

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Early repolarization (ER) is generally defined as a J point elevation of at least 0.1 mV above the baseline level on a standard 12-lead electrocardiography (ECG). ER has been considered as a normal variant, because it was generally known to be associated with younger age, athletes, or healthy individuals without structural heart diseases.1 However, recent studies have reported that an ER pattern in the inferior leads is related to death from cardiac causes in subjects without structural heart disease.234 Previously, we described the prevalence and prognostic significance of an ER pattern in variant angina patients.5 Variant angina is a transient myocardial ischemia caused by coronary arterial spasm and can be associated with fatal arrhythmias and sudden cardiac death.6 In a similar way, myocardial bridging (MB) arises when epicardial coronary arteries exist at intra-myocardium, bringing about systolic compression of the coronary arteries and transient myocardial ischemia. MB is observed during coronary angiography in less than five percent of coronary arteries that are otherwise angiographically normal and do not constitute a hazard.7 Occasionally, compression of a portion of a coronary artery by a MB can be related to clinical symptoms and signs of myocardial ischemia during strenuous physical activities, and may even result in myocardial infarction or initiation of a malignant ventricular arrhythmia.7 We, therefore, hypothesized that the presence of MB may be associated with ER. The aim of this study was to investigate the prevalence and prognosis of MB in subjects with ER.
MATERIALS AND METHODS
Study population
We enrolled 9870 patients who underwent coronary angiography at Severance Hospital in Seoul, Korea from January 2011 to December 2013. To investigate the association between ER and fatal arrhythmia, patients with other known disease related with fatal arrhythmia were differentiated from patients with idiopathic ventricular tachycardia (VT) or ventricular fibrillation (VF). Therefore, 8563 patients, who had known structural heart diseases, such as coronary artery occlusive disease,8 cardiomyopathies, moderate to severe valvular heart diseases, heart failure, and channelopathies, including long QT syndrome, Brugada syndrome,9 and catecholaminergic arrhythmia, were excluded from this study. We also excluded 388 patients who met the diagnostic criteria of vasopastic angina (VA).510 Following these exclusion criteria, the study population consisted of 1303 consecutive patients. The study was approved by the Institutional Review Board of Severance Cardiovascular Hospital, Seoul, Korea, and complied with the Declaration of Helsinki.
Coronary angiography
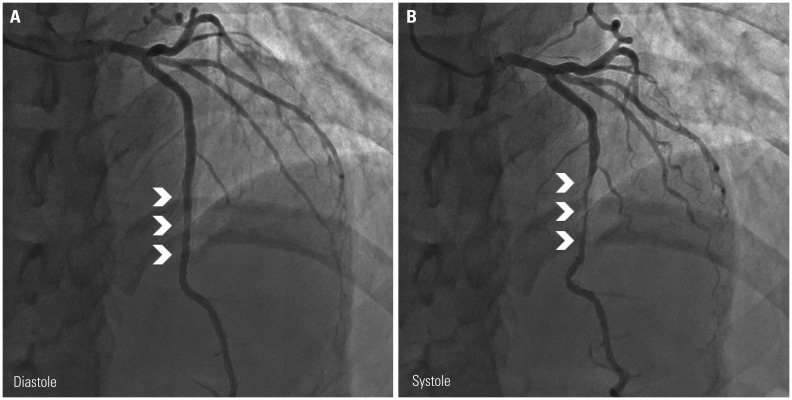
All 1303 patients underwent coronary angiography for evaluation of chest pain (n=1252, 96%), sudden collapse without documented ECG (n=11, 0.8%), pre-operative condition (n=7, 0.5%), or malignant ventricular arrhythmia (n=33, 2.5%). We diagnosed MB upon detection of milking or squeezing of the artery on coronary angiography. Fig. 1 shows a typical angiographic finding of MB during diastole (Fig. 1A) and systole (Fig. 1B). Each angiography positive for MB was classified according to the segment of the coronary artery, such as proximal/mid/distal left anterior descending coronary artery (LAD). We also categorized the severity of MB by the degree of luminal narrowing of the coronary artery. Mild, moderate, and severe MB were each defined as <50%, 50–75%, or >75% narrowing, respectively, compared with proximal and distal reference diameters of the milking area.11
