

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Non-erosive reflux disease (NERD) is defined as the presence of the classical symptoms of gastroesophageal reflux disease (GERD) without esophageal mucosal injury determined by upper gastrointestinal endoscopy.1 It is regarded as one of the two main phenotypes of GERD, the other being erosive esophagitis, in which mucosal injury such as erosion or ulceration is obvious during endoscopy. GERD is a common disorder, and the prevalence of at least weekly heartburn and/or acid regurgitation is 9–28% in Western countries.2345 Although GERD is less prevalent in Asian countries and Korea, occurring in only 2.5–8.2% of people,5678910 however, it is emerging as a leading digestive disorder and has a negative impact on quality of life. Most cases of GERD are of the NERD phenotype, and the proportion of patients with NERD is estimated as 50–85% of the GERD population.111213
The increasing prevalence of GERD appears to be related to that of obesity. Obesity is common in the Western world, and is becoming increasingly common in Asian countries as well. In Korea, the prevalence of obesity [defined as a body mass index (BMI) ≥25 kg/m2 according to the Korean Society for the Study of Obesity] is increasing, and was reported as 26.9% in 1998 and in 32% in 2011.1415 Population-based studies have shown that overweight or obesity are both positively associated with GERD symptoms.16171819 Many studies have also found a positive correlation between obesity and GERD-associated esophageal erosion (e.g., erosive esophagitis, Barrett's esophagus).6182021 However, information regarding the relationship between obesity and NERD is still scarce and inconsistent. One population-based study compared patients with NERD to people from a normal control population, and identified a number of risk factors for NERD.9 Low BMI (<23) was one of the risk factors for NERD. Contrary to the above, however, an another study showed reverse results and a positive correlation between NERD and central obesity.22
With the above in mind, we aimed to investigate the risk factors for NERD by comparing people with the disease to healthy controls from a homogeneous Korean population, and analyzed the associations between BMI/waist circumference (as markers of obesity and central obesity, respectively) and NERD after adjusting for several confounding factors.
MATERIALS AND METHODS
Study design and population
This was a case-control study. We included the participants who had visited the Digestive Disease Center of the Cheju Halla General Hospital for a medical check-up from December 2012 to May 2013. The general medical check-up program included esophagogastroduodenoscopy, abdominal ultrasonography and/or contrast-enhanced computed tomography, and laboratory tests. We excluded subjects who had esophageal erosion or ulceration: i.e., erosive esophagitis (n=26), Barrett's esophagus (n=4), hiatal hernia (n=26), and active mucosal lesions including peptic ulcers (n=12). Subjects with a history of gastric surgery (n=4), proton pump inhibitor/histamine-2 receptor antagonist/aspirin or non-steroidal anti-inflammatory drug therapy during the previous week (n=6), diabetes mellitus (n=31), achalasia (n=1), end-stage renal or liver disease (n=11), or malignancy (n=14) were excluded because of the possibility for these issues to confound the results. Finally, a total of 378 subjects were enrolled in this study. Informed consent was obtained from all participants, and the study was approved by the Institutional Review Board of Cheju Halla General Hospital.
Data collection
Demographic data (age, gender, smoking status, alcohol consumption, medical or surgical history, and history of medication) were obtained before the endoscopic procedure. All subjects were offered a Korean version of questionnaire, the GerdQ,23 which probed the onset, frequency, and severity of classical GERD symptoms (heartburn, acid regurgitation) experienced over the past year as well as atypical symptoms (non-cardiac chest pain, hoarseness, chronic cough, and chronic sore throat). GERD was considered to be present if the total score was ≥8, or ≥3 for the high impact questions according to the GerdQ scoring system. All subjects underwent upper endoscopy, abdominal computed tomography and/or ultrasonography, and laboratory tests during the routine check-up.
Height was measured using a portable stadiometer, and weight was measured using a calibrated balance scale. BMI was calculated as the ratio of weight to the square of height (kg/m2). Obesity was defined as a BMI ≥25 kg/m2 according to the Korean Society for the Study of Obesity.14 Moreover, waist circumference was measured at the midpoint between the lower border of the rib cage and the iliac crest by trained personnel. Central obesity was defined as a waist circumference of ≥90 cm in men and ≥85 cm in women according to the Korean Society for the Study of Obesity.24
Endoscopic procedures were carried out using an upper endoscope (GIF H260, Olympus Optical Co., Ltd., Tokyo, Japan) after pharyngeal anesthesia by an endoscopist with a specialty certificate who was blinded to the results of the GerdQ questionnaire. The severity of esophagitis was classified into four grades according to the Los Angeles classification.25 However, minimal changes (erythema, blurring, friability, mucosal edema, increased vascularity) were not considered as erosive esophagitis. Gastroduodenal lesions, hiatal hernia, and Barrett's esophagus (a pink salmon colored esophageal lining that extends a distance up to the esophagus from the gastroesophageal junction) observed during endoscopy were also recorded. GERD was classified as either erosive esophagitis or NERD according to the presence or absence of esophageal erosions or ulcerations.
