

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spatial hearing refers to the ability to understand speech and identify sounds in various environments. Spatial hearing includes sound localization, understanding speech in a noisy background, and estimating the distance of the sound origin.12 There are many factors that affect spatial hearing, including the severity and symmetry of a hearing impairment. Basic characteristics, such as age, can affect spatial hearing, even in normal hearing children, because of developmental difference.3 The interaural time difference and interaural level difference can also affect spatial hearing.4 Spatial processing problems can be caused by peripheral hearing loss, central hearing loss, and impaired cognitive function.567
The Spatial Hearing Questionnaire (SHQ) is a 24 question self-report with eight subscales. The subscales test male, female, and children's voices; music in quiet; source localization; understanding speech in quiet; understanding speech in noise with target and noise sources from the front; and understanding speech in noise with spatially separate target and noise sources.2
Although there are many subjective questionnaires that assess spatial hearing, the Speech Spatial and Qualities of Hearing Scale (SSQ) is a representative questionnaire.8 However, the SSQ consist of 49 questions, compared to 24 questions in the SHQ, and the SSQ takes more time than the SHQ. Furthermore, there is a high degree of correlation between SHQ and SSQ scores,910 suggesting the possibility of extrapolating the results from one questionnaire to the other. Also, the SHQ has subscales that focus on important listening situations. To create a Korean language spatial hearing scale, we concluded that the SHQ was a better choice than the SSQ.
Although the original version of the SHQ was developed in English, the SHQ has been translated and validated in other languages, including Dutch, Persian, French, and Chinese.11121314 In this study, we assessed the validity of a Korean version of the SHQ (K-SHQ) and compared the results of the K-SHQ to different classifications of hearing loss.
MATERIALS AND METHODS
The Korean version of Spatial Hearing Questionnaire
The original English version of the SHQ consists of 24 questions. Each item is scored from very difficult (0) to very easy (100). With the SHQ, a higher score reflects a better ability to hear. An English-Korean bilingual otologist performed forward translation from English to Korean. The naive Korean version of SHQ was then reviewed by a doctor of Korean literature. Next, the questionnaire was back translated into Eng-lish by a different English-Korean bilingual otologist. A doctor of English literature reviewed the back-translated questionnaire, comparing it to the original version of the SHQ and recommended minor changes. Finally, the K-SHQ was developed (Supplementary Table 1, only online).
Subjects
Power analysis was performed to determine the sample size (effect size 0.810, alpha value 0.05, power 0.8). Forty-eight patients who visited the Yonsei University Wonju Severance Christian Hospital and completed the pure tone audiometry (PTA) test were enrolled in the study. All patients independently answered each question in the K-SHQ. There was no reported difficulty, and participants received no help in answering questions. Patients who use hearing aids were instructed to answer to each question as if they were not using their hearing aid(s).
Since altered cognitive function can affect spatial hearing, patients also completed the Mini-Mental State Examination (MMSE). Patient with an MMSE score of less than 24 were excluded from the study. Patients who could not read and understand the Korean-language were also excluded. Demographic information, including academic background, was collected. Information from medical records, including hypertension, diabetes, pulmonary or cardiac disease, cerebrovascular accident, chronic kidney disease, liver disease, and otologic surgery, was also collected. Previous exposure to noise in a job environment and hearing aid use were noted.
The Institutional Review Board of Yonsei University Wonju Severance Christian Hospital approved this study (YWMR-15-1-109).
Auditory evaluation
Patients underwent auditory testing using PTA, at the Department of Otorhinolaryngology-Head and Neck Surgery. Testing was performed in a double walled, single room audio booth using established standards (ANSI 3.6 type 1 pure tone audiometer, 1989; IEC 645-1 type 1 pure tone audiometer, 1992).
Pure-tone thresholds were obtained for air conduction at 250, 500, 1000, 2000, 4000, and 8000 Hz. Audiologic data were reported in accordance with the methods recommended by the Hearing Committee of the American Academy of Otolaryngology Head and Neck Surgery. The average PTA was calculated using the following formula: [(500 Hz+1000 Hz+2000 Hz+4000 Hz)/4].
