CEA and CA 19-9 levels were significantly correlated with larger lesion size and multiplicity of adenomas.



 XML Download
XML Download