Statistical analysis
Categorical variables were expressed using numbers with proportions (%), and continuous variables were expressed using means and standard deviations. Pearson's chi-square test with Fisher's exact test was used to compare the categorical variables between the NERD and non-NERD groups, while the Mann-Whitney U-test was used to compare the continuous variables. The variables tested were age, gender, smoking status, alcohol consumption status, chronic gastritis, impaired glucose tolerance, hypertension, fatty liver, biliary disease, cerebrovascular accident, azotemia, hyperlipidemia, BMI, and waist circumference. Univariate and multivariate analyses of the factors associated with NERD were performed using a logistic regression model. For each factor, an odds ratio (OR) with 95% confidence interval (CI) was estimated. These results were also confirmed using a propensity-scoring model. Propensity scorematching analysis was carried out using logistic regression to establish propensity scores for patients in the NERD and non-NERD groups. All variables were included in the propensity models except for the outcome variables (BMI and waist circumference). The model was then used to provide a one-to-one match between the two groups using the nearest-neighbor method.26 Multiple logistic regression analyses with matched data were then repeated to assess the association between obesity/central obesity and NERD after adjusting for propensity scores and all covariates. A p value<0.05 was considered statistically significant. All statistical analyses were performed with SPSS software package, version 21 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographics and clinical characteristics
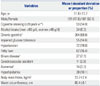
A total of 378 subjects, including 119 NERD patients and 259 controls, were included in this study. The demographic and clinical characteristics of the included subjects are summarized in Table 1. Their mean age was 51.8±13.7 years, the proportion of men was 47.9%, mean BMI was 23.7±2.4 kg/m2, and mean waist circumference was 80.4±6.1 cm. The prevalence of obesity was 17.0% (19.3 and 15.8 with or without NERD, respectively; p=0.400), and the prevalence of central obesity was 19.3% (27.7 and 15.4 with or without NERD, respectively; p=0.005) (Table 2).
Univariate and multivariate analyses of factors associated with NERD
Univariate analysis showed that younger age, female gender, and central obesity were significantly associated with NERD (p=0.020, 0.015, and 0.005, respectively) (Table 3). Smoking status (heavy smokers vs. others) and drinking status (heavy drinkers vs. others) were not significantly associated with NERD (p=0.591 and 0.840, respectively). Other variables including obesity or biliary disease did not show significant associations with NERD. When only gallbladder stone was included in univariate analysis, there was also no association between gallbladder stone and NERD (OR=1.242, p=0.121). Multiple logistic regression analyses adjusting for age, gender, smoking status, alcohol consumption status, chronic gastritis, impaired glucose tolerance, hypertension, fatty liver, biliary disease, cerebrovascular accidents, azotemia, hyperlipidemia, obesity, and central obesity were performed. In the analysis, obesity was not a determinant of NERD. However, the correlation between central obesity and NERD was still observed after adjusting for clinical variables (OR=2.546, 95% CI 1.472–4.405, p=0.001). Female gender (OR=1.928, 95% CI 1.217–3.056, p=0.005) and younger age (OR=1.798, 95% CI 1.146–2.824, p=0.011) were also independent risk factors for NERD.
Propensity score-matching analysis
Table 2 presents the clinical characteristics of the subjects with and without NERD before and after matching using propensity scores. Propensity score matching was employed to adjust the baseline demographics and clinical characteristics between the NERD and non-NERD groups, and to confirm the results of the previous analyses. After adjusting for 12 clinical variables, 114 patients with NERD were matched to 114 healthy controls. All variables were well balanced between the two groups. The average standardized difference was 0.248 before matching, and decreased to 0.066 after matching. Patients with NERD also presented with a higher prevalence of central obesity than healthy controls (28.1% vs. 7.9%). In multiple logistic regression analyses performed after adjusting for propensity scores and all covariates, obesity was not associated with NERD. However, central obesity remained an independent and significant risk factor for NERD (OR=4.553, 95% CI 2.508–10.071, p<0.001) in the propensity score-matching analysis.
