

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is one of the leading cancers among females, resulting in approximate 1.7 million cases and 522 thousands deaths in 2012.1 Based on hormone receptor, as well as human epidermal growth factor receptor type 2 (HER2) status, breast cancer could be classified into several subtypes as follows: luminal A, luminal B, HER2/neu+, and triple-negative.2 Triple-negative breast cancer (TNBC) is defined as tumors that lack expression of estrogen receptor (ER), progesterone receptor (PR), and HER2.3 Due to its specific receptor status, TNBC usually accepts chemotherapy rather than endocrine therapy or trastuzumab.4 However, a sensitive and specific non-invasive biomarker to detect clinical prognosis of TNBC is needed.
MicroRNAs (miRNAs), endogenous RNAs with about 23 nucleotides, regulate protein expression by paring with mRNAs of protein-coding genes and guiding their post-transcriptional repression.4 Deviated expression of the microRNA-34 (miR-34) family has been reported to play an important role in the pathogenesis of many cancers.5 Expression analysis of miR-34 family has suggested that its members play critical roles in many aspects of cancer biology, including invasion, metastasis, proliferation, cell survival, apoptosis, cell growth, cell cycle, migration, senescence, angiogenesis, and silencing, by regulating the expression of their target genes.567 However, most of these studies are tissue- and cell-based miR-34 family expressions. To exploit a noninvasive prognostic biomarker, the association between circulating miR-34 family expressions and clinical prognosis needs to be discovered.
This study aimed to investigate the association of circulating miR-34 family expression with clinicopathological features and their prognostic value in patients with TNBC.
MATERIALS AND METHODS
Patients
In this prospective cohort study, 173 TNBC patients admitted to First People's Hospital of Shunde from May 1, 2009 to April 30, 2013 were enrolled. All patients were diagnosed and assessed by clinical assessment, radiographic examination, and pathological confirmation through needle biopsy or during surgery. TNBC status was defined as ER negative (ER-) [below 10% staining by immunohistochemistry (IHC)], PR negative (PR-) (below 10% staining by IHC) and HER2 negative (HER2-) (0 or 1 by IHC defined as below 10% staining or slight and incomplete staining above 10% cells). Meanwhile, data of 75 age-matched healthy women volunteers were enrolled as healthy controls (HCs).
Peripheral blood samples were obtained from all TNBC patients before any treatments were performed, such as surgery, chemotherapy, and radiotherapy, and during the physical examination in HCs. After sampling, TNBC patients received appropriate treatments according to disease condition and clinical practice policy, and were followed up regularly until August 31, 2016. All clinical and pathological characteristics at baseline, as well as treatments post-sampling, were collected. This study was approved by the Ethics Committee of First People's Hospital of Shunde, and all participants provided written informed consent.
Sample acquisition and handling
An 8 mL aliquot of blood was obtained from all participants directly into sodium citrate tubes. The whole blood was allowed to stand for ~3 h at -4℃ before centrifuging at 1500 g for 10 min at room temperature. The resultant plasma was aliquoted into Eppendorf tubes and stored at -70℃.
RNA extraction
Total RNA was isolated with TRIzol (Invitrogen, Carlsbad, CA, USA) and purified by RNeasy mini kit (QIAGEN, Hilden, Germany) accordingly. Quality, quantity, and integrity of RNA was measured by a nanodrop spectrophotometer (ND-1000, Nanodrop Technologues, Wilmington, Delware, USA) and Ry gel electrophoresis, respectively. The total RNA was subsequently stored at -70℃ for further detection.
