

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic right ventricular (RV) pacing could deteriorate left ventricular (LV) systolic function and increase mortality via pacing-induced electrical and mechanical dyssynchrony,12345 particularly in patients with pre-existing LV systolic dysfunction (LVSD).167 However, even in patients without underlying LVSD, chronic RV pacing can cause new-onset LVSD, which can be defined as pacing-induced cardiomyopathy (PiCM).38
Cardiac resynchronization therapy (CRT) corrects electro-mechanical dyssynchrony and is now established as a standard treatment for advanced heart failure (HF) patients with a pacemaker (upgrade CRT) or without a pacemaker (de novo CRT).91011 However, it remains unclear whether upgrade CRT shows better outcomes than de novo CRT,12131415 and no previous studies have investigated underlying LV function before pacemaker implantation in patients receiving upgrade CRT.12131415
We hypothesized that the efficacy of CRT would be greater in patients with PiCM (upgrade CRT for PiCM) than in those without PiCM (upgrade CRT for non-PiCM) or those treated by de novo implantation (de novo CRT). Therefore, this study aimed to compare the effect of CRT between the upgrade and de novo CRT groups, as well as between the PiCM upgrade and non-PiCM upgrade groups.
MATERIALS AND METHODS
Patients and baseline assessment
We enrolled consecutive patients who received CRT at our center from March 2012 to July 2015. Patients with 1) drug-refractory advanced HF with New York Heart Association (NYHA) class III or ambulatory IV, 2) LV ejection fraction (LVEF) <35%, and 3) QRS duration >120 ms were included. Exclusion criteria included 1) switching off the CRT device within 3 months or 2) a follow-up duration of less than 3 months after implantation.
PiCM was defined when all of the following criteria were met: 1) LVEF prior to permanent pacemaker (PPM) insertion ≥50%, 2) new-onset LVSD (LVEF <35%) in pacing-dependent (>90% RV pacing)16 patients, and 3) the absence of other causes of HF, including previous myocardial infarction, valvular heart disease, tachycardia-induced cardiomyopathy, toxic (alcohol or chemotherapy) cardiomyopathy, hypertensive cardiomyopathy, myocarditis, or other infiltrative diseases. All CRT upgrade patients who did not fulfil the criteria for PiCM were classified into non-PiCM. We categorized the patients into three groups: PiCM-upgrade, non-PiCM upgrade, and de novo CRT (Fig. 1).
Baseline information, such as NYHA functional class and echocardiographic and electrocardiographic (ECG) parameters, was collected in all patients. Echocardiographic parameters included LVEF, end-diastolic dimension (LVEDD), end-systolic dimension (LVESD), end-diastolic volume (LVEDV), and end-systolic volume (LVESV). Additionally, pre-PPM LVEF was investigated in the upgrade CRT groups. ECG parameters encompassed the duration and morphology of the QRS complex. The baseline QRS morphology was categorized as left bundle branch block (LBBB) when all of the following criteria were met: 1) QRS duration >120 ms, 2) QS or rS in lead V1, and 3) monophasic R wave with no Q wave in lead V6 and I; paced QRS complexes in the upgrade groups and native QRS complexes in the de novo group were used for this classification. We also investigated HF duration, defined as the time interval between the first time a patient received diuretics or vasodilator/inotropic therapy for HF symptoms of congestion and/or low cardiac output and CRT implantation. The Institutional Review Board at Samsung Medical Center approved the study protocol and waived the requirement for informed consent.
Device therapy
CRT implantation was performed under local anesthesia using a transvenous approach. The LV lead was preferably placed into the anterolateral, lateral cardiac veins, or posterolateral ventricular veins. An epicardial LV lead was screwed into the lateral mid-LV segment via thoracoscopic surgery unless the transvenous approach via the coronary sinus was successful. The position of the RV or LV lead was confirmed by left and right anterior oblique fluoroscopic images. RV lead positions were classified as apical or septal. LV lead positions were classified as basal, mid, or apical in the right anterior oblique view and as anterior, anterolateral, lateral, posterolateral, or posterior in the left anterior oblique view.17 After implantation, atrioventricular and ventriculo-ventricular delays were determined showing the greatest stroke volume (Doppler-guided) or narrowest QRS duration (ECG-based) before discharge.