Electrocardiography analysis
In all study subjects, ECGs were performed on the same day as coronary angiography. Standard 12-lead ECGs were downloaded digitally from the GE Marquette MUSE system (GE Medical Systems, Milwaukee, WI, USA). We checked the presence of left ventricular hypertrophy (Sokolow-Lyon criteria) and manually measured the QT interval corrected for heart rate (QTc) intervals (Bazett’s formula). Two experienced cardiologists without any information about patients and grouping were independently re-assessed in all ECGs. Substantial interobserver agreement was achieved for evaluation of ER and MB (kappa value, 0.86).12 An ER pattern was defined if all of the following three criteria were fulfilled:13 1) There was an end-QRS notch or a slur on the downslope of a prominent R-wave; the entire notch and onset of a slur should lie above the baseline; 2) J point elevation was >0.1 mV in two or more contiguous leads of the 12-lead ECG, excluding leads V1 to V3; and 3) absence of a widened QRS (QRS duration <120 ms). ER patterns were stratified according to the ST-segment. An ascending ST-segment was defined when the amplitude of the ST-segment 100 ms after the terminal portion of the J point (interval M) was greater than the amplitude at terminal portion of J point. If the amplitude of the ST-segment 100 ms after J point was less than or equal to the amplitude at J point, these patterns were defined as horizontal or descending ST-segment.1314
Fig. 2 show the ECG of notched and slurred ERs, respectively.
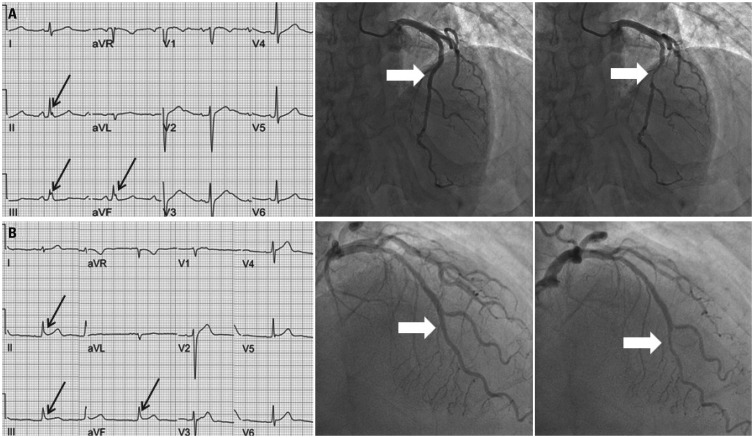
Fig. 2
The relationship between the location of MB and type of ER. (A) ECG of another sudden cardiac death patient who had prominent notched J point elevation (black arrows) and MB in the mid LAD (white arrows). (B) Early repolarization in a 29-year-old female patient, who had aborted sudden cardiac death caused by ventricular fibrillation. An ECG shows the prominent slurred J point elevation (black arrows) and MB in the distal LAD (white arrows). MB, myocardial bridging; ER, early repolarization; ECG, electrocardiography; LAD, left anterior descending coronary artery.
![]()
Statistical analysis
All continuous data are presented as mean±SD, and categorical data are reported as numbers and percentages in each group. Student’s t-test and chi-square test were performed to compare continuous and categorical variables. A multivariate analysis were conducted including age, sex, body mass index, pulse rate, presence of left ventricular hypertrophy, QRS, and QTc durations. A 1:1 propensity score matching by age and sex was performed for comparison of QTc intervals between the ER pattern group and no ER pattern group. SPSS statistical package (version 20.0, SSPS Inc., Chicago, IL, USA) and SAS (version 9.2, SAS Inc., Cary, NC, USA) were used to perform all statistical evaluations. All p-values less than 0.05 were considered statistically significant.
