

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Iron deficiency anemia (IDA) occurs in 2–5% of adult men and postmenopausal women in the developed world,12 and it is one of the common indications for referral to gastroenterologists.3 While the most common cause of IDA in premenopausal women is menstrual blood loss, the major cause of IDA in adult men and postmenopausal women is occult gastrointestinal (GI) bleeding.4567 IDA is considered as an alarm sign for the presence of serious GI disease, because a substantial proportion of patients with asymptomatic GI cancer and precancerous lesions may present with IDA.8910 Colorectal cancer (CRC) is one of the most important causes of IDA and is estimated to be found in 4–16% of patients with IDA.311
Occult GI bleeding may be indicated by a positive result on fecal immunochemical test (FIT), which has been developed to selectively recognize unnoticeable bleeding from colorectal origin.61213 CRC screening with FIT has proven to be an effective, non-invasive method for detecting the majority of CRC cases in asymptomatic populations and reducing the mortality of patients with CRC.1415 Accordingly, FIT has been widely adopted as a CRC screening tool.16
Recently, some studies have reported that subjects with both IDA and positive FIT results have an increased risk of CRC.1718 Based on the results of those studies, we hypothesized that participants with positive FIT results and IDA would have a high percentage of advanced colorectal neoplasia (ACRN) on colonoscopy. If our hypothesis is correct, a combination strategy of FIT and hemoglobin level (IDA) would be helpful in the selection and prioritization of asymptomatic participants for colonoscopy. This combination strategy may be useful, particularly in countries with limited colonoscopy resources. However, data regarding this topic are limited. Therefore, in this study, we aimed to evaluate whether a combination strategy of FIT results and IDA is useful for risk stratification for ACRN in a large sample of asymptomatic male subjects.
Go to : 
MATERIALS AND METHODS
Study population
We retrospectively analyzed data from a prospectively established cohort. The present study population consisted of asymptomatic male participants who underwent both FIT and colonoscopy as part of a comprehensive health screening program at Kangbuk Samsung Hospital, Seoul and Suwon, Korea, from 2010 to 2014 (n=21646). The screening program aimed to promote health through regular medical checkups and to enhance early detection of existing diseases. In Korea, the Industrial Safety and Health Law requires employees to participate in annual or biennial health examinations. About 80% of the participants comprised employees of various companies and local governmental organizations and their spouses, while the remaining participants had registered individually for the program. Prior to colonoscopy, interviews by general practitioners were conducted to ensure that all participants were asymptomatic (i.e., no lower abdominal pain, hematochezia). Participants who had overt GI symptoms were urged to seek medical care.
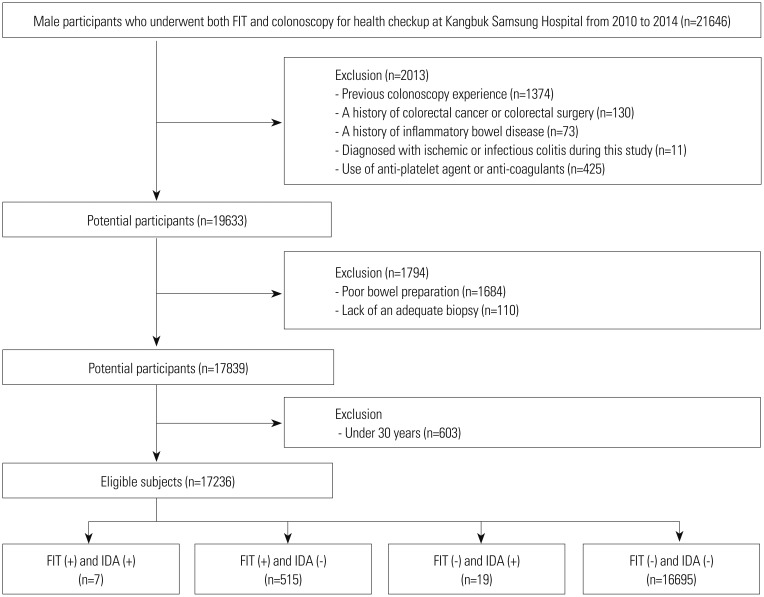
The exclusion criteria for participation in the study were as follows: previous colonoscopy experience (n=1374), a history of CRC or colorectal surgery (n=130), a history of inflammatory bowel disease (n=73), diagnosed with ischemic or infectious colitis during the study (n=11), use of anti-platelet agent or anti-coagulant (n=425), poor bowel preparation (n=1684), inadequate biopsy (n=110), and subjects aged <30 years (n=603). Finally, the total number of eligible subjects for the study was 17236 (Fig. 1). Poor bowel preparation was defined as “large amounts of solid fecal matter found, precluding a satisfactory study; unacceptable preparation; <90% of mucosa seen.”19
In our cohort, most women (80%, n=5393/6774) were premenopausal. In other words, the major cause of IDA in 80% of women in our cohort was menstrual bleeding, but not GI bleeding. Therefore, we did not include female subjects.