Follow-up assessment and outcomes
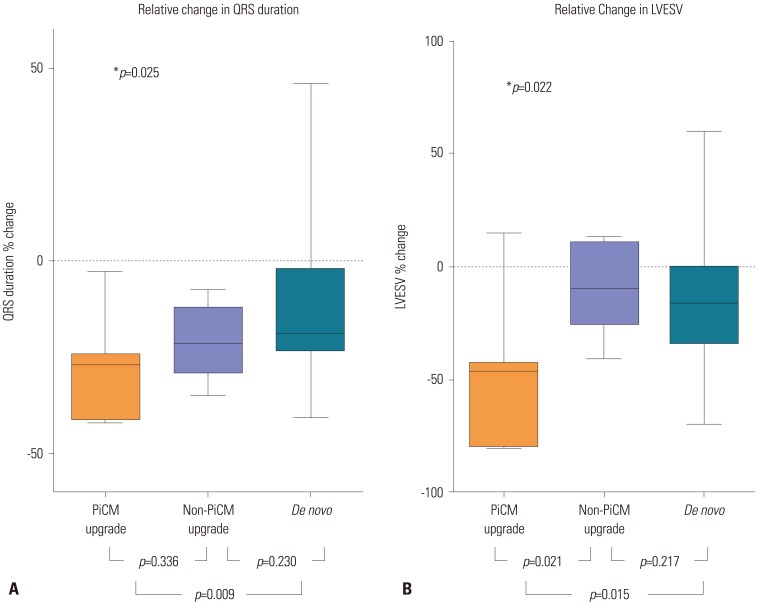
The primary outcome was electrical and mechanical reverse remodeling evaluated at 6 months after CRT implantation. For assessment of electrical reverse remodeling, absolute [(pre-CRT-post-CRT)] and relative [(pre-CRT-post-CRT)/pre-CRT×100, %] change in the QRS duration was calculated. In a similar way, absolute and relative changes in LVESD, LVEDD, LVESV, LVEDV, and LVEF were calculated for mechanical reverse remodeling.
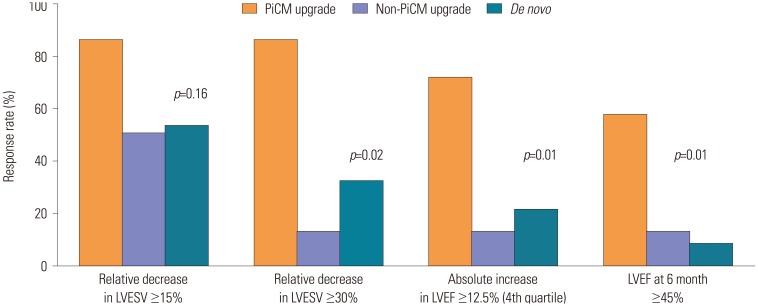
Secondary outcomes included improvement in symptoms assessed by change in NYHA class, responder rate, and long-term clinical outcomes. CRT responders were defined as follows: 1) ‘clinical responder’ for patients with any improvement in NYHA class, 2) ‘echocardiographic responder’ for patients with a relative decrease in LVESV by ≥15%, and 3) ‘super-responder’ for those with any improvement in NYHA class and a relative decrease in LVESV by ≥30%. Super-response rates were also assessed according to LVEF criteria as follows: 1) LVEF increase ≥fourth quartile or 2) LVEF ≥45% at 6 months after CRT.
Long-term clinical outcomes were assessed at the last follow-up in terms of all-cause death, cardiac death, heart transplantation, HF-related rehospitalization, and major adverse cardiac events (MACEs), encompassing cardiac death, heart transplantation, and HF-related rehospitalization.
Statistical analysis
Continuous variables are presented as medians with interquartile ranges and categorical variables are presented as numbers with percentages. Comparisons between groups were performed using chi-square tests, Mann-Whitney U tests, or Kruskal-Wallis tests, as appropriate. Survival free from adverse clinical outcomes was estimated by Kaplan-Meier curve and compared by log rank test. A Cox proportional hazard model was used to assess the risk factors for clinical composite events, and the logistic regression method was used to determine the predictors of a super-responder. Variables for which the p value was <0.2 were included in multivariate analysis. Statistical analyses were performed with the IBM SPSS Statistics version 23 (IBM Corporation, Armonk, NY, USA). All tests were two-tailed, and a p value<0.05 was considered statistically significant.
