

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of obesity has been increasing rapidly in many countries. In Korea, the incidence of obesity was 1.7 times higher in 2011 compared to 9.7% incidence 10 years ago.1 The incidence of non-alcoholic fatty liver disease (NAFLD) in Korea, Japan and north Asian countries has increased 3 folds from less than 10% to 30% over four decades since 1980s, and mostly related with metabolic consequence of over-nutrition with obesity such as insulin resistance (IR), diabetes, and metabolic syndrome.2 Non-alcoholic steatohepatitis (NASH), the severe form of NAFLD, is a common cause of chronic liver disease in children and adolescents, and the number of NASH patients has increased with the increasing number of obese children.3
NAFLD shows evidence of hepatic steatosis either by imaging or histology, and is associated with no causes of secondary hepatic fat accumulation. NAFLD may present as a spectrum of disease, ranging from asymptomatic steatosis with elevated or normal aminotransferases, NASH, and cirrhosis with complications of liver function, to hepatocellular carcinoma.4 NASH includes the presence of hepatic steatosis and inflammation with hepatocyte injury such as ballooning with or without hepatic fibrosis.5
In one-third of NASH patients, progression to liver fibrosis was found within 5 years of diagnosis, and the prevalence of cirrhosis development was found to be 11 times higher in patients with NASH than in patients with simple hepatic steatosis.6 Additionally, NAFLD in children may be associated with significantly shorter survival than the general population because of liver failure or cirrhosis, especially in NASH patients.7 To evaluate the severity of NASH, a liver biopsy is required, in which fibrosis is an important factor.
IR has an important role in the development of NASH by increasing hepatic fatty acid β-oxidation and oxidative stress. Free fatty acids (FFAs) also cause IR by inhibiting insulin-stimulated glucose uptake and glycogen synthesis. IR is impaired insulin sensitivity, which is a decreased tissue response to insulin-mediated cellular actions. This condition is commonly associated with obesity in both children and adults. However, a standard method to evaluate IR in children has not yet been established, although several methods are used to measure IR or insulin sensitivity. The euglycemic and hyperinsulinemic clamp study is the most accurate technique, however, this method is time consuming and requires frequent blood sampling.8 For more simplified measurement of IR, fasting insulin and glucose, homeostasis model assessment of IR (HOMA-IR), insulin sensitivity indices-FFA (ISI-FFA), and quantitative insulin sensitivity check index (QUICKI) have been developed.91011 In addition, several previous studies analyzed the association between IR and NASH.12 A recent Korean study clearly showed higher body mass index (BMI), higher HOMA-IR values, and increased triglyceride (TG) ≥150 mg/dL associated with the occurrence of NAFLD in non-obese subjects.13
Italian national survey earlier defined IR as HOMA-IR >2.5 in pre-pubertal children and HOMA-IR >4 in pubertal children,14 and cut-off values for HOMA-IR according to age and gender have been proposed in Korean children and adolescents,15 and Korean men.16 However, there is limited data on the correlations between clinical manifestations and analysis of liver histopathology, especially in children and adolescents. Therefore, we aimed to investigate clinical characteristics according to the severity of NASH, and explore the relationship between NASH status and IR by using the IR indicators such as HOMA-IR, QUICKI, and ISI-FFA.
Go to : 
MATERIALS AND METHODS
Subjects
The study subjects included 41 children (25 males, 16 females) with NAFLD in whom liver biopsies were performed to assess the severity of liver pathology between July 2006 and September 2014, at the Department of Pediatrics, Hanyang University Hospital. The patients were 7 to 15 years old and did not have a hepatitis A, B, or C virus infection or a history of alcohol consumption, parenteral nutrition, or use of drugs.
Anthropometric data including body weight, BMI, and waist circumference were evaluated. To compare BMI across different ages and both genders, BMI Z-scores were calculated. The Z-score represents the number of standard deviations above or below the mean value based on standardized tables for children, as indicated by the Korean Journal of Pediatrics.17
Clinical features and biochemical findings including alanine aminotransferase (ALT), aspartate aminotransferase (AST), TG, cholesterol, high density lipoprotein-cholesterol, low density lipoprotein-cholesterol, FFA, fasting glucose, fasting insulin, IR, and insulin sensitivity were analyzed retrospectively. These laboratory tests were performed during the same period as the liver biopsy.