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences Software (SPSS 22.0 for Windows; SPSS Inc., Chicago, IL, USA). Cronbach's alpha and item-total correlation were measured to evaluate internal consistency. We used the Kaiser-Meyer-Olkin (KMO) test to measure sampling adequacy. A KMO value is considered good if it is greater than 0.70 and excellent if it is greater than 0.90. When the KMO value is good, factor analysis can be performed. We performed factor analysis, and the number of factors was determined using the eigenvalue and scree plot curve. Varimax rotation was used to simplify the interpretation of data.
To compare continuous variables, an independent t-test and correlation analysis were performed. Chi-square or Fisher's exact test were performed to analyze categorical variables. All p values less than 0.05 were considered significant.
RESULTS
Reliability
For the K-SHQ, Cronbach's alpha was 0.982, suggesting good internal consistency in the Korean-language questionnaire. We also assessed item-total correlation coefficients, which ranged from 0.686 to 0.910 (Supplementary Table 2, only online).
Factor analysis
Factor analysis was used to group questionnaire items with similar features. The KMO value was 0.839, indicating that factor analysis was appropriate for this data.
The number of factors was determined using eigenvalues and a scree plot curve. Two factors had eigenvalues greater than 1 (Supplementary Table 3, only online) and explained 70.60% and 9.97% of all items of K-SHQ. Factor 1 included 12 items, questions number 1 to 12 from the questionnaire. These items are related to understanding speech and music in a quiet and in a noisy environment. Factor 2 included another 12 items, from questions number 13 to 24. These items are related to understanding and locating the origin of sound when the origin cannot be seen (Table 1).
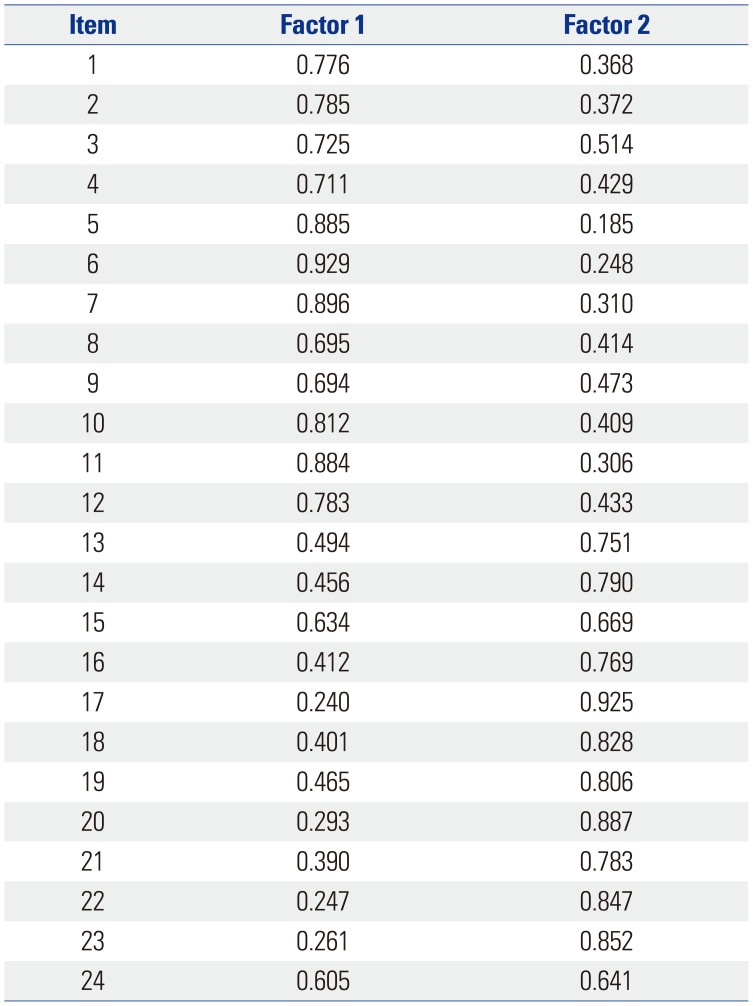
Table 1
Two K-SHQ Factors Identified by a Rotated Component Matrix
![]()
The communality values, which describe the amount of variance of an item as predicted by the loading factor, ranged from 0.654 to 0.924. It is generally considered that each item loads well on a factor when the value of communality is greater than 0.45 (Supplementary Table 4, only online).