DISCUSSION
In this cohort of patients who presented for medical check-ups, we found a positive association between central obesity and NERD after adjusting for several potential confounding factors including age, gender, smoking status, and alcohol consumption. This association remained significant even after adjusting for propensity scores and all covariates (4.5-fold increase). However, obesity was not associated with NERD after adjusting for confounding factors. Other risk factors for NERD included female gender and younger age.
Previous studies have demonstrated significant associations between GERD and obesity/central obesity. However, data concerning the risk factors for NERD are scarce. Only one study22 from Korea reported a positive association between NERD and central obesity, but the results were not derived from a prospective investigation. Although this was not a prospective trial, our present study was conducted using a propensity score-matching method. Considering different sequelae or the natural courses of obesity and central obesity, the present findings are valuable and provide additional information concerning the risk factor of NERD.
In this study, central obesity but not obesity itself was related with NERD. The mechanism of how central obesity can increase the risk of gastroesophageal reflux symptoms is still speculative and maybe multifactorial. Several hypotheses could be suggested to explain the association. One of the possible mechanism is impaired function of the lower esophageal sphincter (LES). The LES acts as a physiological barrier to prevent gastric contents from refluxing to the esophagus. The impaired function of LES have been observed to be more common in patients with central obesity.2728 Intra-abdominal pressure is an another possible explanation. Mechanical effect of adipose tissue within the abdominal cavity and elevated intra-abdominal pressure may lead the relaxation of the LES and the consequent reflux of acid. Some authors suggested that hormonal factors related to visceral adipose tissue, including adiponectin, leptin, tumor necrosis factor-alpha, or others, are also important in the pathogenesis of symptoms of NERD.29 Various kinds of adipocytokines may act systemically, and also influence integration of gastroesophageal junction and enhance gastric secretory function.303132 Future studies need to focus on the association between these factors and the etiology of NERD.
In the present study, we evaluated the association between BMI or waist circumference and NERD. Waist circumference is a simple, widely advocated marker of central obesity.33 We measured waist circumference at the midpoint between the lower border of the rib cage and the iliac crest according to the World Health Organization recommendations, because the inter- and intra-observer reliability and reproducibility were found to be high at this point.34 Our study revealed that the increased prevalence of NERD was not associated with BMI (a marker of obesity), but was associated with waist circumference (a marker of central obesity). Recent studies have suggested that the distribution of body fat, especially the visceral fat, is a more significant factor in terms of obesity. One study found that abdominal diameter rather than BMI was associated with frequent gastroesophageal reflux symptoms.35 Furthermore, based on the measurement of abdominal fat tissue by computed tomography, several studies have demonstrated a significant association between visceral fat and gastroesophageal reflux symptoms.2136 Further studies are needed to explain the main underlying mechanism of the relationship between central obesity and NERD.
The results of this study showed that female gender and younger age were also related with NERD, and this finding was consistent with those of previous reports.4920373839 The different perceptions of gastric sensations according to gender/age may have played a role in the different reflux symptoms observed. Hormonal or physical factors may be associated with differences in the prevalence of NERD between men and women, or between younger and older patients.
This study had several limitations. First, false positivity or negativity is possible when defining GERD symptoms using the GerdQ questionnaire (65% sensitivity and 71% specificity).23 In addition, the Korean version of the GerdQ used in our study has not been officially validated in Korea. It is important to find out whether diagnostic threshold scores for GERD are appropriate for Korean patients. Thus, further studies should be needed to validate GerdQ for Korean patients. Second, the issue is whether these patients with symptoms and negative endoscopy truly have NERD or functional heartburn. This requires the use of objective measures of esophageal acid exposure. However, this study was health check-up based study. Therefore, we did not measure esophageal pH nor exclude esophageal hypersensitivity. Third, the study participants were self-motivated to attend screening medical check-ups, and selection bias might therefore be present. The members of the study population, who could afford the costs of the check-up program, were more likely to be from the higher socioeconomic group. Fourth, the proportion of NERD patients in our study, about 31%, is too high. Study subjects included not only person under health insurance-medical check-up program, but also volunteer who would like to receive medical check-up examination such as CT or/and endoscopy due to their symptom. This point could lead to a selection bias. Fifth, Helicobacter pylori infection and the effect of the participants' diets, which could be potential confounding factors, were not considered in the analyses.
In conclusion, our results showed that central obesity is an independent risk factor for NERD. These findings support the presence of an association between central obesity and reflux disease, even in the absence of esophageal erosion (NERD). Our findings will have important implications for the prevention and management of NERD, and future studies should be built on these findings to explore potential therapeutic and preventative measures related to NERD.


 XML Download
XML Download