

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The probability of 5-year survival for cancer in children and adolescents now exceeds 80% due to dramatic advances in medicine.1 Despite great progress in developing cancer treatment, cancer remains the leading cause of disease-related death among children and adolescents.2 The diagnosis and treatment of cancer present numerous challenges and sources of stress for patients.3 Children and adolescents diagnosed with cancer experience emotional distress, such as sadness, worrying, and irritability among other negative emotions.4 Emotional distress in cancer patients is defined as an unpleasant experience of a psychological, social, and spiritual nature that may interfere with coping with cancer, its symptoms and treatments.5 The prevalence of emotional distress is high in patients diagnosed with cancer in general.6 Despite general agreement that cancer and its treatment can be stressful for patients, few studies have directly addressed the specific factors that affect children and adolescents diagnosed with cancer during early treatment. For children newly diagnosed with cancer, both the Child Behavior Checklist score and emotion-focused coping of their mothers predicted depression, anxiety, and global mental health.78
There is limited information on the psychological well-being of parents at the time of their child's diagnosis. Mothers of children newly diagnosed with cancer reported more depressive symptoms and emotion-focused coping than mothers of children with other acute illnesses such as gastrointestinal infections, fractures or lacerations.7 Previous studies have found that mothers experience substantial posttraumatic stress symptoms near the time of their child's or adolescent's cancer diagnosis and during the first 6 months of treatment.910 Neu, et al.11 reported that 27% of mothers experienced moderate to severe levels of depression and 46% of mothers experienced clinical anxiety during their child's cancer diagnosis. Elevated levels of maternal anxiety and depression may have an impact on an adolescent diagnosed with cancer since depression in mothers has been associated with higher levels of depression in children and adolescents.1213 A recent review of the psychosocial aspects of parents revealed that distress may impair vulnerable parents and may impact children's adjustment to cancer.14
The potential risk factors identified for maladjustment in cancer patients include cancer stage15 and recurrence status.16 In addition to disease factors, patients with premorbid psychiatric history1718 or low resilience are at risk for greater distress when coping with a high symptom burden. According to studies on patient-physician relationships, a physician's empathetic attitude can also have a positive influence on psychological adjustments in newly diagnosed cancer patients.1920 In children, individual variation in adjustment to cancer may be better understood in terms of differences in a child's temperament and coping style.21 Santos, et al.22 reported that family functioning is also a key issue for understanding adaptation in pediatric cancer.
However, less is known about the overall psychological effect of cancer on infants, children and adolescents. More information is needed on the specific factors that affect emotional distress of children and adolescents diagnosed with cancer, and how these stressors are associated with emotional adjustment to the disease and its treatment, particularly in children and adolescents.
The goal of this article was to investigate whether maternal and patient factors are associated with emotional distress of patients newly diagnosed with cancer. From a developmental perspective, we expected differences among infants, children, and adolescents.
MATERIALS AND METHODS
Study design and subjects
Research approval for a retrospective chart review was granted by the Institutional Review Board for research with human subjects at Yonsei University Severance Hospital. We retrospectively reviewed the medical records of patients newly diagnosed with cancer who were admitted to Yonsei Cancer Center and referred for psychiatric consultation between November 2014 and October 2016. Of 210 patients, 85 patients were included in the analysis. Inclusion criteria for patients were as follows: newly diagnosed with cancer including relapse after remission; diagnosed within the past 3 months; no pre-existing mental disorders; completed psychological inventories at the initial psychiatric evaluation; sufficient knowledge of the Korean language; presence of a mother as a caregiver; and age between 1 and 17 years.
