

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A missed Monteggia fracture refers to an unreduced dislocation of the radial head that is still present 4 weeks after injury, which may lead to elbow pain, decreased elbow motion, increasing valgus deformity, and neurologic problems.1234 Surgical treatment is usually recommended for patients with pain or limited functionality with loss of elbow motion, in whom the concave morphology of the radial head is preserved.5 For this, there are various surgical treatment options, including open reduction of the radial head and ulnar osteotomy with or without annular ligament reconstruction (ALR),26789101112131415 closed reduction by ulnar correction using single-stage osteotomy,16171819 or gradual distraction lengthening using an external fixator.202122 Although many studies have reported various techniques, there is no established standard treatment protocol for missed Monteggia fracture.
Although many surgeons agree that ulnar length and alignment must be restored to reduce the radial head congruently, opinions differ regarding the need for open reduction of the radial head. Some surgeons have performed open reduction of the radial head as a first procedure before ulnar osteotomy or ALR to remove posttraumatic fibrosis and annular ligament remnants,7810152324 while others insist that indirect reduction of the radial head by ulnar osteotomy could achieve good results without open reduction.171819202122 Moreover, several papers have reported satisfactory results with open reduction alone in some patients with missed Monteggia fracture.1462526 Although these reports could not suggest the indications for open reduction alone for missed Monteggia fracture, open reduction alone might be the ideal procedure in select patients.
At our institution, surgical reconstruction has always begun with open reduction of the radial head. On the basis of our clinical observations, we hypothesized that open reduction could be performed as a solitary procedure without ulnar osteotomy or ALR in some cases of missed Monteggia fracture. Therefore, the purposes of this study were to review our cases of missed Monteggia fracture treated by open reduction of the radial head with or without ulnar osteotomy and to investigate the indication for open reduction alone in surgical treatment of missed Monteggia fracture.
MATERIALS AND METHODS
This study was perfomed at Severance Children's Hospital. This retrospective study was approved by the Institutional Review Board at our institution. We identified 22 patients who were treated with open reduction of the radial head with or without combined ulnar osteotomy between July 2003 and November 2015 for missed Monteggia fracture. Patients who presented at least 1 month after injury were included in the study. Patients with congenital dislocation or neuromuscular diseases were excluded.
The mean age of the patients at operation was 7.6 years (range, 3.5–14.3 years), and there were 11 boys and 11 girls. The right elbow was injured in 13 patients, and the left was injured in 9. All cases were classified as Bado27 type I. All patients had a history of trauma involving the ipsilateral elbow or forearm and were referred from other hospitals. They complained of limited elbow and forearm motion, and none of patients had signs of neuropathy or a history of previous elbow surgery. The mean interval from injury to surgery was 16.1 months (range, 1 month–7 years). The mean period of follow-up was 3.8 years (range, 1–14 years).
