

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Statin treatment has persistently demonstrated a significant benefit in diminishing cardiovascular disease (CVD) risk, especially in primary prevention settings.12 Recently, the American College of Cardiology (ACC) and American Heart Association (AHA) reported extensively on cholesterol management guidelines, focusing on the use of statin therapy for prevention of CVD, based on a new pooled cohort risk equation designed to predict 10-year risk of atherosclerotic cardiovascular disease (ASCVD).3 Although these updated guidelines increased the eligibility of patients for statin treatment, they also led to an overestimation of CVD risk in several particularistic populations.456
Coronary artery calcium (CAC) score is determined using cardiac computed tomography and acts a robust marker of coronary artery calcification. Prior studies have reported that CAC score is closely associated with increased coronary atherosclerotic burden, as well as future onset of adverse cardiac events.78910 Current guidelines for assessing CVD recommend that CAC screening should be considered for primary risk assessment in asymptomatic populations.11 Furthermore, more recent studies have documented that reclassification of populations according to CAC score may facilitate treatment decision-making in clinical settings.121314
Cardiovascular disease burden tends to differ according to ethnicity. Indeed, Asians often present with a low risk for CVD.1516 Accordingly, assessing the efficacy of statin treatment according to the recently updated 2013 ACC/AHA guidelines in these individuals is warranted. Using a large multicenter registry of asymptomatic Korean adults, we sought to explore whether CAC scoring could reclassify individuals recommended for statin treatment according to the recently updated 2013 ACC/AHA cholesterol management guidelines.
MATERIALS AND METHODS
Study design and population
This study population belonged to the KOrea Initiative on Coronary Artery calcification (KOICA) registry. The KOICA registry is a single ethnicity, multicenter, observational registry of self-referred individuals who underwent a health check-up at one of three healthcare centers in South Korea (i.e., Severance Check-up Healthcare Center; Seoul National University Healthcare System, Gangnam Center; and Samsung Medical Center in Seoul, South Korea). A total of 48903 individuals were recruited between December 2002 and July 2014. For the purposes of this study, subjects were deemed eligible for study inclusion if they were of an age between 40 to 75 years and had no known CVD at baseline. Otherwise, individuals were excluded from the study if they were prescribed any lipid-lowering medication or were missing any values related to risk factors used for calculating 10-year ASCVD risk or CAC score. Hence, after applying the inclusion and exclusion criteria, 31375 individuals were subsequently enrolled in the current analysis (Fig. 1). The appropriate institutional review board committees at all centers approved the study protocol.
Acquisition of clinical factors
Baseline demographic and risk factors were collected at the time of each initial visit to the healthcare centers. Age, gender, body mass index, and systolic and diastolic blood pressure were measured as baseline demographic profiles. A self-reported medical questionnaire was used to obtain information on past medical history. Presence of hypertension was defined as a history of being diagnosed with hypertension or taking antihypertensive medications. Presence of diabetes mellitus was defined as a history of being diagnosed with diabetes or receiving medication for diabetes. Current smoking was defined as active smoking status. Total, high-density lipoprotein, and low-density lipoprotein (LDL) cholesterol were obtained after participants had fasted for a minimum 8 h. CACS was measured using a >16-slice CT scanner. Specific CT scanner types used within each center included the Philips Brilliance 256 iCT, Philips Brilliance 40 channel multi-detector CT (Philips Healthcare, Cleveland, OH, USA), Siemens 16-slice Sensation (Siemens AG, Forchheim, Germany), and GE 64-slice Lightspeed (GE Healthcare, Milwaukee, WI, USA). A calcium scan was performed using standard prospective or retrospective methods with a 225 to 400 ms gantry rotation time. Image data were reconstructed with a 2.5- to 3-mm slice thickness. Calcium score analysis was performed using dedicated workstations (AW Volume Share 5 workstation, GE Healthcare; Rapidia 3D, Infinitt Co., Seoul, Korea; EBW workspace version 3.5, Philips Healthcare) and analysis software (Smart Score 4.0, GE Healthcare; Rapidia3D, Infinitt Co.; HeartBeat CS, Philips Healthcare). Estimated radiation doses for CACS ranged between 0.7–1.5 mSv. CAC score was calculated based on the Agatston scoring method,17 and subjects were categorized according to the presence any of CAC (CAC>0), as well as CAC 0, 1–100, and >100 based on the background of CAC.1819
Statin candidate groups
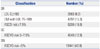
In this study population, we calculated 10-year ASCVD risk, based on that for Caucasians, and subsequently categorized participants according to 2013 ACC/AHA cholesterol management guidelines using the following groups: statin recommended (SR), statin considered (SC), and statin not recommended (SN) (Table 1).3 Specifically, the SR group was defined as either: 1) those with LDL cholesterol levels ≥190 mg/dL, 2) those aged 40 to 75 years with diabetes and LDL cholesterol levels ranging from 70 to 189 mg/dL, or 3) individuals without diabetes, but with an estimated 10-year ASCVD risk of 7.5% or higher. The SC and SN groups were defined as individuals without diabetes or ASCVD events and with a 10-year ASCVD risk of between 5% to 7.5%, and <5%, respectively.