Insulin resistance and insulin sensitivity
IR and insulin sensitivity were calculated as follows: HOMA-IR=fasting insulin (µIU/mL)×fasting glucose (mmol/L)×0.55/22.5.10 ISI-FFA=2/(insulin×FFA+1); mean normal values of ISI (FFA) are reported to be around 1 in adults.1819 QUICKI was calculated as 1/[log fasting insulin (µIU/mL)+log fasting glucose (mg/dL)]. Impaired QUICKI was suggested as QUICKI below than 0.43 to 0.91 in the children.2021
Liver biopsy and histology
Liver biopsy was performed by an 18-gauge automatic gun [Autovac (BARD Angiomed, Karlsruhe, Germany)]. Before the biopsy, we selected the area in the right intercostal space to avoid the pleura and blood vessels, and disinfected the skin with povidone-iodine; local anesthesia was performed on the area of skin puncture. The needle of the biopsy gun was advanced 1–2 cm into the hepatic capsule, and at least 1.5 cm of tissue was biopsied from each patient under ultrasonic guidance.
NAFLD scoring system, designed and validated by the pathology committee of the NASH-Research Network, was used to evaluate the liver biopsy samples.22 Main histological features described in NASH/NAFLD, including steatosis, ballooning change, lobular inflammation, portal inflammation, and fibrosis, were scored using this scoring system. Simple steatosis is defined to show fatty infiltration in the hepatic tissue without fibrosis or ballooning. Steatosis was graded on a four-point scale: grade 0 (<5%), grade 1 (5–32%), grade 2 (33–66%), or grade 3 (>66%). Lobular inflammation was graded on a four-point scale: grade 0 (no foci), grade 1 (<2 foci/200×field), grade 2 (2–4 foci/200×field), or grade 3 (>4 foci/200×field). Portal inflammation was graded on a three-point scale: grade 0 (none), grade 1 (minimal), or grade 2 (greater than minimal). Hepatocyte ballooning change was graded on a three point scale: grade 0 (none), grade 1 (few ballooning cells), or grade 2 (many ballooning cells). Fibrosis was graded on a five-point scale: grade 0 (none), grade 1 (zone 3 perisinusoidal), grade 2 (perisinusoidal and portal/periportal), grade 3 (bridging fibrosis), or grade 4 (cirrhosis).
We calculated the NAFLD activity score (NAS) as an objective marker of NASH grade based on the sum of steatosis, lobular inflammation, and ballooning change scores and the group with score ≥5 were defined as NASH. Among the total 41 children, pathologic changes compatible with NAFLD were noted in 24; NASH with high NAFLD score was found in 16, and mild pathologic change with low NAFLD score was found in 8.
Statistical analysis
SPSS Statistics ver. 21.0 (IBM Co., Aronk, NY, USA) was used for statistical analysis of the data. A Mann Whitney U-test was performed for comparative analysis of the lab findings according to NAS. For the associations between clinical laboratory findings and liver pathology, a Jonckheere-terpstra test was performed. A p value less than or equal to 0.05 was considered statistically significant. This study was approved by the Institutional Review Board (IRB) of our institute (2015-11-016-002).
Go to :
RESULTS
Clinical characteristics and endocrine features
The mean patient age was 11.1±2.3 years (range, 7–15 years), and the majority of the 24 NASH patients were male (19 males and 5 females). Clinical characteristics and laboratory findings are summarized in Table 1. All patients had a BMI above the 85th percentile, and 18 patients were obese. The levels of AST and ALT were elevated to 69.9±48.6 and 134.6±111.5 IU/L, respectively. The FFA level was 578.9±253.2 µmmol/L, and fasting glucose and insulin were 96.5±11.2 mg/dL and 36.7±41.1 µIU/mL, respectively. The mean values of HOMA-IR were 5.33±3.65, QUICKI, 0.29±0.06, ISI-FFA, and 0.24, respectively.