All patients were checked for elbow pain, range of elbow movement, carrying angle, and any disabilities in daily life by two independent orthopedic residents who were blinded to the study. Preoperative and postoperative Mayo Elbow Performance Index (MEPI) scores were ascertained for all patients.28 We also compared the preoperative and postoperative Kim's elbow functional scores.29 The Kim's index is based on four parameters: deformity, pain, range of motion, and function. These four parameters are weighted equally, giving 25 points to each parameter, for a total score of 100 points.29
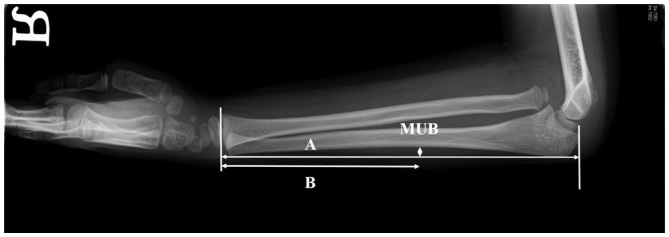
All radiologic measurements were performed by two orthopedic clinical fellows who were blinded to the study. Deformity of the radial head, osteoarthritic changes, and congruency of the radiocapitellar joint were evaluated with routine preoperative and postoperative serial radiographs. We measured the maximum ulnar bow (MUB) and location of the bow on true lateral forearm radiographs, because humeral tilting on forearm radiography affected the assessment of ulnar bowing (Fig. 1).30 MUB was defined as the maximum perpendicular distance from a straight line drawn along the dorsal ulnar border.31 The location of the bow was defined as the location of the MUB and calculated as a ratio of the percentage of the length of the ulna from the distal end.31 The final reduction status of the radial head was divided into three categories: good (complete reduction without osteolytic change), fair (reduction with subluxation or osteolytic change), or poor (radial head dislocation).12
Surgical technique
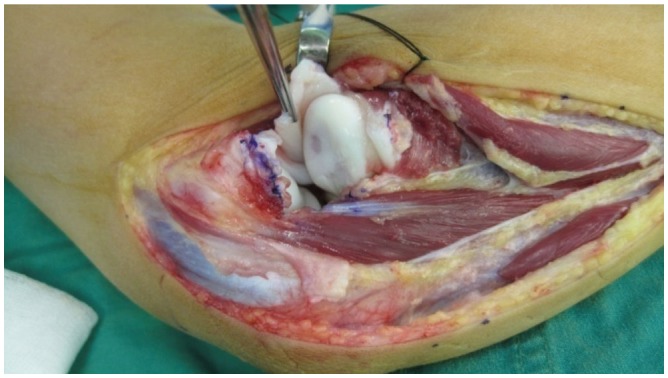
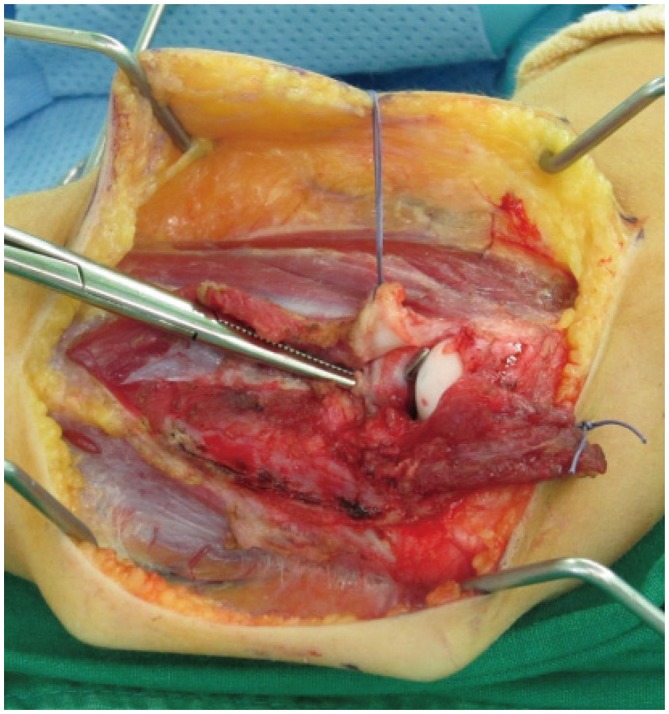
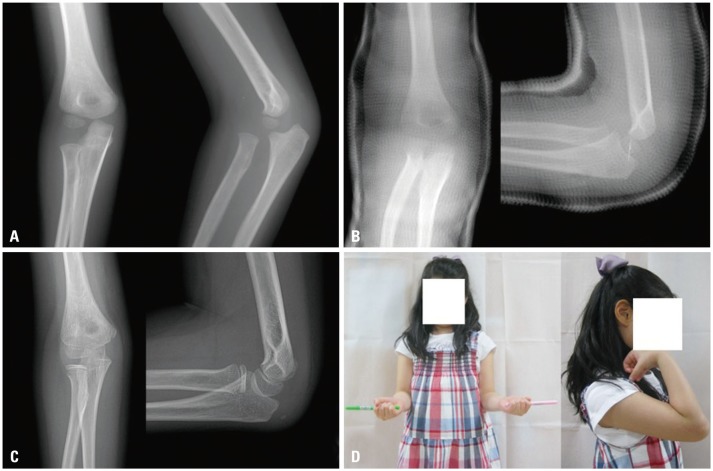
All operations were performed by one of the authors. First, we tried closed reduction under general anesthesia. However, we failed to achieve proper reduction in all patients, so surgical treatment was performed. We performed open reduction through a Kocher approach. The radiohumeral joint was opened, the radial head was exposed, and we assessed the state of the cartilage of the radial head. In all cases, the radial head was surrounded with dense fibrous scar tissue, which was excised, as it was preventing the radial head from reducing to a stable position (Fig. 2). However, we observed that the annular ligament was displaced into the joint but remained intact in some cases (Fig. 