RESULTS
Prevalence of myocardial bridging
Of the 1303 patients who had undergone coronary angiography, ER was observed in 142 (11%) patients. Table 1 lists the baseline characteristics of the study population. Subjects with ER were more often men (70% vs. 48%, p=0.001), younger (59±13 years vs. 61±11 years, p=0.04), and had shorter QTc intervals (424±22 ms vs. 428±24 ms, p=0.049) and PR intervals (162±21 ms vs. 167±27 ms, p=0.04) on ECG than those without ER. However, after propensity score matching by age and sex, there was no difference in PR (164±21 ms vs. 168±21 ms, p=0.122) and QTc intervals (424±21 ms vs. 424±25 ms, p=0.853) between matched patients with ER (n=140) and no ER (n=140). The average heart rate of the 142 patients with ER pattern was 67±14, and the 1161 patients with no ER pattern had a heart rate of 69±13 (p=0.096). There was no difference in the usage of medications. Interestingly, MB was observed in 54 (37.6%) and 196 (16.8%) patients in the ER and no ER groups (p<0.001), respectively. Among patients with MB, 165 patients (66%) had chest pain caused by MB, and were treated with calcium channel blockers or beta blockers. Forty three patients (17%) had chest pain related with MB, and visited an outpatient clinic without prescription of medications. Ten patients (4%) were diagnosed with gastric ulcer or gastroesophageal reflux disease, and four patients (1.6%) had an anxiety disorder with or without panic disorder. Comparisons of baseline characteristics between patients with MB and without MB are presented in Supplementary Table 1, only online.
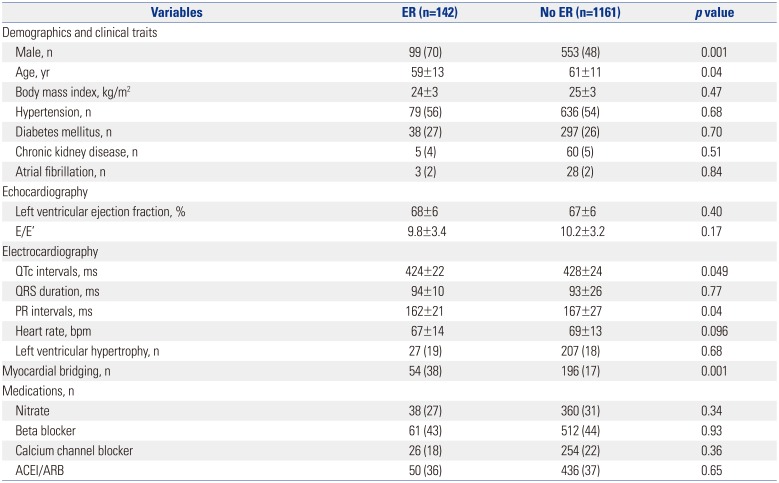
Table 1
Comparison of Baseline Characteristics between Patients with ER and those with No ER
![]()
Exercise stress test and imaging studies
Exercise stress test for chest pain was performed in 673 (52%, 158 MB and 515 no-MB subjects) patients. A positive result on the exercise stress test was observed in 59 (37%) and 134 (26%) patients in the MB and no MB groups, respectively. Myocardial ischemia was more common in the MB than the no MB group (p=0.006, Supplementary Table 2, only online). Ninety eight patients underwent single photon emission computed tomography (SPECT; n=93) or cardiac MRI (n=5). Reversible perfusion defect was observed in four out of 16 (25%) MB patients and in 12 out of 82 (14%) no MB patients (p=0.29).
Myocardial bridging as a predictor of ER
In univariate analysis, positive risk factors of ER were MB [odd ratio: 3.03, 95% confidence interval (CI): 2.08–4.40, p<0.001] and male sex (odd ratio: 2.5, 95% CI: 1.72–3.65, p<0.001). Negative risk factors were age (OR: 0.98, 95% CI: 0.97–0.99, p=0.03). In multivariate analysis, ER was independently associated with MB (odd ratio: 2.9, 95% CI: 1.98–4.24, p<0.001) and male sex (odd ratio: 2.4, 95% CI: 1.66–3.59, p<0.001) (Table 2).