Measures
Outcome variables
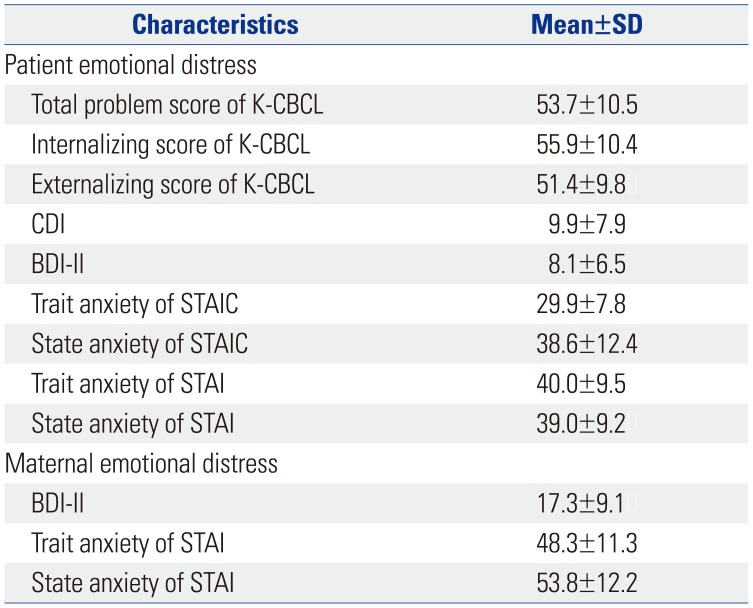
The following psychological inventory results were obtained from the patients and their mothers at the initial psychiatric evaluation. The Korean-Child Behavior Checklist (K-CBCL) was completed by mothers considering the behavior of their children in the previous 3 months. The inventory consists of 119 items which are summed into three global scores (total problem, internalizing, and externalizing scores). the inventories for the children between ages 7 and 12 years were: 1) Children's Depression Inventory (CDI) (Kovac, 1981) and 2) State-Trait Anxiety Inventory for Children (STATIC) (Spielberger, 1973). The inventories for the children between ages 13 and 17 years were: 1) Beck Depression Inventory-II (BDI-II) (Beck, et al., 1979) and 2) State-Trait Anxiety Inventory (STAI) (Spielberger, 1983). The STAIC and STAI consist of two subscales that measure state anxiety and trait anxiety.
Statistical analyses
All statistical analyses in this study were performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were presented as percentages. Pearson correlation analysis was used to analyze correlations between patient data including age, K-CBCL, CDI, BDI-II, STATIC, and STAI scores, and maternal data including BDI-II and STAI scores. To determine factors associated with patient emotional distress, multiple linear regression was used after performing correlation analyses. The stepwise method was used for the order of significance in the correlation analysis. Correlations between variables with p-values<0.05 were considered significant.
RESULTS
Demographic and clinical data
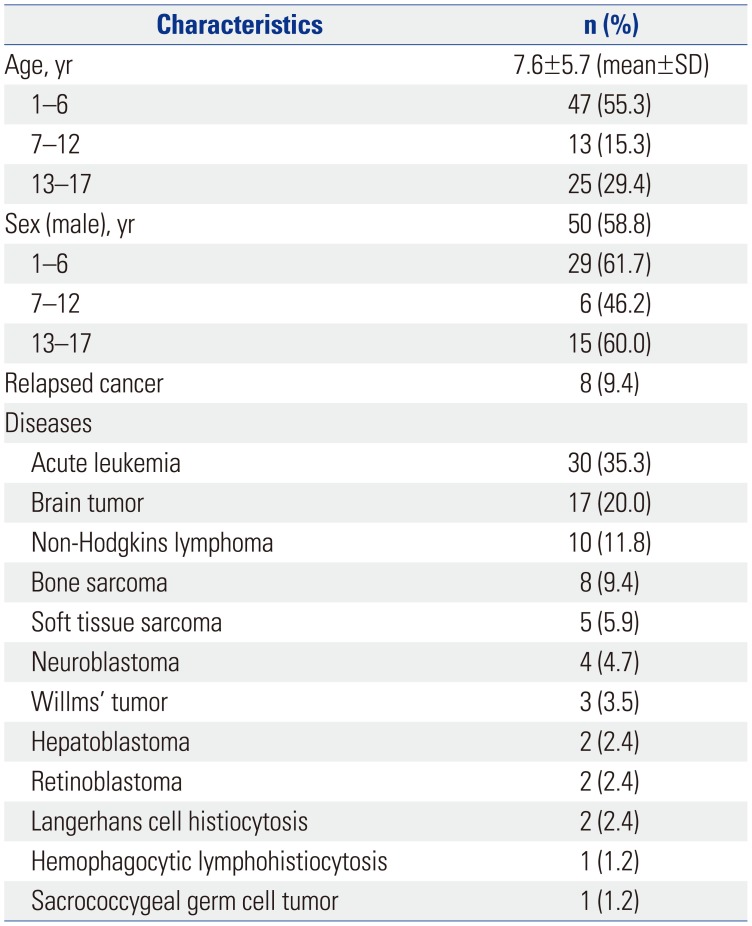
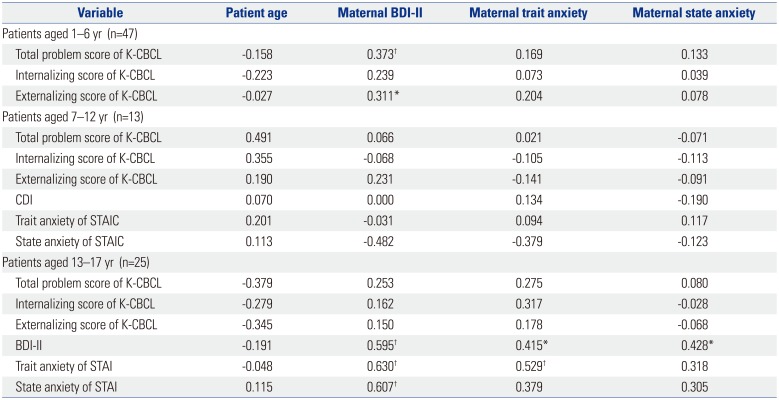
Table 1 lists the demographic and clinical characteristics of patients and their mothers. Patient mean age was 7.6 years. The total number of patients included in the analysis was 85. There were 47 infants and preschool-aged children in the 1–6 year patient age group, 13 school-aged children in the 7–12 year patient age group, and 25 adolescents in the 13–17 year patient age group. About 24.7% were diagnosed with acute lymphoblastic leukemia, and 10.6% were diagnosed with acute myeloid leukemia. About 9.4% had relapsed cancer.