3). Then, reduction of the radial head was attempted and its stability was assessed. The correct position of the radial head was evaluated in flexion, extension, pronation, and supination under direct visualization. Especially, it is important to check the stability of the radiocapitellar joint with the elbow in full pronation and flexion beyond 90 degrees. We also confirmed the position of radial head in both the anteroposterior and lateral projections under an image intensifier. When the annular ligament was identified and repairable, we only tried to repair the remnants of the ligament. ALR was not performed in any cases. If reduction of the radial head was achieved easily and it was confirmed to be sufficiently stable, then no additional procedure was performed. We achieved stable reduction with open reduction alone in some patients (Fig. 4). However, in cases where reduction of the radial head was not possible with open reduction alone, corrective ulnar osteotomy was performed (Fig. 5). The osteotomy site was the area of maximum deformity or at the proximal third of ulna if there was no apparent deformity.1214 After osteotomy, the osteotomy site was angulated to correct the deformity, and the radial head was easily reduced by manipulation. The angulated shaft of the ulna was rigidly fixed with a plate bent to the desired angle. Additional bone grafting was not performed in all patients. Postoperatively, an above elbow cast was applied to all the other patients with the elbow in 90° of flexion, and the forearm was maintained in a neutral position for 6 weeks after surgery. After removal of the cast, we encouraged gentle active movement of the elbow.
Statistical analysis
Bland and Altman plots and repeatability coefficients were used as measures of the interobserver and intraobserver repeatability for all evaluations. The 95% limits of agreement represent a visual judgment of how well the measurements of the two reviewers agreed. By definition, the measurement error was smaller than the repeatability coefficient for 95% of the observations. To compare preoperative variables between patients according to surgical technique, Mann-Whitney U test was used for nonparametric data. Student's paired t test was used for parametric data, and the Wilcoxon signed-rank test was used for nonparametric data to compare clinical and functional outcomes. In all analyses, a p-value less than 0.05 was considered statistically significant.