Table 2
Uni and Multivariate Analysis of Factors to Influence ER
![]()
Cardiac events
Table 3 shows the comparison of cardiac events, including cardiac death or fatal arrhythmia (including VF and/or VT), between ER and no ER patients. During a median follow-up period of 37 months, cardiac events occurred in nine (6.3%) and 22 (1.9%) subjects with and without ER, respectively (p=0.001). Arrhythmic events were observed in seven (4.9%) and 20 (1.7%) patients in ER and no ER groups, respectively. Out of 31 cardiac events, four (13%) were sudden cardiac deaths. Among patients with sudden death or fatal arrhythmic events, MB was observed in two out of nine (22%) patients with ER and no patients without ER (n=22). There was a tendency of more frequent MB in the ER group than no ER group without statistical significance. VF and VT were the most commonly documented initial arrhythmias in both groups. Cardiac events occurred during sleep in two (1.5%) and four (0.3%) patients with ER and no ER, respectively. Five (42%) patients had a VF during the day (AM 08:00–PM 22:00) and seven (58%) patients had a VF during the night (PM 22:00–AM 08:00). All 4 patients with ER and three out of 8 patients without ER had a VF during the night (p=0.081).
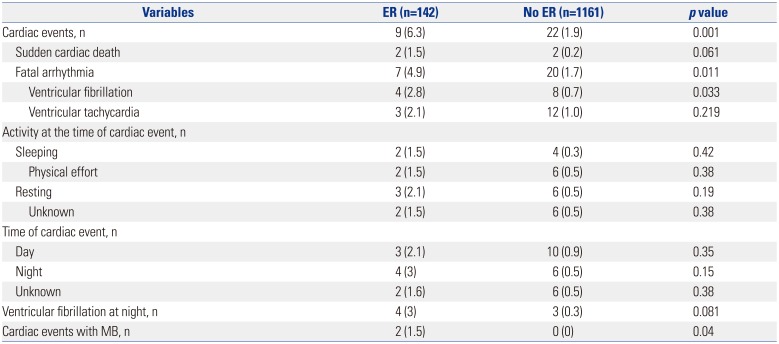
Table 3
Comparison of the Cardiac Events, Documented ECGs and Characteristics of Cardiac Events between Patients with ER and those without ER
![]()
In subgroup analysis of 44 patients with syncope and/or malignant arrhythmia, 4 patients had MB and ER, 8 patients had only ER, 2 patients had only MB, and 30 patients did not have MB or ER. In this subgroup, MB is more prevalent in the ER group (4/12, 33%) than the no ER group (2/32, 6%) with p-value of 0.039. Supplementary Table 3, only online shows the comparison between patients with and without syncope and/or malignant ventricular arrhythmias.
Difference of ER ST-segment pattern according to MB
Table 4 shows ER ST-segment patterns between patients with MB and those without MB. There was no difference in types of ST-segment elevation, amplitude of J point elevation, and location and types of ER pattern. Among all 54 (21%) MB subjects with ER, the type of J point was notched in 34 (62%) and slurred in 20 (38%). MB involved the mid LAD in 44 (81%) patients and distal LAD in only 10 (19%) patients. Interestingly, notched type ER was more frequently observed in MB involving the mid portion of the LAD (70% vs. 30%, p=0.03) (Table 5). Fig. 2 shows notched and slurred types of ER in MB involving the mid LAD and distal LAD, respectively. However, there was no significant difference in cardiac events regardless of whether ER with MB involved the mid LAD or not.