This study was approved by the Institutional Review Board of Kangbuk Samsung Hospital, which exempted the requirement for informed consent as we only accessed de-identified data retrospectively.
Measurements and definitions
Data on medical history and health-related behaviors were collected through a standardized, self-administered questionnaire. Physical measurements, such as height and weight, were performed by trained staff. The participants' smoking status was categorized into never, formerly, or currently, and family history of CRC was defined as CRC in one or more first-degree relatives at any age. Self-reported use of nonsteroidal anti-inflammatory drugs (NSAIDs), anti-platelet, or anticoagulant (regular use over the previous month) was also assessed.
Hypertension was defined as a systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or current use of antihypertensive medication. Diabetes mellitus was defined as a fasting blood glucose ≥126 mg/dL, hemoglobin A1c ≥6.5%, or current use of insulin or antidiabetic medications. Obesity was defined as body mass index (BMI) ≥25 kg/m2, which is the proposed cut-off for obesity diagnosis in Asians.20 BMI was calculated by dividing the measured weight (kg) by the square of the height (m2).
Fecal immunochemical test
A one-time stool sample was collected by participants in a sampling tube (Eiken Chemical Company, Tokyo, Japan) containing 2.0 mL of buffer designed to minimize hemoglobin degradation at home within 3 days before initiating bowel cleansing for colonoscopy. The collected fecal material, sealed in a plastic bag, was sent to the laboratory. Fecal hemoglobin concentration was quantitated using OC-SENSOR DIANA™ (Eiken Chemical Company), and FIT results were expressed in nanograms of hemoglobin per milliliter of buffer (ng Hb/mL). The FIT-positivity cutoff value was 100 ng Hb/mL (equivalent to 20 micrograms of hemoglobin per gram of feces).22
Colonoscopy and histologic examination
All colonoscopies were performed using the EVIS Lucera CV-260 colonoscope (Olympus Medical Systems, Tokyo, Japan) by experienced board-certified endoscopists. All participants took 4 L of polyethylene glycol solution for bowel preparation.
All endoscopically detected polypoid lesions were biopsied or removed. All specimens obtained from biopsy, polypectomy, or endoscopic mucosal resection were evaluated by experienced GI pathologists via histopathological examination. Polyps were classified by number, size, and histologic characteristics (tubular, tubulovillous, or villous adenoma; hyperplastic polyp; inflammatory polyp; and sessile serrated adenoma or traditional serrated adenoma). Pathologic results of the hyperplastic polyps, inflammatory polyps, or lipomas were considered normal findings. Advanced adenoma was defined as the presence of one of the following features: >10 mm diameter, tubulovillous or villous structure, and high-grade dysplasia.23 Colorectal neoplasia (CRN) was defined as a cancer or any adenoma, and ACRN was defined as a cancer or advanced adenoma.24 For patients with multiple neoplasms, the most advanced lesion was reported (e.g., adenoma with the greatest diameter or the most serious histology).
Statistical analysis
Data are expressed as mean±standard or frequency (%). The prevalences of cancer, ACRN, and non-advanced CRN according to FIT result and presence of IDA were compared using chi-square test or Fisher's exact test.
The sensitivity, specificity, positive predictive value (PPV), negative predictive value, and corresponding 95% confidence intervals (CIs) of FIT and IDA in predicting ACRN and cancer were calculated. The area under the receiver operating characteristic curve (AUROC) of FIT and IDA for detecting ACRN and cancer was also calculated. We determined whether statistically significant differences exist among the diagnostic strategies using chi-squared test of homogeneity of areas.
All of the reported p values are two-tailed, and p values <0.05 were considered to be statistically significant. SPSS version 21 (IBM Corp., Armonk, NY, USA) was used for statistical analyses.
