

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most humeral shaft fractures can be treated using the functional bracing method.1 Surgery is considered when this conservative treatment fails to maintain the stability of reduction, open fracture, or other combined injuries. Many surgical techniques have been introduced to correct humeral shaft fractures, and there have been debates regarding their clinical indications.2 One of the standard surgical treatments is closed reduction and internal fixation using antegrade intramedullary nails. This technique has several potential advantages over other methods, including open reduction and internal fixation with plates, in terms of reduced disruption to the surrounding soft tissue and greater preservation of extramedullary vascularity around the fracture site.23 However, it can be difficult to perform a closed reduction or obtain the required stability from fixation with an intramedullary nail in highly unstable fractures of the humeral shaft in which there are complex or severely-displaced fragments, and such difficulties could result in delayed union or non-union of the bone fragments.4 Manipulation during cl-osed reduction can lead to the development of iatrogenic radial nerve palsy, since the lateral intermuscular septum fixes the radial nerve in fractures of the distal humerus.5 Therefore, in unstable humeral fractures, we have performed open reduction and internal fixation using one or two cerclage cables followed by an intramedullary nail to gain greater stability. Cerclage cables have been commonly used to fix periprosthetic fractures following total knee or hip arthroplasties at the femur or tibia, since they are particularly useful in the long bones that are occupied with the intramedullary stem.678 In addition, cerclage cables are used for subtrochanteric femur fractures treated with intramedullary nails and have provided satisfactory clinical results.9 There may be concern about delaying the bone union or increasing nonunion caused by cerclage cables in humeral shaft fracture, for the cables have been shown to affect periosteal circulation in a cadaveric study.10
To the best of our knowledge, there has been no previous study evaluating the clinical results of the open cerclage cable technique followed by intramedullary nailing (IMN) in humeral shaft fractures. Therefore, the purpose of this study was to compare the clinical results between two surgical techniques in humeral shaft fractures: the open cerclage cable technique followed by IMN and the conventional closed nailing technique. Our hypothesis was that one or two cerclage cables applied after open reduction would not delay bone union in patients with an unstable humeral shaft fracture treated with antegrade intramedullary nails, compared to the closed nailing technique. Moreover, this technique could provide similar functional results and postoperative complications to the closed nailing technique.
MATERIALS AND METHODS
We examined the medical records of 232 patients who had undergone surgery for humeral diaphyseal fractures from January 2001 to January 2014. Patients who had received internal fixation with an antegrade intramedullary nail were included in this study. All patients were aged 18 years or older. The exclusion criteria included an open or pathologic fracture, treatment by a plate or bone graft, revision surgery or surgery combined with preoperative nerve palsy, and an ipsilateral fracture in the upper extremities. Patients who were lost to follow-up within 1 year of surgery or who died as a result of combined injuries prior to documentation of fracture union were also excluded. After applying these criteria, a total of 96 patients were included in the study and were divided into two groups. One group had surgery with open reduction and internal fixation using one or two cerclage cables combined with an antegrade intramedullary nail (cable group; n=32), while the second group was treated with the conventional technique of closed reduction and internal fixation with an intramedullary nail (non-cable group; n=64).
Background data were recorded for each of the enrolled patients, including age, gender, injury type (such as high or low energy), smoking history, and fracture type. Fracture types were classified using the Orthopaedic Trauma Association/AO Foundation (OTA/AO) 12-diaphyseal humerus classification.11
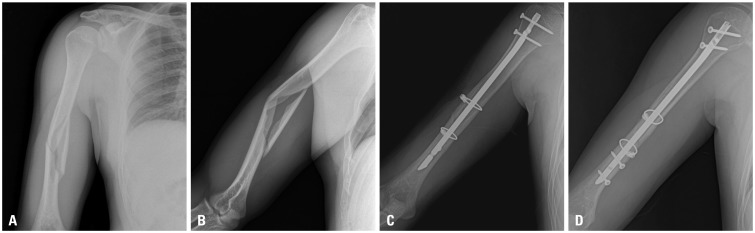
This study was conducted at a university-based, level 1 trauma center. All operations were performed by a single senior surgeon with more than 15 years of experience in orthopedic surgery. Reduction was attempted under general anesthesia using manual traction. If this was easily performed, the conventional closed nailing technique followed by postoperative rehabilitation, as described in Chapman, et al.,12 was used. However, if closed reduction failed or the reduced humerus was too unstable to maintain the reduced status, open reduction was selected instead. This usually happened in OTA/AO A1, B1, or C type fractures. The location and length of incision required for reduction of the fracture was confirmed using an image intensifier. A skin incision was created along the anterolateral aspect of the arm, and the length of the incision was within half the length of the fracture extent, approximately 4–5 cm long. The brachialis muscle was split longitudinally, while injury to the periosteum was kept to a minimum. Incarcerated soft tissue and hematoma were removed to clear the surgical field and create an anatomical reduction. To maintain the anatomical reduction by forceps or clamps, one cerclage cable (Cable-ready, Zimmer, Warsaw, IN, USA) was applied. The tip of the cable passer (Zimmer) was kept in contact with the cortex so as not to jam the radial nerve or muscles between the cable and the humerus. Cable passers with a varying radius simplified this procedure. Considering the anatomic position of the radial nerve, passing the tip of the passer from posterior to medial was preferred. The regulation tension of the cerclage cable, with a diameter of 1.8 mm, was set to 70 lb. If the reduced fragments were still unstable, an additional cable was added in the same manner. All cases were stabilized by an AO unreamed humeral nail (Synthes, Oberdorf, Switzerland) with an appropriate length and a diameter of 6.7 or 7.5 mm.