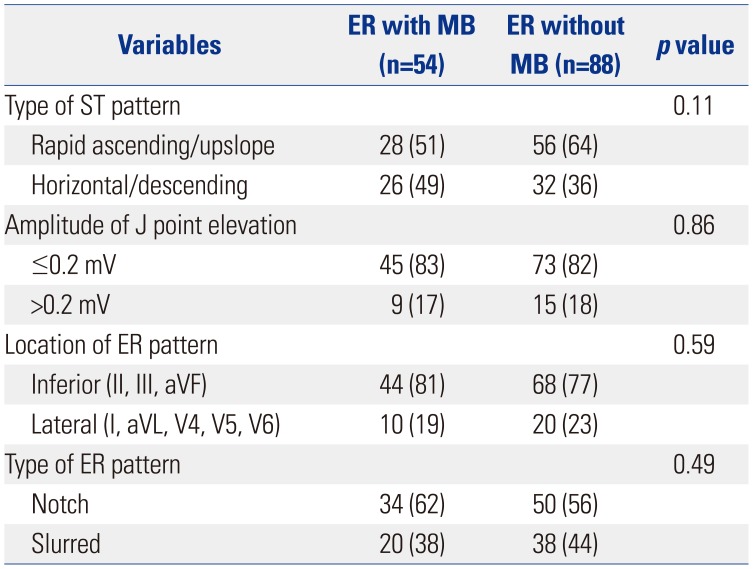
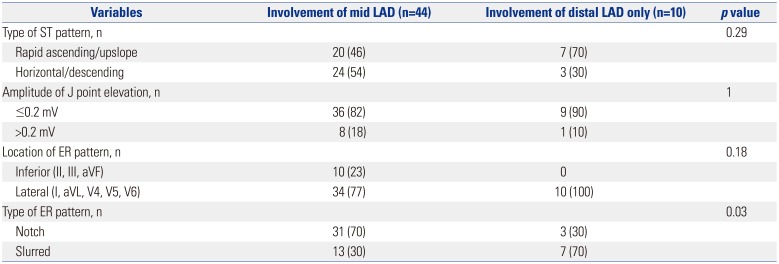
Table 4
Difference of ER ST-Segment Pattern According to MB
![]()
Table 5
Difference of ER Characteristics Depending on MB Location
![]()
DISCUSSION
Major findings
The main finding of this study was that MB was twice more frequently observed in subjects with ER than those without ER patterns. Even after adjusting for other risk factors, MB was an independent risk factor of ER. Second, the presence of MB did not change the rate of cardiac events. Finally, the notched type ER was associated with MB involving the mid LAD, but not the distal LAD. This study suggests that ER might be associated with MB, and the prognosis is benign in this situation.
Early repolarization and myocardial bridging
ER was observed in 22% of MB patients. The reason why ER was frequently observed in patient with MB might be explained by the fact that MB produced ischemia.715 Direct MB compression of the LAD at cardiac systole was previously found to result in delayed arterial relaxation at diastole, reduced blood flow reserve, and decreased coronary blood perfusion.15 Previous studies also showed ECG changes caused by myocardial ischemia, resulting from the compression of coronary artery.1617 Also, it was reported that the ECG manifestation and arrhythmogenic pathophysiology of early phase ischemia were similar to that in J wave syndrome.18 Myocardial ischemia reduces inward currents (principally INa and ICa), increases outward potassium currents by opening KATP channels, and intensifies Ito, especially in the epicardium. Blocking the INa current, KATP opening, and the Ito current generates J waves in both genetically proven channelopathies and in experimental drug-induced models.19 Consistently, myocardial ischemia was more common in MB patients during a treadmill stress test in our study. Also, Gawor, et al.20 reported that 43% of MB subjects with >50% systolic constriction at angiography had stress-induced ischemia on SPECT. Although the number of subjects was too small to have clinical significance in our study, a higher rate of reversible perfusion defect was observed in MB subjects than those without MB. Another potential explanation of ER in MB patients is that MB can lead to irreversible myocardial damage. MB produces not only myocardial ischemia but also may even result in myocardial infarction.1521 And a high incidence of ER was reported in patients with healed myocardial infarction.8 Finally, MB induced endothelial injury arising from abnormal hemodynamics provoked by retrograde blood flow toward the left coronary ostium at cardiac systole,715 resulting in the formation of several atherosclerotic lesions.7
Since we analyzed patients who had undergone coronary angiography for various reasons, mostly chest pain (96%), a higher prevalence of MB was observed in this study, compared with previous studies (17% vs. 5%).722 Also, the fact that a number of symptomatic MB patients were included in this study is why the persistent ER pattern could be observed frequently.