RESULTS
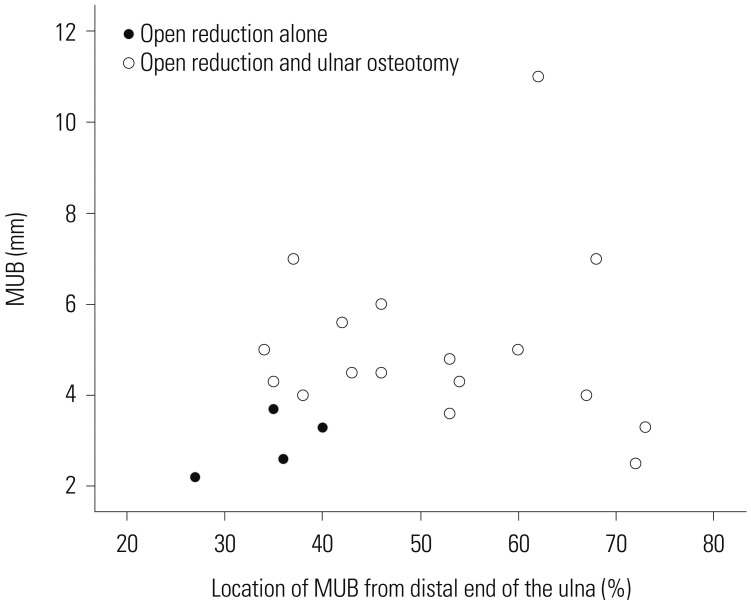
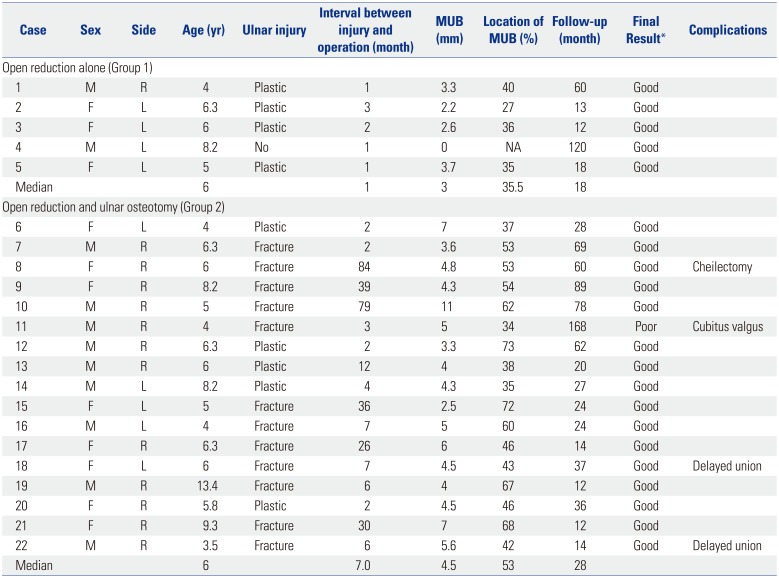
Five patients (Group 1) underwent open reduction without ulnar osteotomy, and the other 17 patients (Group 2) underwent additional ulnar osteotomy fixed with a plate. At the latest follow-up, the radial head was maintained in a completely reduced positioned in 21 (95%) patients. The overall preoperative variables, postoperative radiographic and final results, and complications are summarized in Table 1. In the five patients who underwent open reduction alone, the median MUB was 3 mm and the median location of the MUB was 35.5%. Additionally, there were no previous displaced ulnar fractures in this group. There was statistically significant differences with regard to the interval between injury and operation (p=0.004), MUB (p=0.011), and the location of MUB (p=0.018). In Group 1, the interval between injury and operation was shorter, the MUB was smaller, and the location of MUB was more distal area of ulna than in Group 2. The relationships between the method of surgical treatment, MUB, and the location of MUB are shown in Fig. 6. When the MUB was less than 4 mm and the MUB was in the distal 40% of the ulna, we were able to achieve reduction of the radial head without ulnar osteotomy.
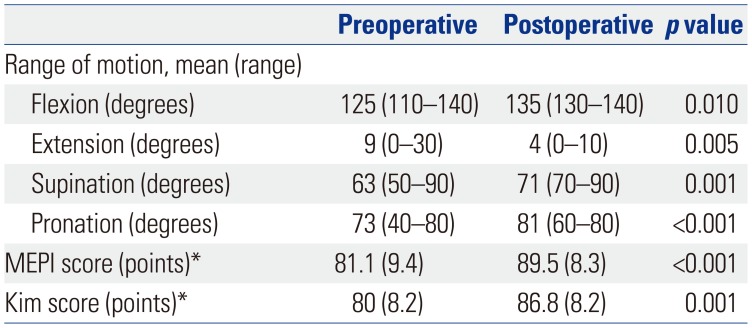
We found a significant improvement between preoperative and postoperative elbow ranges of motion in all patients. The mean preoperative MEPI and Kim's scores improved significantly at final follow-up (Table 2).