Radiographs, function [indexed by scores on the Disabilities of the Arm, Shoulder and Hand (DASH)13 and the University of California, Los Angeles (UCLA)14], and postoperative complications, such as non-union, delayed union, and radial nerve palsy or infection, were evaluated during every visit to the outpatient clinic at 1, 2, 3, 4, 6, and 12 months after surgery. The mean duration of the follow-up was 32.2 months in the cable group and 29.6 months in the non-cable group. Radiographic interpretation was conducted by a single orthopedic surgeon blinded to patient information. Bone union was determined as cortical continuity and obliteration of the fracture line. Non-union was defined as a fracture that showed absence of bone union for at least 6 months. This study was approved by the Ethics Committee at our university.
To compare the two groups, we used a Mann-Whitney U-test for continuous variables and Fisher's exact tests for categorical variables. Statistical significance was considered for p<0.05. SPSS software for Windows (ver. 12.0.1; SPSS, Inc., Chicago, IL, USA) was used for the statistical analysis.
RESULTS
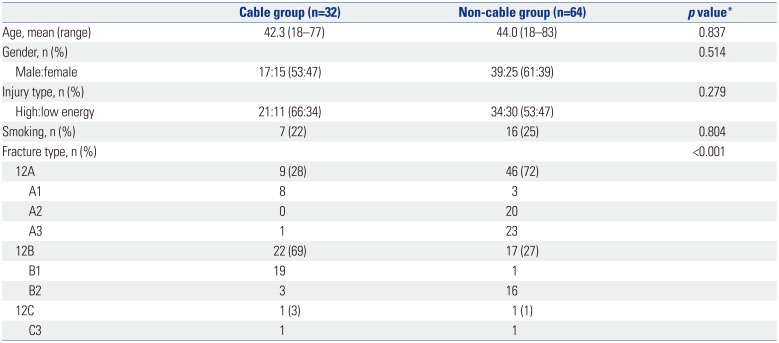
The patients' demographic data are provided in Table 1. No significant differences in terms of age, gender, injury type, or smoking history were found between the groups, except for the type of fracture. The cable group had significantly more complex fracture types than the non-cable group: 69% of the cases in the cable group were classed as type 12B, while 72% of cases in the non-cable group were classed as type 12A (p<0.001).
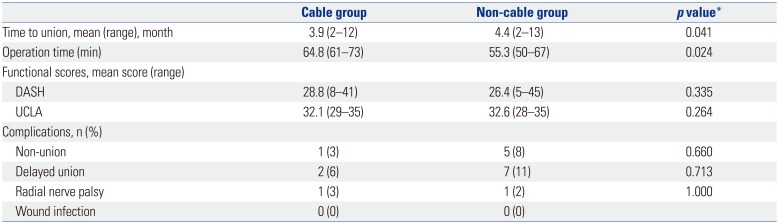
The length of time to bone union was shorter in the cable group (mean, 3.9 months) than the non-cable group (mean, 4.4 months); this difference was found to be statistically significant (p=0.041) (Fig. 1). At the final follow-up, the mean DASH scores for disabilities were 28.8 in the cable group and 26.4 in the non-cable group (p=0.335). The UCLA scores for shoulder function in the two groups were 32.1 and 32.6, respectively (p=0.264).
In terms of postoperative complications, non-union was identified in one case in the cable group and in five cases in the non-cable group (p=0.660). Three of the cases from the non-cable group underwent re-operation by augmented fixation with a locking compression plate (LCP), while the remainder underwent an auto iliac bone graft and augmented LCP. The incidence of radial nerve palsy was found to be comparable between the two groups. In both groups, each case of radial nerve injury had fully improved within 6 months after surgery (Table 2).