Study outcome
The primary outcome of the KOICA registry is all-cause mortality (ACM). Ascertainment of ACM events was determined by querying the Ministry of Security and Public Administration up until December 2014 for two centers and until September 2014 in the remaining center.
Statistical methods
Continuous variables are reported as means with standard deviations, and categorical variables are reported as counts with proportions. A one-way analysis of variance (ANOVA) was used for the comparison of continuous variables across statin groups, and Pearson’s Chi-squared test was employed for comparison of categorical variables between statin groups. Cumulative mortality events over time according to CAC categories and statin candidate groups were calculated by use of the Kaplan-Meier method and compared using the log rank test. Time to mortality event was assessed using incidence rates per 1000 person years. Further, Cox regression analysis was used to estimate the risk of ACM according to CAC categories across statin candidate groups, reporting adjusted hazard ratios (HR) with 95 % confidence intervals [95% confidential interval (CI)]. Models were adjusted for age, gender, BMI, hypertension, and current smoking. We calculated number needed to treat (NNT) to prevent one mortality event by applying the mortality risk associated with statin treatment in primary prevention on the basis of a Cochrane meta analysis.20 The results from 18 randomized control trials showed that the incidence of ACM is lowered by 14% according to statin treatment (odds ratio: 0.86, 95% CI: 0.79 to 0.94). The 5-year NNT was calculated as the reciprocal of the absolute risk difference at 5-year follow up based on Kaplan-Meier estimates, according to the Altman and Andersen21 method, in each CAC category across statin candidate groups. A two-tailed p value <0.05 was considered statistically significant. All statistical analyses were performed using STATA Version 13 (StataCorp LP, College Station, TX, USA).
RESULTS
Baseline characteristics
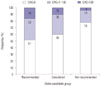
Mean age of the study participants was 54.4±7.5 years, and 23923 (76.3) were male. Baseline characteristics according to the statin candidate groups are shown in Table 2. Demographic variables and lipid profiles differed among the three statin candidate groups. CAC distribution according to statin eligibility is displayed in Fig. 2. The proportion of zero CAC was more than 50% across all statin candidate groups, while the proportion of a CAC score >100 tended to increase within the SR group (16%), as compared with the SC (10%) and SN groups (4%), respectively.
All-cause mortality and CAC across statin candidate groups
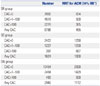
During a median follow-up of 5 years (25–75th percentile: 3–7 years), 251 mortality events occurred among 31375 subjects. Fig. 3 shows the incidence of mortality per 1000 person-years for each CAC category by statin candidate group. Notably, mortality events tended to be higher among subjects with a CAC score >100, compared with the other CAC groups. In Cox regression analysis, a CAC score >100 was independently associated with ACM in all three statin candidate groups, even after adjusting for numerous cardiac risk factors (Table 3). In particular, in the SN group, the adjusted risk of death for those with a CAC score >100 increased by more than three-fold (HR, 3.14; 95% CI, 1.08–9.17; p value, 0.036), compared with those in the SN group with a CAC=0.
Number needed to treatment
In Fig. 4, Kaplan-Meier survival curves revealed that increasing CAC score categories were associated with a concurrent rise in mortality across each of the statin candidate groups (Log rank p values were <0.01 in overall, SR, and SC groups, and p value= 0.07 in SN group). Based on Kaplan-Meier estimates, the 5-year NNTs to prevent one ACM event was 834, 1250, and 2000 for CAC score 0; 500, 1250, and 1429 for CAC scores 1–100; and 385, 667, and 500 for CAC scores more than 100 in the SR, SC, and SN groups, respectively (Table 4). Foremost, subjects with a CAC score >100 demonstrated the lowest NNT across all statin candidate groups.
DISCUSSION
In this multicenter observational study, we assessed the impact of CAC for reclassifying statin candidates according to the 2013 ACC/AHA cholesterol management guidelines for primary prevention. The results of the present study showed that CAC is closely related to a greater risk of ACM. Specifically, a CAC score >100 independently increased the risk of ACM across all statin candidate groups, while the NNT for preventing one mortality event during the current study period was lower among subjects with a CAC score >100 in the SC and SN groups. The 2013 ACC/AHA guidelines for the assessment of cardiovascular risk recommend that CAC screening should be considered only among cases in which treatment decisions remain uncertain following quantitative risk assessment.11 Nevertheless, the results of the current investigation indicated that CAC screening may be of use in guiding initiation of statin treatment in asymptomatic individuals.
In 2014, the ACC/AHA reported new cholesterol management guidelines that were based on 10-year ASCVD risk.3 In comparison with previous scores, such as the Third Report of the National Cholesterol Education Program (NCEP ATP-III) guidelines,22 in this study, the statin-eligible population was significantly increased when applying the new guidelines. Further still, Pencina, et al.6 reported that the more recent guidelines would increase the number of candidates for statin treatment by 11.1% or 12.8 million, especially in primary prevention settings, using data from the United States National Health Survey. Although the use of statins could have a large public health benefit,23 statins cannot be recommended purely on the basis of high risk, given concerns for efficacy, potential side effects, and health-related costs.2425 Therefore, the implication of the new cholesterol management guidelines should be carefully assessed.