There were four postoperative complications. In one patient (case 11), the radial head re-dislocated anteriorly from the center of the capitellum, and the patient's symptoms did not improve, but he refused further surgery. He complained of a cubitus valgus deformity 7 years after the surgery, and a correctional osteotomy was done. Two patients (cases 18 and 22) had a delayed union at the ulnar osteotomy site and were managed with refreshment of the nonunion site, application of an iliac crest bone graft, and repeat plate fixation. One patient (case 8) had a complaint regarding cosmetics and posterior ulnar angulation due to the ulnar osteotomy. We performed cheilectomy for a bony spur of the ulna. Other complications, such as compartment syndrome, infection, and neuropathy, did not occur in any patients.
All measurements showed excellent intraobserver and interobserver reliability, with correlation coefficients ranging from 0.71 to 0.85.
DISCUSSION
Many studies have reported on the treatment of missed Monteggia fracture; however, there is no general consensus regarding the best method of treatment. Previous studies mainly have focused on only one procedure or issue, such as reduction methods (open vs. closed), the location and technique for ulnar osteotomy, or the necessity of ALR. We highlighted the sequence of surgical treatment for missed Monteggia fracture. Our surgical procedure is based on the hypothesis that open reduction plays the most important role among surgical procedures for missed Monteggia fracture. In this study, we performed open reduction of the radial head as a first step. If stable reduction of the radial head was not achieved, ulnar osteotomy was done as an additional procedure. In five patients, reduction of the radial head was maintained with open reduction only. We were able to achieve stable reduction of the radial head in these patients until final follow-up.
Open reduction alone is not sufficient to obtain and maintain reduction of the radial head in all patients with missed Monteggia fracture and has been used in only a few studies.1462526 These authors operated on select patients with missed Monteggia fracture using open reduction only, reporting good results. Among them, one report recommended that open reduction with repositioning or repair of the annular ligament might be a favorable option.26 In our study, we achieved stable reduction of the radial head with open reduction alone in five patients. Therefore, we think that open reduction alone may be effective in select patients.
Our results suggest that patients with a smaller MUB and an MUB closer to the distal end of the ulna are less likely to require ulnar osteotomy. There were no previous displaced ulnar fractures in the five patients who underwent open reduction alone. Although ulnar bowing was not investigated in previous studies, one author insisted that neither ALR nor osteotomy of the ulna were necessary in the treatment of missed Monteggia fractures without bowing of the ulna.25 The authors of the current study do fully agree with this opinion. Although we could not suggest definite indications of open reduction alone for missed Monteggia fracture, open reduction alone may be effective for select patients with minimal bowing of the distal ulna.
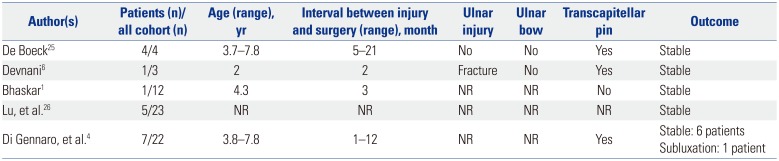
In our sturdy, the median interval from injury to surgery in patients who underwent open reduction only was 1 month. Although these intervals were significantly shorter, compared with those in patients who underwent ulnar osteotomy, we could not reduce the radial head without ulnar osteotomy in patients who had short interval from injury to surgery and definite ulnar bowing (Table 1) (case 6, 7, 12, 20). We noted intraoperatively that in patients with definite ulnar deformity, it was more difficult to achieve a stable reduction with open reduction alone. We reviewed previous studies reporting the results of open reduction alone in missed Monteggia fracture (Table 3). While the interval from injury to surgery varied, some surgeons performed open reduction alone in patients with long interval from injury to surgery.425 Considering results of our study and previous reports, the interval from injury to surgery may not be a factor to decide on a surgical procedure.