Patients aged 1–6 years
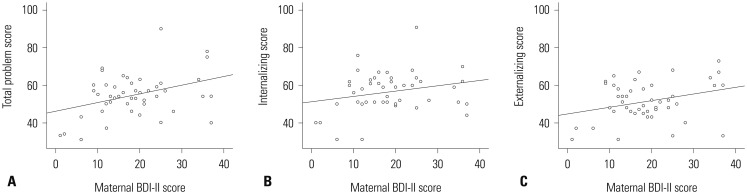
Maternal BDI-II score was positively correlated with patient total problem and externalizing scores (Fig. 1A and C), although there was no significant association between maternal BDI-II score and patient internalizing score (Fig. 1B). Among the variables, maternal BDI-II score was the only factor associated with patient total problem and externalizing scores (Table 2).
Patients aged 13–17 years
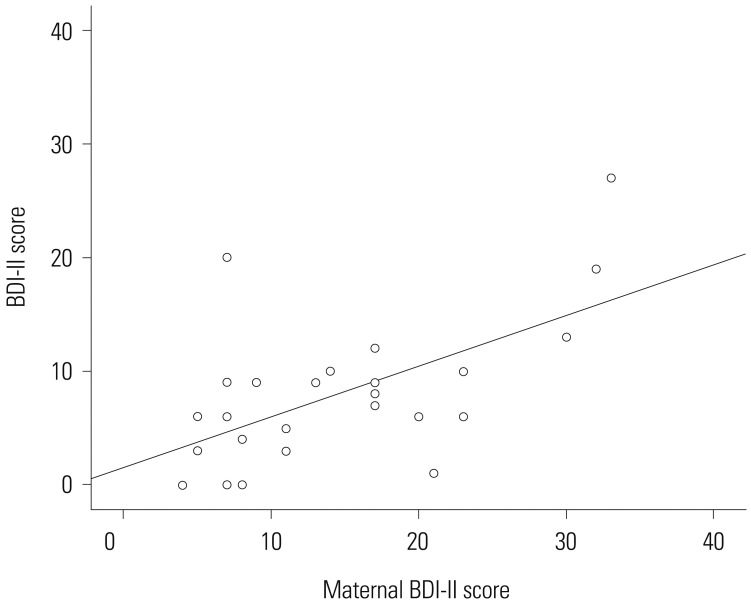
We conducted analyses of the association between patient emotional distress and other variables (Table 3). Patient BDI-II score was associated with various factors including maternal BDI-II (Fig. 3), maternal trait anxiety and maternal state anxiety scores. Patient trait anxiety score was associated with maternal BDI-II and maternal trait anxiety scores. Patient state anxiety was associated with maternal state anxiety. Factors related to the BDI-II score in patients aged 13–17 were identified using multiple stepwise linear regression analysis. Maternal BDI-II score was the only factor associated with patient depression (Table 4).
DISCUSSION
Our study extends the findings of previous research on the psychological responses of patients to cancer diagnosis by assessing the more immediate emotional responses within 3 months of diagnosis. Most previous studies examined patients with terminal cancer23 or cancer survivors,24 while others assessed patients during the first year after diagnosis.2125 In our present study, most patients were scored in the subclinical range of psychological inventories. This finding is comparable with the findings of previous studies. This might be related to patient's different coping strategies to deal with acute stress. In addition, we identified that maternal depression emerged as the strongest factor associated with subjective emotional distress in adolescents newly diagnosed with cancer.