Construct validity
Construct validity was assessed by comparing K-SHQ scores from patients with normal hearing to those with a hearing impairment. Of the 48 patients, 17 patients had normal hearing, and 31 patients were hearing impaired. Baseline characteristics are shown in Table 2. Mean hearing threshold was significantly different in the hearing-impaired patients, compared to those with normal hearing. There were no other differences in patient baseline characteristics. Table 3 also shows there were no differences in patient medical characteristics. The mean SHQ score and all subscale scores were significantly different when patients with normal hearing were compared to those with hearing impairment (Table 4).
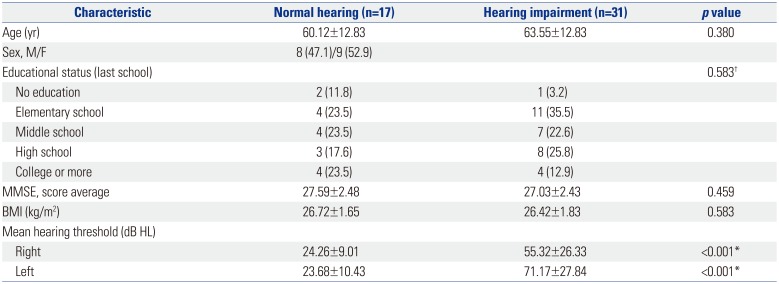
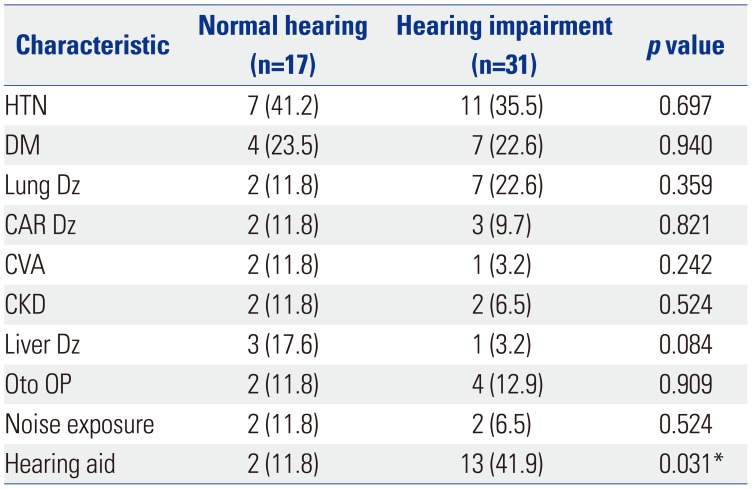
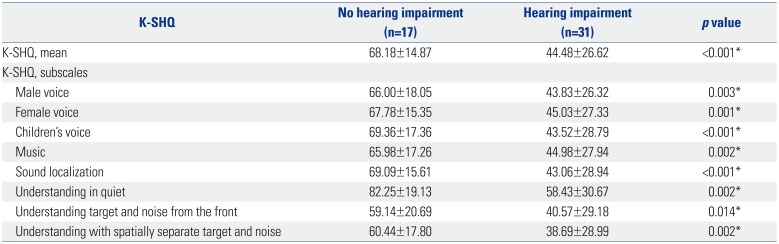
Table 2
Baseline Characteristics of the Study Participants
![]()
Table 3
Medical Characteristics of the Study and Control Groups
![]()
Table 4
Mean Scores of the K-SHQ and K-SHQ Subscales in the Study and Control Groups
![]()
We divided patients with a hearing impairment into unilateral and bilateral hearing loss. Of the 31 patients with a hearing impairment, 12 had unilateral hearing loss, and 19 had bilateral hearing loss. Since patients with unilateral hearing loss benefit from the ability to hear normally in one ear, they were expected to have better K-SHQ scores than those with bilateral hearing loss. There was a significant difference in average scores for K-SHQ and all subscales between patients with unilateral and bilateral hearing loss (Table 5).