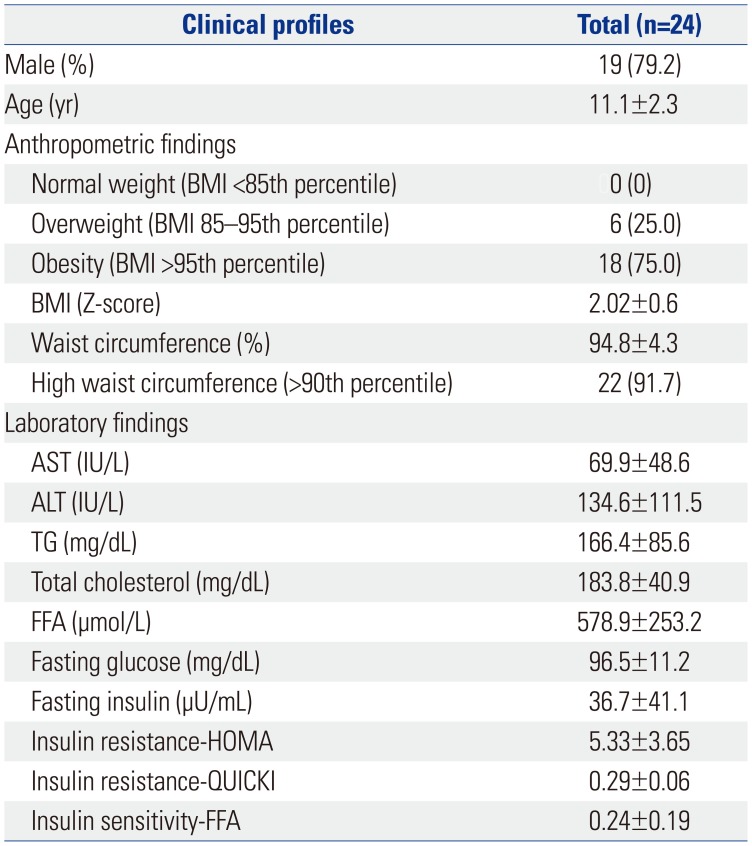
Table 1
Anthropometric and Biochemical Laboratory Data of the Patients
![]()
Histopathology of patients with NAFLD
The 24 patients with an NAFLD score were divided into two groups. The low score group included 8 patients with an NAS from 0 to 4, and the high score group included 16 patients with an NAFLD score from 5 to 8. The high NAS group had higher TG levels than the low NAS group; however, the mean age was lower in the high score group than in the low score group (Table 2). The tendencies of TG level and mean age were considered significant. Based on the p values for IR and sensitivity, however, these values were not considered significantly different between the two groups.
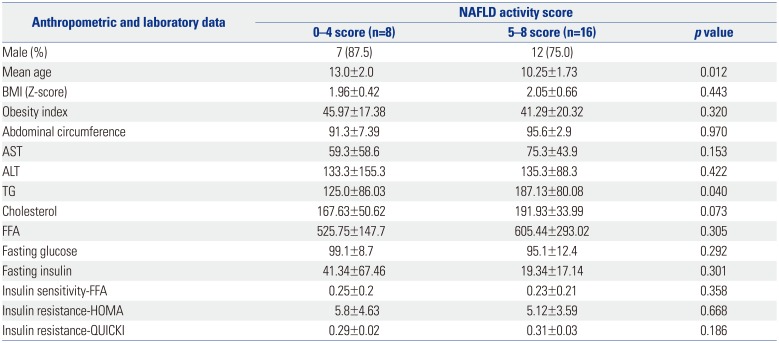
Table 2
Differences in Anthropometric and Laboratory Data Based on the NAFLD Activity Scores
![]()
The association between the hepatic pathologic findings and clinical and laboratory data
The severity of steatosis was statistically significantly associated with higher age, AST, and ISI-FFA. The severity of ballooning change was statistically associated with AST and TG. The severity of lobular inflammation was associated with the indices for HOMA-IR and QUICKI, and that of fibrosis was associated with higher indices of IR; fasting insulin, ISI-FFA, HOMA-IR, and QUICKI. In contrast, portal inflammation had no association with any clinical or biochemical laboratory data (Table 3).