Quantitative reverse-transcription polymerase chain reaction (qRT-PCR)
To confirm the findings obtained by analyzing the miRNA profiling, we measured the expression of upregulated miRNAs using TaqManqRT-PCR. All reactions were carried out using Gene Amp PCR System 9700 (Applied Biosystems, Foster City, CA, USA). Briefly, the reverse transcription reaction was performed in a 20-µL mixture consisting of 0.3 µL of 10 µM RT primer, 100 ng RNA sample, 2 µL of 2.5 mM dNTPs, 0.2 µL MMLV reverse transcriptase, 2 µL of 10× reverse transcription buffer, 0.3 µL RNase inhibitor, and nuclease-free water. The reaction mixture was incubated for 30 min in 16℃, 40 min in 42℃, and 5 min in 85℃, and then kept in -20℃. Next, qPCR was performed in a final volume of 10 µL containing 1 µL PCR probe, 2 µL product from the RT reaction, 5 µL PCR Master Mix (2×), and 2 µL nuclease-free water. The thermal cycle started with 10 min at 95℃, followed by 40 cycles of 95℃ for 10 s and 60℃ for 1 min.
The threshold cycle (Ct) values obtained for each miRNA were then normalized to obtain ΔCt values and eventually used to plot relative expression values. Data are presented as mean±standard deviation, and miRNA values are presented as fold changes relative to controls. U6 was used as internal reference. The miRNA expression fold changes were calculated using the arithmetic formula 2-ΔΔ Ct.
Statistical analysis
Data were analyzed using SPSS software (version 20.0, SPSS, Inc., Chicago, IL, USA). Categorical variables were presented as counts and proportions, and were compared using chi-square test or Fisher's exact test. The Kaplan-Meier method and log-rank test was used to evaluate differences in survival according to miR-34 expression. Univariate and multivariate Cox proportional hazards regression analysis were used to identify risk factors for overall survival (OS). All statistical tests were two-sided, and p-value <0.05 was considered statistically significant.
RESULTS
miR-34 expression in TNBC patients and HCs
As demonstrated in Fig. 1, the expressions of miR-34a/b/c in plasma were significantly lower in TNBC patients, compared with HCs: miR-34a: 0.738 (0.533–1.141) vs. 1.197 (0.984–1.797), p<0.001; miR-34b: 0.980 (0.621–1.424) vs. 1.246 (0.780–1.611), p=0.027; miR-34c: 0.215 (0.143–0.384) vs. 0.390 (0.284–0.516), p<0.001.
Correlation of miR-34a/b/c expressions with clinical and pathological features
To reveal to correlation between miR-34a/b/c expression and clinicopathological characteristics, TNBC patients were divided into high (n=87) and low (n=86) expression groups by the median value of miR-34a/b/c. As shown in Table 1, miR-34a was correlated with tumor grade (p=0.038), lymph node positive (p=0.027), distant metastasis (p=0.004), and surgery (p=0.023); miR-34b was correlated with lymph node positive (p=0.027); and miR-34c was correlated with tumor grade (p=0.017) and distant metastasis (p<0.001). There were no other differences between clinicopathological features with miR-34a/b/c expression.
miR-34a/c low expressions were associated with worse prognosis
Next, Kaplan-Meier curve analysis was performed to demonstrate the correlation between miR-34 family expressions and OS. As shown in Fig. 2, patients with low expression of miR-34a (p=0.011) (Fig. 2A) and miR-34c (p=0.002) (Fig. 2C) had shorter OS than high expression group, while no differences were observed in miR-34b (p=0.138) (Fig. 2B).
miR-34c low expression was an independent factor for worse OS
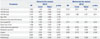
To better identify the impact of factors at baseline on prognosis, univariate Cox proportional hazards regression were performed, and all factors with a p value <0.1 were further analyzed by multivariate Cox's proportional hazards regression.
Univariate Cox's proportional hazards regression analysis indicated low expression of miR-34a (p=0.013) and miR-34c (p=0.003), tumor grade III (p=0.039), lymph positive (p=0.011), distant metastasis positive (p<0.001), and radiotherapy (p=0.010) and predicted worse OS, while surgery treatment could predict prolonged OS (p<0.001). Further multivariate Cox proportional hazards regression demonstrated only low expression of miR-34c (p=0.011), tumor grade (p=0.013), lymph positive (p=0.050), and distant metastasis positive (p=0.020) were independent risk factors for OS (Table 2).