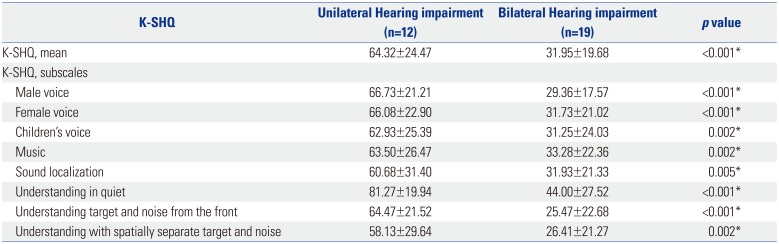
Table 5
Mean Scores of the K-SHQ and K-SHQ Subscales for Participants with Unilateral and Bilateral Hearing Loss
K-SHQ, Korean version of the Spatial Hearing Questionnaire; PTA, pure tone audiometry.
Unilateral hearing impairment: mean hearing threshold (dB HL) of 40 decibels with four-frequency average of PTA in one ear. Bilateral hearing impairment: 40 dB HL of four-frequency average of PTA in both ears. Values are expressed as mean±standard deviation.
*p value<0.05.
![]()
Since spatial hearing is associated with not only the severity of hearing impairment but also with binaural hearing, we divided patients with hearing impairment into two groups based on the symmetry of hearing function. We defined hearing symmetry as an interaural difference of less than 15 dB of the average value of PTA. If the differences between the two ears was greater than 15 dB, it was considered asymmetric. Sixteen patients had symmetric hearing and 15 patients had asymmetric hearing (Table 6). Patients with asymmetric hearing loss had significantly better spatial hearing ability, compared to patients with symmetric hearing loss.
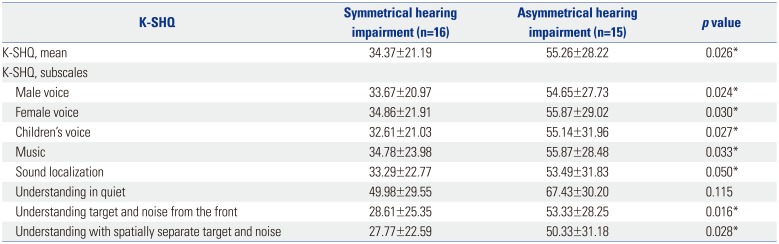
Table 6
Mean Scores of the K-SHQ and K-SHQ Subscales for Participants with Symmetric and Asymmetric Hearing Loss
K-SHQ, Korean version of the Spatial Hearing Questionnaire; PTA, pure tone audiometry.
Symmetric hearing impairment: The difference between the two ears is less than 15 dB of the average value of PTA. Asymmetric hearing impairment: the differences between the two ears is greater than 15 dB of the average value of PTA. Values are expressed as mean±standard deviation.
*p value<0.05.
![]()
DISCUSSION
A measurement of internal consistency, such as Cronbach's alpha, is required to validate the translation of a questionnaire.10 Dutch, French, Chinese, and Persian versions of the SHQ reported Cronbach's alpha of 0.98 or greater.11121314 In our study, Cronbach's alpha was 0.982, suggesting good internal consistency.
The item-total correlation coefficients of K-SHQ ranged from 0.686 to 0.910. This indicates that all individual items correlated well with the total score.11121314 The item-total correlation coefficients for the other language versions of the SHQ were similar to those of our study: Dutch (0.65 to 0.90), French (0.63 to 0.88), Chinese (0.75 to 0.92), and Persian (0.84 to 0.92).11121314 The original English SHQ reported item-total correlation coefficients from 0.41 to 0.88.2
Factor analysis was used to assess the internal structure of the K-SHQ, and two factors were identified according to eigenvalues. Each factor consisted of 12 items from the questionnaire, with a serial rule. Factor 1 included understanding speech and music in quiet and in noise, while factor 2 included understanding and locating the origin of sound when the origin cannot be seen. In the other language versions of the SHQ, scores loaded on two to four factors, and in the original version of SHQ, scores loaded on three factors.211121314 Since it is important to assess a patient's spatial hearing in specific conditions, the original SHQ was developed with 8 subscales, and the mean score of each subscale is a useful clinical tool.