In prior research, statin therapy exhibited different effects between Western and Asian populations. For example, the initiation of statin therapy in Asian populations usually begins with a lower dose, compared to Western populations, as the pharmacokinetics and metabolites of statins differ substantially by ethnicity.26 Moreover, the Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese (MEGA) study reported that the low dosage statin prescribed therein was half the dose often utilized in European and U.S. populations and could significantly lower the risk of coronary heart disease in Japanese patients.27 A recent meta-analysis evaluating the effect of statin therapy on coronary plaque also documented a different effect of statins for modifying LDL-cholesterol levels, as well as the regression of coronary atherosclerotic plaque, among ethnic groups.28
In this study, we employed CAC as a marker for reclassification of statin treatment. It is well known that CAC score has added benefit towards cardiovascular risk prediction over conventional risk tools.2930 An additional strength is that CAC can be employed to better define target populations who require preventive treatment through prescribing cardiovascular medications. Indeed, Miedema, et al.13 investigated aspirin use for primary prevention of CHD in the Multi-Ethnic Study of Atherosclerosis (MESA). In that study, participants with a CAC score >100 showed favorable risk/benefit estimation on the background of aspirin use. Similarly, Blaha, et al.12 showed that CAC might have benefit for defining rosuvastatin eligible participants according to the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) trial.31 The results of the latter study demonstrated that the absence of CAC was related to an extremely lower CVD event rate in statin eligible participants.
Recently, Nasir, et al.18 reported the implications of CAC testing among statin candidates according to 2013 ACC/AHA cholesterol management guidelines in the MESA population. In that study, ASCVD risk appeared to be heterogeneous among statin candidate groups, while CAC appeared to reclassify this population. To this end, the absence of CAC reclassified half of the candidates as not suitable for statin treatment. Our data supports those results in that CAC scoring also appeared to be effective in determining a target population among Asians who might benefit from statin therapy. Nevertheless, some disparity exists between these studies: Our study showed that a CAC >100 is closely associated with mortality events and can perhaps identify participants who may be eligible for statin treatment. However, the absence of CAC did not prove useful for predicting incident mortality or NNT when compared with the presence of CAC in our study population. It bears mentioning however, that the clinical outcomes differed between both studies, whereby ASCVD events included both ACM and non-fatal CVD events in the MESA population while in the present study, only ACM events were included. In addition, the burden of CVD is lower in Korean populations than Western populations (i.e., MESA participants) that consist mainly of Caucasians.1532 Thus, the onset of adverse clinical events may only occur on the background of a higher level of CAC in Korean populations, particularly when compared with previous study cohorts, such as MESA.
Although, in this study, CAC scanning displayed some added benefit for reclassifying patient eligibility to receive statin therapy, the latter purpose of CAC scanning and its subsequent benefits are somewhat offset in light of the anticipated rise in healthcare costs, as well as the burden of additional radiation exposure. Though, a recent investigation from MESA study showed that CAC screening is likely to incur cost savings, compared with guideline based risk assessment strategies.33 Moreover, the radiation dose administered for CAC screening is continuously decreasing, with an effective median radiation dose comparable to mammograms.34
Limitations
The KOICA registry was designed retrospectively and observationally in nature. Thus, The KOICA population comprised only a self-referred population, and was predominantly male. Hence, our findings should be interpreted with caution when extrapolated to other populations. In light of the retrospective nature of this study and given treatment strategies for atherosclerotic disease have likely evolved since initial enrollment in 2002 through 2014, persons enrolled later into the study might have received different treatment strategies, compared to those enrolled earlier, which could have offset the risk of the study outcome. While we selected individuals who did not receive any lipid-lowering medications at baseline, we were unable to assess medication use that may have been initiated during the study follow-up period. Hence, another limitation of this study was not being able to ascertain the prevalence of statin therapy beyond CAC examination. While the new cholesterol management guidelines were based on a 10-year risk of ASCVD, information regarding ASCVD events was unavailable, as only ACM were ascertained in the KOICA registry. Therefore, further studies are needed to assess CAC and statin eligibility according to ASCVD events. Despite this, ACM is considered a useful clinical outcome as it lowers the potential for bias as opposed to utilizing a cause specific endpoint, particularly in a retrospectively designed study.35 Also, when estimating NNT, it is perhaps feasible to consider the likelihood for some uncertainty with regards to the application of reduction in risk of ACM on the background of Cochran’s meta-analysis. As such, our study’s NNT findings should be considered hypothesis generating only and interpreted with caution.
Conclusion
In a large sample of asymptomatic Koreans, CAC scoring further reclassified individuals for eligibility of statin treatment according to the recently updated 2013 ACC/AHA cholesterol management guidelines. Assessment of CAC scoring may prove useful for guiding treatment decision-making for initiating statins among Korean adults in a primary prevention setting.





 XML Download
XML Download