Subgroup (TNM stage I–III patients and stage IV patients) analysis of prognosis
In TNM stage I–III subgroups (Table 3), tumor grade (p=0.016), lymph positive (p=0.016), and surgery treatment (p=0.001) were found to be correlated with OS by univariate Cox proportional hazards regression, while miR-34c low expression (p=0.035) and tumor grade (p=0.027) were independent risk factors for worse OS in multivariate analysis. In TNM stage IV subgroup (Table 4), miR-34a (p=0.029), miR-34b (p=0.020), and miR-34c (p=0.010) expressions were shown to be associated with shorter OS by univariate Cox proportional hazards regression, while no independent predictive factors for OS were found by multivariate analysis.
DISCUSSION
This publication was designed to study the relationship of circulating miR-34 family expressions with prognosis in TNBC patients and to evaluate its possibility of becoming a novel non-invasive prognostic biomarker. Our results demonstrated the expressions of miR-34a/34b/34c to be significantly decreased in TNBC patients. Moreover, low expressions of miR-34a and miR-34c indicated shorter OS, while miR-34c low level was an independent factor for worse prognosis.
Due to its specific receptor status, TNBC usually accepts chemotherapy rather than endocrine therapy or trastuzumab. There is no standard effective chemotherapy regimen for TNBC patients, which makes an biomarker to evaluate effectiveness of the therapy critical. Studies have demonstrated that miRNAs regulate many oncogenes, tumor suppressor genes, and dissemination and chemoresistance of tumors, which suggest that these miRNAs play critical roles in the pathogenesis of numerous cancers, including TNBC.89 Previous studies demonstrated the miR-34 family to be activated to transcript by high mutations rate of p53 gene production in TNBC patients,10 and involved in cancer cell proliferation, invasion, metastases, and apoptosis, as well as cell survival, cell cycle progression, cell senescence, cell migration, and angiogenesis.5 All these characteristics of the miR-34 family make it a promising biomarker of TNBC. Our study first focused on the relationship between circulating miR-34 family and prognosis in TNBC, which provided data for further development of novel noninvasive prognostic biomarkers.
Previous studies demonstrated the miR-34 family as tumor suppressive miRNA participating in the p53-driven apoptotic pathways.1011 However, the role of miR-34a in tumor suppression is controversial in previous reports. MiR-34a has also been pointed out as a potential tumor suppressor by inducing apoptosis in neuroblastoma cells.12 Controversially, overexpression of miR-34a has also been reported as an indicator of an aggressive breast tumor phenotype,13 and low expression of miR-34a suppressed breast cancer cells to proliferate.14 As for circulating miR-34a, a previous study showed it was significantly reduced in breast cancer without association with stage or grade of tumors.15 However, our results showed downregulation of miR-34a to be associated with worse tumor grade. Whether the differences in patient population (general breast cancer vs. TNBC) and sources of miR-34a (tissue vs. blood sample) led to these disparities deserves further investigation. As for the metastaticcondition, we found upregulation of miR-34a to be significantly correlated with non-metastatic condition in TNBC, which was similar with a previous report in breast cancer.16 Additionally, we also found miR-34a was related to lymph node status, and most importantly, was a risk factor of the OS in TNBC patients.
Our study revealed that miR-34c downregulation was correlated with tumor grade, metastasis, and was an independent risk factor of OS in TNBC patients. The mechanism of miR-34c involving in breast cancer by suppressing breast cancer migration and invasion by targeting GIT1 and Fra-1,1718 inducing G2/M cell cycle arrest in breast cancer cells.19 The down-regulation of miR-34c was induced by epithelial-mesenchymal transition and DNA methylation promoting self-renewal.20
In our study, there was no significant correlation between circulating expression of miR-34b and tumor status or OS in TBNC. However, in a study detected by formalin-fixed paraffin-embedded tissues from breast cancer, miR-34b, but not miR-34a/c, expression was reported to be negatively correlated with disease free survival and OS in TNBC patients.21 These diverse results might result from the different distribution of the deviated miR-34b in breast cancer tissues and blood samples, and further investigation is needed.
In conclusion, this study demonstrated that reduced miR-34a/c expression is highly associated with tumor progression and indicated worse prognosis and that miR-34c was an independent risk factor for OS in TNBC patients.





 XML Download
XML Download