Go to :
RESULTS
Baseline characteristics of the study population
A total of 17236 male subjects were eligible for the analysis (Fig. 1). Baseline characteristics of the study population are summarized in Table 1. The mean age of the study participants was 40.8 years, and the proportions of subjects aged 30–39, 40–49, and ≥50 years were 48.2, 40.1, and 11.7%, respectively. The proportions of subjects with smoking, family history of CRC, NSAIDs use, and obesity were 65.6, 3.4, 3.2, and 41.5%, respectively. Among 17236 participants, 522 (3.0%) showed positive FIT results (≥100 ng Hb/mL) and 26 (0.2%) had IDA. The prevalences of cancer, ACRN, non-advanced CRN, and overall CRN were 0.1, 1.9, 16.4, and 18.3%, respectively.
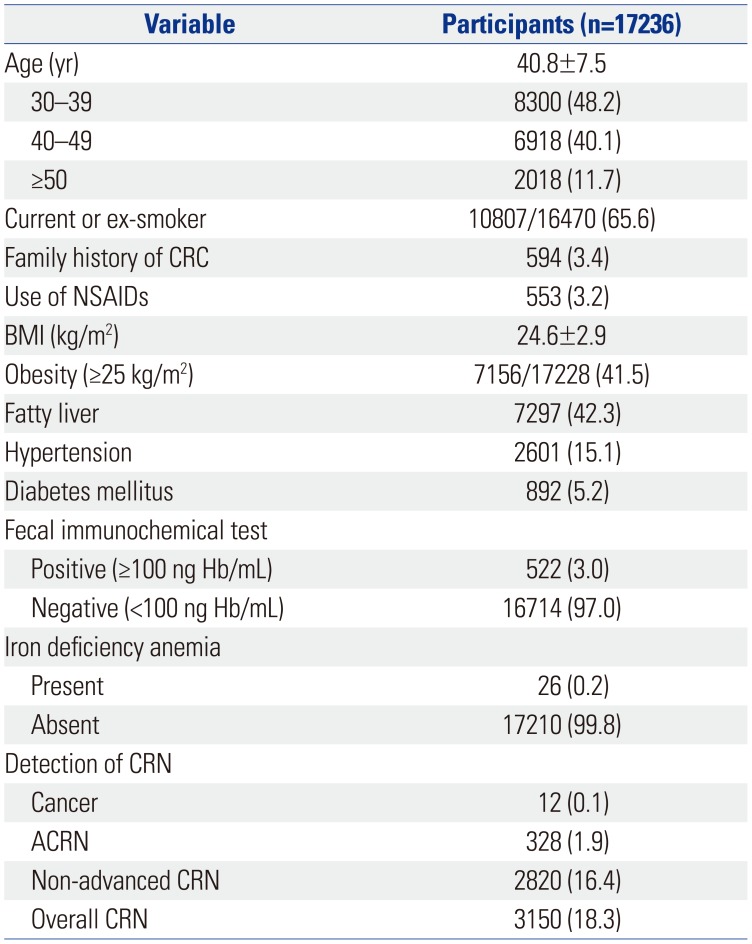
Table 1
Characteristics of the Study Population
![]()
Prevalence of CRN according to FIT result and presence of IDA
The prevalences of CRN according to FIT result and presence of IDA are compared in Table 2. The prevalence of cancer was significantly higher in subjects with positive FIT result (1.9% vs. 0.01%, p<0.001) and IDA (7.7% vs. 0.1%, p<0.001) than in those with negative FIT result and no IDA, respectively. The prevalence of ACRN was also higher in subjects with positive FIT result (13.6% vs. 1.5%, p<0.001) and IDA (11.5% vs. 1.9%, p=0.013) than in those with negative FIT result and no IDA, respectively. The prevalence of non-advanced CRN was lower in subjects with IDA than in subjects without IDA (0.0% vs. 16.4%, p=0.015), while it was not different significantly between subjects with positive vs. negative FIT result (19.3% vs. 16.3%, p=0.061).