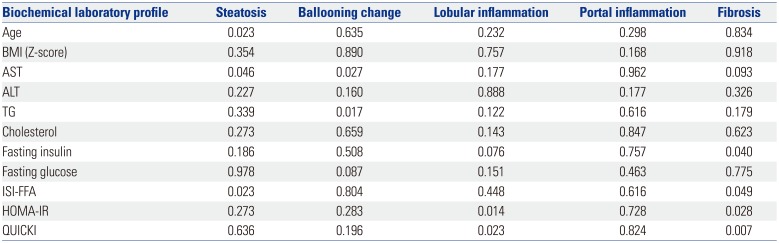
Table 3
Correlations between Biochemical Laboratory Results and Each Pathologic Finding (p values)
![]()
Insulin resistance in children with NASH
Hepatic fibrosis was highly related with IR. The severity of the fibrosis was strongly associated with higher fasting insulin, HOMA-IR, and lower QUICKI, ISI-FFA (Table 4).

Table 4
Correlations between Fibrosis Results and Each Laboratory Finding
![]()
Go to :
DISCUSSION
It has been well known that NASH is a hepatic portion of metabolic (IR) syndrome.232425 NASH has recently become one of the leading indications of liver transplantation in the United States.26 Furthermore, liver transplantation outcomes are worse in recipients with NASH or metabolic syndrome. Many recipients die due to cardiovascular complications and sepsis within a short follow-up period of 5 years.27 In 330 young patients with NASH who were morbidly obese, insulin-resistant, complicated with liver cirrhosis and end-stage liver failure, and underwent liver transplantation, 4% were pediatric patients, and 6% were younger than 25 years. The post-transplantation prognosis in these patients was very poor, and 30% died within a 4-year follow-up period.28
There are few studies on liver histopathology in NASH patients because it is difficult to perform a liver biopsy in pediatric patients. The present study highlights that severe hepatic pathology, such as hepatic fibrosis, is related with IR or insulin sensitivity index.
There are several potential mechanisms underlying NASH. One strong hypothesis among them is the ‘two-hit theory.’ The ‘first hit’ is an excessive hepatocyte TG accumulation resulting from IR and can be described as a TG imbalance. Fatty liver is caused by an accumulation of TG that is related with the first hit. This explains why a higher NAS is correlated with a higher TG level, as shown in Table 2. There are several mechanisms that affect the TG level. The first mechanism is an increased uptake of FFA. FFA contains TG that is hydrolyzed to FFA by lipoprotein lipase. Excessive FFA in the liver is converted to TGs, which leads to the accumulation of TG in the liver. The second mechanism is the suppression of FFA synthesis or increased synthesis in liver cells. This phenomenon depends on the intake of nutrients that can serve as substrates for fatty acid synthesis. Other mechanisms include reduced catabolism of FFA in liver cells or decreased release of TGs from liver cells. Increased IR can lead to the inhibition of lipolysis in lipid cells and the release of FFA from lipid cells in the liver.12
The ‘second hit’ involves an inflammatory injury to the liver due to oxidative stress. An increase in peroxidation and oxidative stress can activate stellate cells and accelerate liver fibrosis.12 As shown in Table 1 in the present study, most NASH patients were overweight and had large waist circumferences. We speculate that obesity stimulates the second hit because of fibrosis since leptin may be an important link between obesity and fibrosis. Oh, et al.29 also showed that the degree of NAFLD correlated with the degree of obesity. Obesity was shown to be required for the development of liver fibrosis in a steatohepatitis model.30
Jee, et al.31 found that hepatic ultrasonography was associated with NAS, steatosis, and ballooning change. Hepatic fibrosis, however, was not correlated with hepatic ultrasonography, therefore, a liver biopsy is still necessary to determine the most important information about the pathology of hepatic fibrosis. The finding in the present study suggests the relevance between IR and the degree of fibrosis because of the statistically significant correlation between these measures; one can predict the degree of liver fibrosis through the IR and ISI using a blood test. A liver biopsy is a very invasive test, which makes it difficult to perform in NAFLD patients. Furthermore, parents of many pediatric patients are very reluctant to allow their children to undergo a liver biopsy. In the future, we can apply this association to confirm liver fibrosis without biopsy. Although not statistically significant, high insulin level and HOMA-IR were observed even in the group with lower NAS, as shown in Table 2. It might be explained by the fact that fibrosis could progress in some patients with lower NAS, which was calculated by the sum of steatosis, lobular inflammation, and ballooning change, excluding fibrosis score.