In infants and preschoolers, emotion regulation is dyadic because the primary caregiver is central to providing regulation that an offspring needs, which in turn facilitates the development of autonomous emotion regulation.2627 Previous studies suggested that increased parenting stress predicted poorer behavioral, emotional, and social adjustments in children with cancer.2829 Greater illness-related parenting stress is correlated with greater parental emotional distress such as depression and anxiety.30 Manian and Bornstein31 suggested that infants of depressed mothers used more internally self-soothing strategies to reduce negative emotions than infants of mothers who were not depressed. In our sample, an elevated maternal BDI-II score was correlated with total problem score and externalizing score in patients aged 1–6 years. It seems that parenting issues, mediated by maternal depression, can lead to emotional distress in infants and preschoolers and result in externalized symptoms including aggressive behaviors. However, maternal BDI-II score was not correlated with internalizing score. This discrepancy might be due to the high ratio of boys to girls in patients aged 1–6 years. Previous studies reported that current maternal depression was related positively to internalizing score of girls and to externalizing score of boys.32 In addition, illness-related parenting stress is related to parental responsibility for managing treatment.33 Because children younger than 7 years old have less autonomy and depend more on their mothers, their mothers may feel a greater responsibility than mothers of children older than 7 years. In adolescent patients, depressive mood and anxiety were positively correlated with maternal depression; in contrast, subjective emotional distress in school-aged patients was not related to maternal depression.
There are several potential explanations for the discrepancy found between children and adolescents. The difference could be explained primarily by the development of empathy in adolescents. Two components of empathy, empathic concern and perspective thinking, increase throughout adolescence.34 Perspective thinking is a cognitive component of empathy that does not begin to emerge until childhood, although empathic concern which is an emotional component of empathy appears to stabilize in early childhood.3435 Perspective thinking allows the understanding of the mental state and viewpoints of others, and moderates the relationship between cognitive and emotional empathy.36 Hereby, adolescents with cancer may be more susceptible to maternal depression than school-aged children. This is in line with findings that subjective illness perception in adolescent and young adult cancer patients is the strongest predictor of their own stress symptoms and is significantly correlated with stress symptoms in caregivers.37
However, school-aged children have difficulties recognizing their mother's emotional status because of their immature empathy. In addition, they often perceive their illness as a punishment for a perceived wrong.38 School-aged patients' subjective depressive mood and anxiety may be most strongly related to their own beliefs about their illness rather than maternal emotional distress. Furthermore, emotional understanding in young children developes primarily through socialization processes within the family context, especially through the quality of mother-child relationships. Sympathy and personal distress responses to a mother's distress might facilitate the socialization process by allowing children to focus on their parent rather than their own distress, and providing opportunities for parents to respond to children's emotions facilitate emotional learning.39
This study has several limitations. First, the cross-sectional study design does not provide the ability to clearly discern psychological trajectories over time. In addition, the direction of the influence between parental distress and patient distress could not be elucidated. Future research may use a longitudinal study design to clarify the direction of this moderation effect. Second, the number of patients with relapsed cancer was not large enough to analyze the difference between the initial diagnosis and relapse. Relapse of cancer is known to be negatively associated with a child's self-perception and positively associated with trait anxiety.40 Third, the number of patients aged 7–12 was small compared to other age group, therefore, there might not be a significant correlation. Fourth, we were unable to make broader conclusion about vulnerable maternal characteristics. The inclusion of multiple variables including maternal age, coping strategies and attachment types of mothers would provide advanced results. Fifth, further research may benefit from focusing on more homogeneous samples of children with specific diagnosis of cancer or specific treatment received that may present specific types of stressors. And finally, we included cancer patients only in this study; further research is necessary to compare the differences between cancer diagnosis and other traumatic stressors.
In conclusion, this study suggests that the most important factor affecting the emotional distress of patients, especially adolescents, is maternal depression. Understanding the factors associated with emotional distress of cancer patients allows us to develop early psychiatric interventions including supportive psychotherapy for patients and their primary caregivers at the initial psychological crisis. Finally, the results suggest that early psychiatric assessment is important to reduce emotional distress and improve the quality of life of patients. Future research should continue to develop innovative interventions for managing emotional distress of patients in the oncology setting.


 XML Download
XML Download