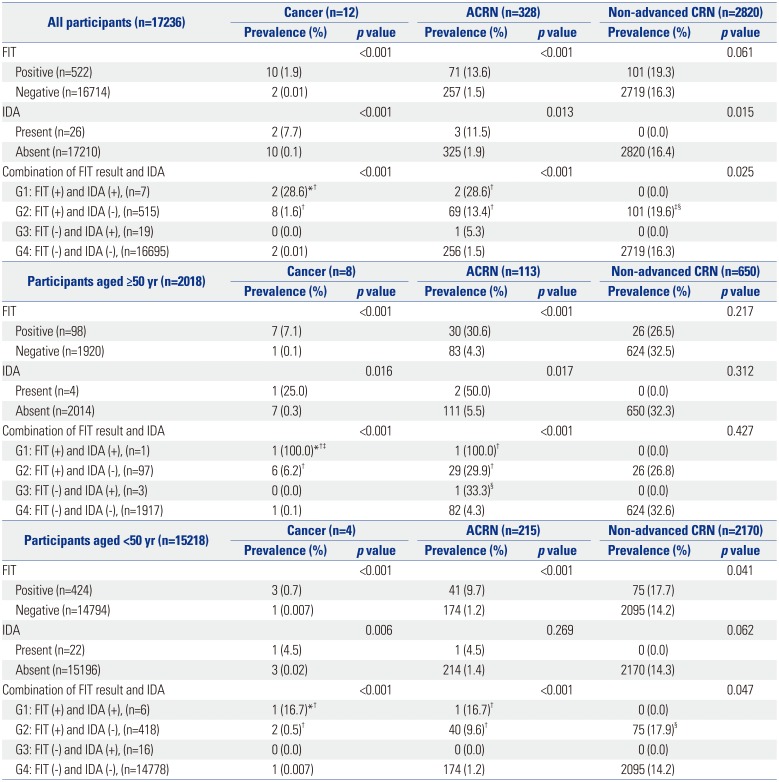
Table 2
Prevalence of CRN According to FIT Result and Presence of IDA
CRN, colorectal neoplasia; ACRN, advanced colorectal neoplasia; FIT, fecal immunochemical test; IDA, iron deficiency anemia.
Values are presented as numbers and percentages.
*Indicates statistically significant from G2 (p<0.001), †Indicates statistically significant from G4 (p<0.001), ‡Indicates statistically significant from G3 (p<0.05), §Indicates statistically significant from G4 (p<0.05).
![]()
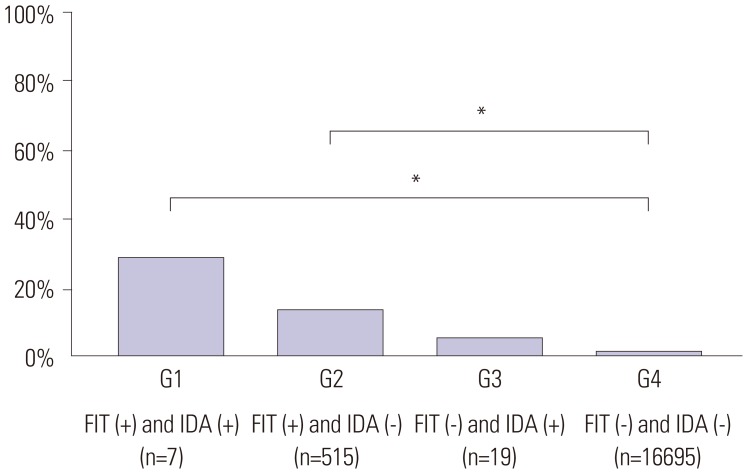
The participants were classified into four groups stratified by FIT results and the presence of IDA. Subjects with positive FIT result and IDA were assigned to group 1 (G1, n=7); subjects with positive FIT result and no IDA, group 2 (G2, n=515); subjects with negative FIT result and IDA, group 3 (G3, n=19); and subjects with negative FIT result and no IDA, group 4 (G4, n=16695). The prevalences of ACRN in G1, G2, G3, and G4 were 28.6, 13.4, 5.3, and 1.5%, respectively (p<0.001). Subjects with both positive FIT result and IDA (G1) had a higher prevalence of ACRN than the other groups. In post-hoc analysis, the prevalence of ACRN was significantly higher in G1 and G2 than in G4, respectively (all p<0.001) (Fig. 2). The prevalences of cancer in G1, G2, G3, and G4 were 28.6, 1.6, 0.0, and 0.01%, respectively (p<0.001). Subjects with both positive FIT result and IDA (G1) also showed a higher prevalence of cancer than the other groups. The prevalence of non-advanced CRN was higher in subjects with positive FIT result and no IDA than in other groups (0.0, 19.6, 0.0, and 16.3% in G1, G2, G3, and G4, respectively; p=0.025).