Cardiac events
Our results showed that MB may induce coronary ischemia, resulting in an ER pattern, although it does not significantly influence a cardiac event. Among the entire study population, only three MB patients experienced a cardiac event. This number of cardiac events in the MB group was too small to reach a conclusion. Another potential explanation for this result is a different rate of beta blocker usage. Subjects with ER and MB had a higher rate of previous beta blocker usage (27/54, 50%) than subjects with ER and no MB (35/88, 39%). Despite the absence of statistical significance due to the small numbers of both groups (p=0.233), the preventive effect of beta blocker to malignant ventricular arrhythmia could influence the results of cardiac events.
The site of MB and characteristics of ER
In this study, notched type of ER was more frequently observed in MB involving the mid portion of the LAD. A prominent Ito-mediated action potential notch in ventricular epicardium produces a transmural voltage gradient during early ventricular repolarization that registers as a J wave.23 The degree of accentuation of action potential notch depends on the magnitude of Ito, and increased voltage gradient across the ventricular wall results in a J wave.24 The presence of an intensive magnitude of Ito and dispersion of repolarization can induce a Phase 2 reentry and VT/VF. Therefore, patients with ER might involve arrhythmogenic potential and consequently, may be more susceptible to myocardial ischemia caused by MB. In addition, the more proximal the MB is located to the left coronary ostium, the more turbulent the blood flow becomes in the LAD segment proximal to the MB.25 It was reported that intimal thickness beneath MB is remarkably thin in contrast with various atherosclerotic lesions in the intima both proximal to MB.2627 These results may be associated with higher transmural gradient and electric heterogeneity between the epicardium and endocardium, which makes notched type J wave easily, in MB located in the proximal LAD than those of the distal LAD.
Recently, it was reported that tachycardia-dependent augmentation of notched type J wave must be explained by conduction delay or phase 3 block.1428 This type of ER can be observed in J waves of individuals in which idiopathic VF or sudden cardiac death is unlikely.28 Although it is a consensus that the pattern of end-QRS notching and slurring may be due to late depolarization rather than ER,13 the mechanism of J wave has not yet been completely established.
Study limitations
This study had some limitations. First, since the number of events is too small in the groups, we could not sufficiently investigate the effects of MB in ER in this study. A study with a larger number of MB patients is needed. Second, we selected patients who had undergone coronary angiography for various reasons, such as chest pain, pre-operative evaluation, or malignant ventricular arrhythmia, which explains why both group had high incidence of MB and sudden cardiac death. Third, too small number of subjects underwent cardiac MRI or SPECT to detect myocardial ischemia which might help explain the cause of ER in patients with MB. Fourth, although we excluded 388 patients who met the diagnostic criteria of VA, we could not completely exclude vasospastic angina patients. Therefore, ER in the cases of bridged LAD may be related to coronary spasm in some patients. Finally, we could not find the ECG before ER in most patients; therefore, we could not determine with definite certainty whether the probability of patients with ER facing an adverse event was changed because of MB or if MB was a potential cause of selection bias that led patients with ER to the doctors’ attention.
In conclusion, MB was independently associated with ER in patients without out structural heart disease who underwent coronary angiography. Notched type ER was closely related with MB involving the mid portion of the LAD. Among patients who had experienced cardiac events, a higher prevalence of MB was observed in patients with ER than those without ER. Further prospective studies on the prognosis of MB in ER patients are required.
 XML Download
XML Download