In a study on adults with NAFLD, more severe hepatic fibrosis was correlated with increased liver-related morbidity and mortality.32 In addition, NASH has been recognized as an important cause of cirrhosis, liver transplantation, and hepatocellular carcinoma.33 Our present results found a correlation between fibrosis and IR, and that obesity may contribute to this result. Singh, et al.34 showed that the fibrosis progression rate is higher in patients with NASH, while mild degree NAFLD can also lead to fibrosis. NAFLs have mild lobular inflammation without hepatocyte ballooning or fibrosis, although this can progress to definite NASH because of persistent inflammation. In this case, there is a risk of poor outcomes and progressive liver damage, with fibrosis being the key to liver damage progression. In this analysis, the AST and ALT ratios were correlated with fibrosis progression. Recently, AST and ALT have been focused as markers of definite NASH. Our present study showed that higher AST was related to higher steatosis that defines the NASH score, and Patton, et al.35 also found that highly severe NASH was associated with high AST levels.
A previous study showed that HOMA-IR was higher in the NAFLD group than in the control group and was also significantly correlated with liver enzyme levels. Moreover, they found a significant difference in HOMA-IR between simple steatosis patients and NASH patients.36 In adults, QUICKI ranged between 0.45 in healthy individuals and 0.30 in diabetic patients, while it ranged from 0.31 to 0.33 in obese children of Swedish population study and IR pediatric patients.37 In our cohort, impaired IR were identified using HOMA-IR and QUICKI, and especially impaired IR were found in subjects with lobular inflammation and severe fibrosis in liver histopathology. In addition, decreased insulin sensitivity was associated with more severe steatosis and fibrosis. Therefore, there was a significant impairment of IR and decrease of insulin sensitivity in our co-hort, indicating that IR plays an important role in development and progression of NASH. IR indices showed significant differences according to the severity of hepatic fibrosis. On the other hand, however, there was no significant correlation between fasting glucose level and the severity of hepatic fibrosis in our study. Carter-Kent, et al.38 also reported no association between fasting glucose and hepatic fibrosis in children with NASH.
Takahashi, et al.39 reported that steatosis was more severe in pediatric cases than in adult cases. In contrast, ballooning and lobular inflammation were milder in pediatric cases. The severity of periportal fibrosis was almost the same in both cases. In our study, more than half of the patients showed higher grade of steatosis and lower grade of lobular inflammation.
Age can influence the severity of NASH. As shown in Table 2, mean patient age in our study was higher in the high NAS group than in the low score group, and hepatic steatosis was corre-lated with age, AST, and ISI-FFA (Table 3). In liver pathology, hepatic steatosis is known as the ‘first hit’ in the development of NASH.40 Severity of hepatic steatosis was also predicted based on age. Accordingly, the amount of hepatic fat accumulation increases with aging and the duration of obesity. Recently, the effects of hepatic steatosis on IR have been elucidated. Cali, et al.41 reported that NASH patients showed impairment in beta-cell function and a decrease in insulin sensitivity, both of which indicate the severity of hepatic steatosis. The harmful effects of fat accumulation in the liver can affect insulin sensitivity at a multi organ level. Consequently, insulin secretion is decreased so that it is difficult to maintain glucose level, developing beta-cells long-term. A similar Korean study showed that the more hepatic steatosis is severe, the more type 2 DM presents, concluding that IR caused by hepatic fat accumulation may be a critical mechanistic connection.42
In obese children, beta-cell function is reduced according to age. Arata, et al.12 performed a meta-analysis of several studies to suggest the underlying mechanism in the development of IR in pediatric nonalcoholic steatohepatitis and nonalcoholic fatty liver disease; IR is an important factor in the first hit of the two-hit model of NASH.
In conclusion, we found that correlations among hepatic histopathologic findings, clinical characteristics, and IR that have an important role in the development of NASH. Patients with high IR had more severe lobular inflammation and hepatic fibrosis. The higher the serum TG level, the higher the NAS, and the more severe the ballooning change. Finally, analyses of biochemical and endocrine parameters could be applied to determine the severity of hepatic pathologic status in patients with NAFLD, especially in many children who cannot undergo a liver biopsy.
Go to :
 XML Download
XML Download