The average K-SHQ score in patents with a hearing impairment was lower than that for patients with normal hearing. We also determined that if a patient with a hearing impairment had normal hearing in one ear, the patient had better spatial hearing. The K-SHQ score for patients with unilateral hearing impairment was higher than the score for patients with bilateral hearing impairment.
Spatial hearing is co-influenced by many factors, including the severity and symmetry of the hearing impairment.67 It is expected that the more severe the hearing loss, the lower the K-SHQ. In addition, asymmetric hearing loss was expected to lower K-SHQ scores, since impaired interaural time and level differences can affect spatial hearing. However, in our results, patients with asymmetric hearing loss had higher K-SHQ scores than patients with symmetric hearing loss. This is in contrast to previous reports.1214 Potvin, et al.12 reported that patients with asymmetric hearing loss had lower SHQ scores than patients with symmetric hearing loss. No significant difference in Fletcher index (FI) was found when patients with the best hearing were compared to patients with the poorest hearing. However, the FI of the worst ear was significantly lower in patients with asymmetrical hearing loss, when compared to those with symmetric hearing loss.12 In our study, the mean threshold of PTA in patients with asymmetric hearing impairment was lower in the better ear and higher in the worse ear, indicating a wide gap in hearing threshold between both ears, when compared to those with symmetric hearing impairment. This difference was significant (in the better ear: asymmetric=39.73±19.14 vs. symmetric=56.71±16.29; in the worse ear: asymmetric=92.25±26.03 vs. symmetric=62.66±17.38; p<0.005). Our study suggests that the hearing ability of the better ear is a more important factor than the difference in hearing ability between ears. Fig. 1 shows that the better the hearing ability of the less impaired ear, the higher the K-SHQ score. However, lower K-SHQ scores did not differ significantly in relation to hearing ability between ears.
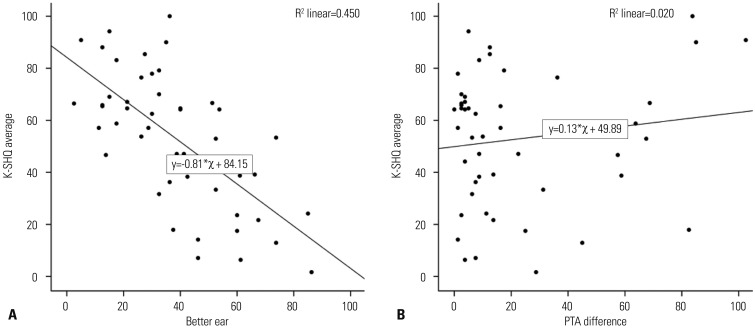
Fig. 1
Correlation of the mean K-SHQ score and hearing features of the better ear. (A) Hearing ability of the better ear is well correlated with the mean K-SHQ score. The worse the hearing ability of the better ear, the lower the K-SHQ score. (B) PTA difference between ears is not well correlated with K-SHQ score. PTA, pure tone audiometry; K-SHQ, Korean version of the Spatial Hearing Questionnaire.
![]()
Generally, both hearing loss severity and bilateral symmetry are considered similarly important factors, and the relative importance of each might depend on listening situations, degree of hearing loss, and degree of asymmetry. The effect of hearing asymmetry on spatial hearing is manifested when the hearing ability of better ears are similar. However, we did not determine the contribution of the severity of hearing impairment and hearing asymmetry on spatial hearing.
Binaural hearing is important in sound localization and speech perception in a noisy environment. However, binaural hearing is less important in understanding in a quiet background.15 In this study, understanding in quiet was the only construct that was not statistically different between patients with symmetrical and asymmetrical hearing loss.
In conclusion, the K-SHQ is a reliable and valid tool with which to assess spatial hearing in people who can read the Korean language. The K-SHQ accurately reflects the severity and symmetry of hearing impairment. In patients with hearing impairment, the mean PTA of the better ear correlates more with spatial hearing than with asymmetry of hearing. However, bilateral symmetry of hearing is also considered an important factor of spatial hearing. Further study is needed to identify how the severity and asymmetry of hearing impairment contribute to spatial hearing.
 XML Download
XML Download