We further analyzed subjects aged ≥50 and <50 years, respectively (Table 2). Among subjects aged ≥50 years, the prevalences of ACRN in G1, G2, G3, and G4 were 100% (n=1/1), 29.9% (n=29/97), 33.3% (n=1/3), and 4.3% (n=82/1917), respectively (p<0.001), and those for CRC were 100% (n=1/1), 6.2% (n=6/97), 0.0% (n=0/3), and 0.1% (n=1/1917), respectively (p<0.001). Among subjects aged <50 years, the prevalences of ACRN in G1, G2, G3, and G4 were 16.7, 9.6, 0.0, and 1.2%, respectively (p<0.001) and those for CRC were 16.7, 0.5, 0.0, and 0.007%, respectively (p<0.001). In other words, subjects with positive FIT results and IDA had an increased risk of ACRN and CRC in subjects aged <50 years as well as ≥50 years.
Table 3 shows the diagnostic performance of FIT and IDA for ACRN and cancer. As mentioned above, a combined strategy of FIT results and IDA had higher PPV than FIT alone and IDA alone. The sensitivities of FIT for ACRN and CRC were 21.6 and 83.3%, respectively, while the sensitivities of IDA for ACRN and CRC were 0.9 and 16.7%, respectively. The sensitivities of the combination strategy of FIT and IDA for ACRN and CRC were 0.6% (n=2/328) and 16.7% (n=2/12), respectively.
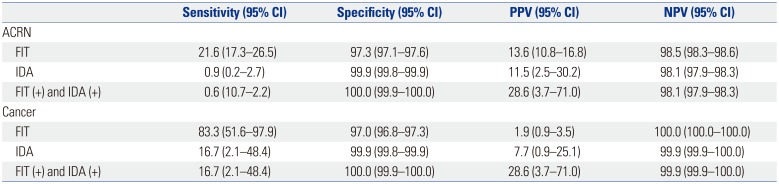
Table 3
Diagnostic Performance of FIT and IDA for ACRN and Cancer
![]()
We also calculated the AUROC of FIT and IDA for detecting ACRN and cancer. The AUROCs of FIT, IDA, and combination strategy of FIT and IDA for ACRN were 59.5 (95% CI, 57.3–61.7), 50.4 (95% CI, 49.9–50.9), and 59.6 (95% CI, 57.3–61.9), respectively (p<0.001). The AUROCs of FIT, IDA, and combination strategy of FIT and IDA for cancer were 90.2 (95% CI, 79.2–100.0), 58.3 (95% CI, 47.3–69.3), and 90.4 (95% CI, 79.3–100.0), respectively (p<0.001). In post-hoc analysis, the AUORCs of combination strategy of FIT and IDA for ACRN and cancer were significantly higher than those for IDA, but they were not significantly different to those for FIT.
We did not include female subjects, because most of them (80%, n=5393/6774) were premenopausal. However, we further compared the prevalence of ACRN among four groups stratified by FIT results and the presence of IDA in postmenopausal female subjects (n=1381). As a result, the prevalences of ACRN in G1, G2, G3, and G4 were 100% (n=1/1), 16.7% (n=8/48), 0.0% (n=0/32), and 2.6% (n=34/1300), respectively (p<0.001).
Go to :
DISCUSSION
To the best of our knowledge, this study is the first to compare the prevalences of ACRN and CRC among four groups stratified by FIT results and the presence of IDA. This large-scale study of 17236 asymptomatic men showed that patients with both positive FIT results and IDA had the highest rate of ACRN and CRC. The prevalences of ACRN among patients with positive FIT result/IDA, positive FIT result/no IDA, negative FIT result/IDA, and negative FIT result/no IDA were 28.6, 13.4, 5.3, and 1.5%, respectively, and those for CRC were 28.6, 1.6, 0.0, and 0.01%, respectively. Our findings suggest that subjects with positive FIT results with IDA should be considered a higher priority for colonoscopy. A combination strategy of FIT results and hemoglobin level (IDA) may be useful for risk stratification for detecting ACRN.
IDA is a common medical condition encountered in clinical practice and accounts for approximately one-half of all anemia cases.2526 The etiologies of IDA differ with age and gender, and chronic occult GI bleeding is the most common cause of IDA in adult men and postmenopausal women. CRC is one of the most important causes of IDA, and approximately 11–57% of patients with CRC present with IDA.1727 Additionally, several studies have shown that patients subsequently diagnosed with CRC who first present with IDA typically have worse staging and mortality and that pre-existing IDA is an independent factor associated with poor survival outcomes in patients with CRC.282930 Therefore, when IDA is diagnosed in adult men and postmenopausal women, clinicians should carefully consider the possibility of undiagnosed CRC and need to recommend colonoscopy.30 However, IDA is investigated sub-optimally in general practice. Several studies have reported that only 19–31% of patients with IDA receive colonoscopic evaluation,313233 which may be attributed to limited colonoscopy resources.