DISCUSSION
Cerclage cables have been regularly used in the lower extremities for periprosthetic fractures following arthroplasty and have provided satisfactory clinical results.815 However, few studies have investigated the use of cables in the upper extremities. A case of a periprosthetic fracture after shoulder arthroplasty was reported in which a plate/cable system for the humeral shaft was used.16 One study reported that, of 125 cases with a humeral shaft fracture, 20% of patients with an extended oblique or spiral type of fracture were fixed with cerclage wiring followed by IMN; however, no subgroup results were reported.2
We compared the clinical results of the open cerclage cable technique followed by nailing to the traditional closed nailing technique in humeral shaft fractures. As indicated by our results, the cable group, which had a greater number of patients with complex types of fracture, had a greater tendency for bone union to occur over a shorter time than the non-cable group. Other clinical results, such as functional score and the incidence of postoperative complications, such as non-union, delayed union, radial nerve palsy, and infection, were found to be similar between the two groups. Therefore, we deemed the open cerclage cable technique followed by nailing to be an effective and safe treatment for fractures of the humeral shaft.
The time taken for bone union to occur in a humeral shaft fracture is reported to be approximately 4 months and the rate of non-union is 4–13%.41718 Although open reduction and internal fixation with cerclage cables followed by IMN could have advantages over the conventional closed nailing technique, such as easier and more anatomic reduction and stability, there remains the concern of whether the technique can delay the time required for bone union to take place or increase the rate of non-union by decreasing the periosteal blood circulation. There have been several reports in the literature that have supported the concept that the humeral shaft has sufficiently strong circulation to allow healing of the fracture while remaining resistant to surgical dissection around the fracture site. In a randomized study, both the conventional open plating technique and minimal invasive plate osteosynthesis (MIPO) showed no significant difference in the time taken for bone union to occur in humeral shaft fractures (15.8 and 14.6 weeks, respectively).19 Additionally, another randomized study reported that the closed IMN and dynamic compression plating techniques result in comparable bone union in such fractures.17 A cadaver study concluded that a small number of cerclage cables had a minimal effect on the periosteal blood supplying the femur as long as they were not vigorously applied.20 Therefore, our hypothesis was that additional fixation with one or two cerclage cables after open reduction for complex types of fracture might be reasonable, even though it may also affect periosteal circulation in the humerus. In the current study, the mean length of time to bone union in the cable group was 3.9 months, which was shorter than that in the non-cable group, even though the cable group included much more complex types of fractures. Therefore, the open cerclage cable technique may not affect the rate of bone union adversely.
Radial nerve palsy probably occurs as a result of excessive traction or manipulation and interposition of the nerve at the fracture site.21 Most occurrences of radial nerve palsy following treatment for humeral shaft fracture are transient and do not require further intervention, as long as the nerve is not interposed at the fracture site.22 If radial nerve palsy does develop in a case of distal humeral fracture following conventional closed IMN, it could be difficult to determine its cause (i.e., neuropraxia from excessive manipulation or interposition of the nerve at the bone fragments). Therefore, open reduction during IMN in the distal humeral fracture can provide other advantages, such as the intraoperative inspection of the interposition of the nerve at the fragments. Jamming of the radial nerve between the cable and humeral cortex can be prevented if the cable passer is in touch with the cortex, as mentioned in the surgical technique.
In patients who have undergone open reduction and additional fixation with cerclage cables, the muscles in the arm, particularly the brachialis, may experience increased injury, compared with the closed nailing technique. However, DASH scores, reflecting the level of disability in the arm, were similar between the two groups. Other studies have reported excellent functional scores after the union of humeral shaft fractures with treatment techniques, such as conventional plating or MIPO, which suggests that the muscles in the humerus recover well without any functional deficits.
Open reduction and fixation with cerclage cables prior to IMN may lead to even more advantages. The radiation exposure time during the operation can be decreased compared to the conventional nailing technique. Although the exposure time has not been investigated in the present study, the open reduction method can decrease the level of radiation exposure, compared to closed reduction.19
Our study had some limitations. First, it was a comparative study, but not of a randomized design. The open cerclage cable technique can be used only for cases where closed reduction is difficult or where the fracture is highly unstable even after closed reduction has taken place, which may complicate a randomized comparative study. Second, the cable and non-cable groups included different types of fractures. However, this was inevitable because the more complex the fracture, the greater the need for additional fixation with cerclage cables via open reduction. Markedly comminuted fracture with multiple small fragments may not be a good indication for the open nailing technique as it is difficult to stabilize the fracture site using cerclage cables. In the future, if there were a larger number of patients, it would be possible to analyze them according to fracture subtype, such as 12A, 12B, and 12C, etc. Third, the open cable technique should be performed carefully not to hurt the radial nerve.
In conclusion, we have shown that additional fixation with one or two cerclage cables following open reduction may not delay the time taken for bone union to occur or increase the rate of postoperative complications, such as radial nerve palsy, compared with the conventional closed nailing technique. Therefore, in humeral fractures that are highly unstable or would be difficult to reduce in a closed manner, open reduction and internal fixation with one or two cerclage cables followed by IMN may be a safe and effective option.
 XML Download
XML Download