There were several reports about successful reduction of the radial head by ulnar osteotomy without open reduction in missed Monteggia fracture.1719202122 However, most reports recommended open reduction if satisfactory closed reduction was not achieved.192021 We think that it may be difficult to reduce the radial head with ulnar osteotomy alone without open reduction, because a dislocated or torn annular ligament could form meniscoid scar tissue. The advantage of open reduction as a first step is that we can observe the status of the radiocapitellar joint and excise underlying pathologic lesions, such as dense fibrous tissue, cartilaginous or meniscoid scar tissue, and a pseudocapsule. Another advantage is that we can achieve stable reduction with open reduction alone without ulnar osteotomy in some patients.
Ulnar osteotomy has been recommended as a key procedure in the treatment of missed Monteggia fracture and is based on the hypothesis that the primary problem is malunion of the ulna preventing reduction of the radial head.7919 Open reduction of radiocapitellar joint as a first surgical approach may be an inappropriate solution for missed Monteggia fracture. However, in some previous studies, ulnar osteotomy for the treatment of missed Monteggia fracture has been performed at proximal area not original fracture site of the ulnar, which helped maintain the integrity of the interosseous membrane.123233 Although ulnar osteotomy is not a difficult procedure, there are several complications related to ulnar osteotomy, including delayed union, nonunion, fixation failure, and negative cosmetic problems.9143435 Therefore, we think that open reduction of radiocapitellar joint may be considered as first step if the ulnar length and alignment is not deformed severely.
Regarding ALR, various methods have been proposed.131536 Several authors insist that ALR is crucial for stability of the radial head and are concerned about the lack of stability of the radial head without reconstruction of the annular ligament.15373839 However, others found that ALR was not mandatory.6891019 Moreover, other complications, including osteolytic changes, narrowing of the radial neck, growth disturbance, heterotopic ossification, and osteonecrosis of the radial head, have been reported after ALR.2935404142 Although the annular ligament contributes to the stability of the radial head to a certain extent, stability of the elbow joint is maintained by the bony structure and joint congruity.34 In our series, the radial heads were stable and the functional outcomes were satisfactory without ALR. In most cases, the annular ligament was ruptured or dislocated over the radial head, forming meniscoid scar tissue and thereby preventing reduction. We simply repaired or resected the annular ligament in all patients. Therefore, we thought that ALR was not necessary according to our experience.
To summarize the surgical strategies, the first step is to perform X-ray of the forearm in order to measure the ulna contour. True lateral forearm radiograph in which the posterior supracondylar ridges are superimposed should be obtained.30 This method allows for visualization of true bowing present in the ulna. If there is minimal bowing, especially if the MUB was less than 4 mm and the MUB was in the distal 40% of the ulna, we suggest that an open reduction must be perform as a first surgical approach. Then if stability of the radial head is achieved by open reduction only, then an additional procedure for the ulna is not necessary. However, if the definite ulnar bowing is seen on initial X-ray, open reduction with additional ulnar osteotomy should be considered, because residual deformity of the ulna interrupts repositioning of the radial head by open reduction alone. By following our treatment plan, unnecessary ulnar osteotomy can be avoided in some cases.
There were several limitations to our study. First, it was a retrospective review without randomization, and our sample size was small because of the infrequent incidence of missed Monteggia fracture. Accordingly, it is difficult to draw generalizable conclusions from our study. However, our number of cases (22 cases) was similar to the size of the cohort of most previous studies. Second, although we performed subgroup analysis according to surgical technique, sample size was too small to compare the preoperative variables between groups. These may have decreased the power for statistical analysis. Third, although MEPI has presently been validated only in adults, there is no elbow score for children, and therefore, we used MEPI, as have previous studies. To compensate for this limitation, we used an additional functional outcome measure proposed by Kim, et al.29
Our data suggest that open reduction alone can lead to stable relocation of the radial head only in select patients with minimal bowing of the distal ulna. We recommend open reduction as a first surgical procedure to prevent unnecessary ulnar osteotomy. However, ulnar osteotomy should be considered in patients with definite ulnar deformity.

 XML Download
XML Download