FITs use specific antibodies that selectively react with the globin moiety of the human hemoglobin and detect the colonic blood with great sensitivity.634 Globin is rapidly degraded by proteases during its passage through the GI tract. Thus, FIT does not detect small amounts of blood from the upper GI tract and selectively recognizes occult bleeding of colorectal origin.612 Given these characteristics, FIT has been widely adopted as a CRC screening tool,16 and it has been proven to detect a large portion of CRC cases in asymptomatic average-risk populations.1415
Based on the findings of previous studies, we speculate that a combination strategy of FIT results and IDA may be useful for selecting participants who are highly likely to have CRC or ACRN. Similar to our expectation, the highest rates of CRC and ACRN were found in patients with both positive FIT result and IDA. In accordance with the present investigation, a Japanese study reported that the detection rates of CRC were 13, 8.3, 0.4, and 0.1% in patients with positive FIT result and IDA, those with positive FIT result and no IDA, those with negative FIT result and IDA, and those with negative FIT result and no IDA, respectively.17 The study demonstrated that patients with both positive FIT results and IDA had the highest rate of CRC and suggested that colonoscopy is necessary, particularly in cases with positive FIT result and IDA.17 However, this study focused on CRC only and did not provide data regarding ACRN. Additionally, the substantial proportion of subjects were premenopausal women in whom the major cause of IDA is menstrual bleeding, but not GI bleeding. Recently, another study, including 140 IDA patients without overt bleeding, demonstrated that potential GI lesions including CRC are frequently detected in FIT positive-IDA patients than in FIT negative-IDA patients (33.3% vs. 8.7%, p=0.001).18 However, this study included a small number of subjects and compared the prevalence of potential GI lesions according to FIT results only among patients with IDA.
Contrary to the results of CRC or ACRN, the prevalence of non-advanced CRN was lower in patients with IDA than in those without IDA, and it was highest in subjects with positive FIT result and no IDA. These findings suggest that IDA shows no predictability for non-advanced CRN. Additionally, considering that patients with positive FIT result and no IDA had a higher rate of ACRN than those with negative FIT result and IDA, although without statistical significance, FIT appears to better reflect the presence of ACRN than hemoglobin level.
Although the PPV of the combination strategy of FIT results and IDA for ACRN and CRC was higher than that of FIT alone and IDA alone, the sensitivities of IDA (0.9% for ACRN and 16.7% for CRC) and the combination strategy of FIT and IDA (0.6% for ACRN and 16.7% for CRC) were lower than that of FIT (21.6% for ACRN and 83.3% for CRC). This is because the proportion of patients with IDA was very small. In addition, the AUROC of the combination strategy of FIT and IDA (90.4) and FIT alone (90.2) for CRC was high, whereas that of IDA alone was low (58.3). Our results suggest that hemoglobin level (IDA) is inappropriate for screening test and that it should be used as an adjunct to FIT.
Our study showed that subjects with positive FIT results and IDA had an increased risk of ACRN and CRC in subjects aged <50 years as well as ≥50 years. Although the prevalence of ACRN in subjects aged <50 years was lower than that in subjects aged ≥50 year, given that the incidence of CRC is increasing in young populations,3536 a combination strategy of FIT results and IDA may be useful for some young adults at high risk for ACRN (such as smoker or obese person). Primary screening with colonoscopy, however, is difficult to implement in young populations.
The present study has three limitations. First, this study was hospital-based rather than population-based, and our cohort was recruited at two medical centers in Korea. Therefore, selection bias may occur to some extent. Second, we adopted a one-specimen FIT; thus, the sensitivity of FIT for detecting ACRN may have been underestimated. Third, the proportion of patients with IDA is very small and patients with both positive FIT results and IDA are also very rare. These results raise concerns for the usefulness of additive serology test (IDA), and further consideration for cost-effectiveness is needed. Finally, our cohort included relatively young participants (the proportion of participants aged <50 years was 88%). Care must be taken when making generalizations from our results.
In conclusion, subjects with positive FIT results with IDA had an increased risk of ACRN and CRC. Our results suggest that subjects with positive FIT results and IDA should be considered higher priority for colonoscopy. A combination strategy of FIT results and the presence of IDA may be helpful in the selection and prioritization of asymptomatic men for colonoscopy.
Go to :
 XML Download
XML Download