RESULTS
Patients and baseline characteristics
We identified 82 patients who underwent a CRT procedure during the enrollment period. Five of these patients were excluded because of the following reasons: two patients (one patient in the non-PiCM upgrade and one in the de novo group) were followed for less than 3 months, one patient (de novo group) died after the CRT procedure during the admission period, and two patients (de novo group) had their CRT devices turned off due to worsening HF symptoms. Of the remaining 77 patients, 62 underwent de novo implantation of CRT devices (de novo group), and 15 had their old PPM replaced by a CRT device (upgrade group). Indications for a pacemaker and RV pacing burden in CRT upgrade patients are summarized in Supplementary Table 1 (only online). Among the 15 patients in the upgrade group, seven met the criteria for PiCM, showing normal LVEF before PPM insertion and no definite cause of LVSD before CRT implantation (the PiCM upgrade group), while the remaining eight had reduced LVEF prior to PPM insertion (the non-PiCM upgrade group) (Fig. 1).
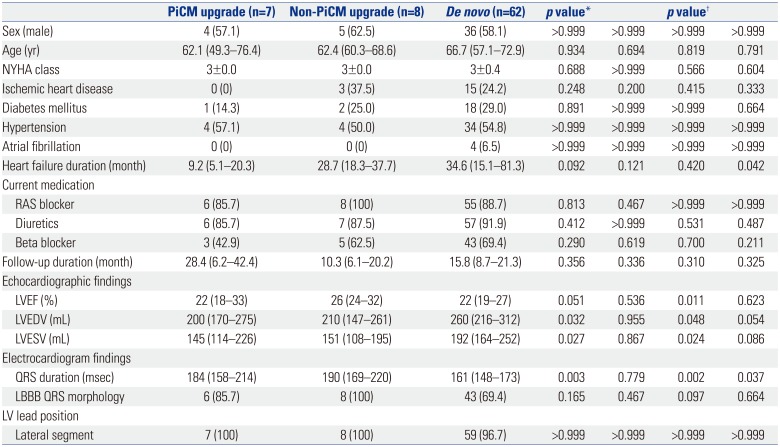
There were no differences in baseline demographic characteristics among the groups. For echocardiographic findings, the non-PiCM upgrade group showed the highest median LVEF, while LV volumes were greatest in the de novo group. QRS duration in both upgrade groups was significantly longer than that in the de novo group, and LBBB morphology tended to be more frequent in the upgrade groups. Most patients in all three groups had their LV leads in lateral (anterolateral, lateral, or posterolateral) LV segments (Table 1).
Primary outcomes
Fig. 2 and the Supplementary Table 2 (only online) show the primary outcomes. The percent decrease in QRS duration was greatest in the PiCM upgrade group (26.8% vs. 21.4% vs. 19.0%, p=0.025). The percent reduction in LVESV was significantly greater in the PiCM upgrade group than in the other two groups at 6-month follow-up (46.2% vs. 9.4% vs. 18.1%, p=0.022).
Secondary outcomes
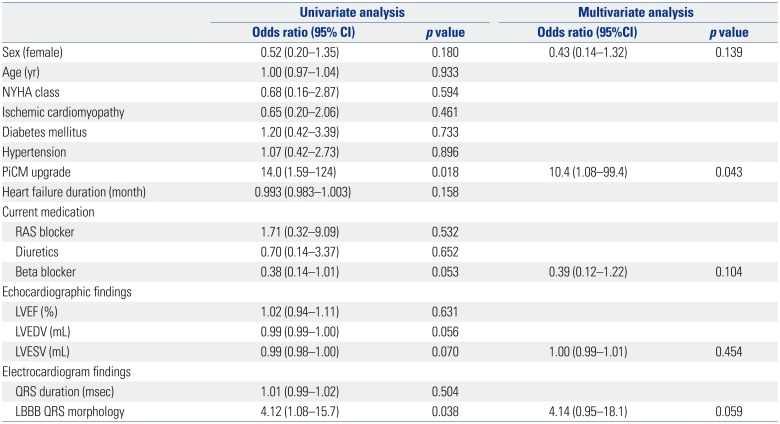
The PiCM upgrade group showed the highest responder rates, although the clinical and echocardiographic responder rates at 6 month did not reach statistical significance (Table 2, Fig. 3). Especially, the super-responder rate was remarkably higher in the PiCM upgrade than the other groups (6.9 and 2.6 times higher than in the non-PiCM upgrade and de novo group, respectively). The super-response rates according to LVEF criteria were also highest in the PiCM upgrade group (Fig. 3). On univariate and multivariate analyses, the PiCM upgrade group showed a significant association with super-responders (odds ratio 10.4, 95% confidence interval 1.08–99.4, p=0.043) (Table 3).
Patients underwent follow-up for a median of 15.8 (7.4–21.6) months, with no significant differences in follow-up duration among the groups. However, the PiCM upgrade group showed a tendency toward more favorable outcomes in terms of MACEs, compared to the other patient groups (p=0.059) (Fig. 4). More detailed clinical outcomes are summarized in Supplementary Table 3 and Supplementary Fig. 1 (only online).
DISCUSSION
In this study, PiCM upgrade was associated with more favorable outcomes with regard to electrical and mechanical reverse remodeling. Furthermore, PiCM upgrade was an independent predictor of CRT super-response. Survival analysis showed that clinical outcomes tended to be better in the PiCM upgrade group than the other groups.
Previous studies comparing the efficacy of CRT between upgrade and de novo groups showed conflicting results.12131415 In a prospective observational study including 135 CRT cases, the authors showed that upgrade CRT had more favorable outcomes than de novo CRT over a period of 4 years in terms of death, heart transplantation, or LV assist devices.15 However, no significant differences were observed in functional class change, QRS narrowing, and mortality at 1-year follow-up in the European CRT Survey, which compared 692 cases of upgrade CRT against 1675 of de novo CRT.14 This conflicting data might result from the fact none of the previous researchers specified the efficacy of upgrade CRT according to initial pre-PPM LV systolic function. In other words, patients with preserved pre-PPM LVEF (PiCM upgrade) and those with reduced pre-PPM LVEF (non-PiCM upgrade) were all incorporated into the same group, increasing the heterogeneity of the upgrade group. On the contrary, we made an extra effort to break down the upgrade CRT group into the PiCM and non-PiCM upgrade subgroups; we investigated LVEF prior to PPM implantation and the presence of other causes of LVSD by a comprehensive review of patient medical records, including clinical information, echocardiography, ECG and other imaging and laboratory findings. We hypothesized that patients with PiCM would be better CRT responders than those in the other CRT groups, because, by definition, most of them had non-ischemic substrate and LBBB pattern, which are well-known predictors for favorable CRT response.18192021 PiCM patients have other favorable features as well, including a greater degree of QRS narrowing after CRT upgrade.192022 and a shorter duration of HF than those treated by de novo CRT implantation.222324
In our data, almost half of patients (46.7%) in the upgrade CRT group were classified as PiCM, according to the definition mentioned above in the Methods section. As compatible with our hypothesis, the PiCM upgrade group showed the greatest electro-mechanical reverse remodeling (p<0.05) and the lowest rate of adverse events, including cardiac death, heart transplantation, and HF-related rehospitalization (p=0.059). We believe statistical significance could also be achieved for long-term clinical outcomes if a greater number of patients were followed for a longer period of time.
Although patients in the PiCM upgrade and non-PiCM upgrade groups shared similar manifestations of LV dilation, systolic dysfunction, and PPM dependency, clinical scenarios might have been quite different. In the PiCM upgrade group, conduction disorder requiring artificial pacing came first, and then LV dilatation and systolic dysfunction followed chronic RV pacing. However, in the non-PiCM upgrade group, pre-existing LV dilation and systolic dysfunction likely brought about a subsequent conduction disorder. Therefore, CRT could be a fundamental treatment for PiCM as it corrects the primary cause of LVSD.
There were several limitations of our study. As a single-center study of a small number of patients, there are concerns regarding selection bias. Especially, this study is underpowered to perform multivariate analysis for predictors of super-responder due to small patient number in upgrade groups. Furthermore, there was no standardized follow-up protocol, and retrospective data were collected for a relatively short follow-up duration. To overcome these limitations, we are also conducting analyses using nationwide, multicenter data.
The PiCM upgrade group showed better CRT response, compared to the non-PiCM upgrade and de novo groups, in terms of electrical and mechanical reverse remodeling. Therefore, CRT upgrade should be considered a fundamental therapy for patients with unexplained ongoing LVSD after PPM implantation.



 XML Download
XML Download