

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of asthma in the United States has increased significantly over the last decade, and an estimated 24 million persons in the US were diagnosed with asthma in 2014.12 Asthma increases medical costs and may be associated with activity limitations, inability to work, increased number of sick days, and unemployment.34 The total incremental cost of asthma is estimated at $67–$75 billion (2015 dollars).56 Prescription drugs represent the biggest component of asthma medical costs, and job loss is estimated to account for 61% of the indirect costs attributable to asthma.7 Estimated missed work days attributable to asthma have been associated with an estimated $301 for each worker per year (2015 dollars).5
Obese individuals incur substantially greater medical costs, compared to normal-weight persons;89 per capita healthcare costs attributable to obesity are estimated at $1889–$4380 (2015 dollars), which is significantly higher than costs incurred by normal weight individuals.1011 Furthermore, obesity also significantly increases absenteeism costs,12 and concurrent obesity exacerbates the impact of chronic diseases on medical expenditures, missed work days, and lost productivity.13
Body mass index (BMI) has been shown to be negatively associated with various lung volume measures, and obesity has been correlated with lower lung function and more comorbidities among asthma patients.14 Increasing BMI has been found to be significantly associated with worsening asthma severity,15 greater asthma symptoms, poorer asthma control,1617 more activity limitations, worse general physical health status, more missed workdays, and more medication use and hospitalization.151819 Compared to normal-weight patients with asthma, overweight or obese patients tend to have more asthma-related hospitalizations, more emergency department visits, and more unscheduled urgent care visits, regularly scheduled visits, and follow-up visits for an asthma episode.1920 Studies conducted among non-elderly and elderly asthma patient cohorts have demonstrated a significant impact of obesity on healthcare costs.1021
Although previous studies have consistently shown the significant economic impact of asthma or obesity on medical costs and lost productivity, the total incremental costs of obesity among patients with asthma have not been estimated. The objective of this study was to estimate the annual health care and productivity loss costs attributable to overweight or obesity in working asthma patients in the US from 2003 to 2013 using the Medical Expenditures Panel Survey (MEPS).
MATERIALS AND METHODS
Data source
The data source for this study was the 2003–2013 MEPS, which has been conducted annually since 1996 under the sponsorship of the Agency for Healthcare Research and Quality and the National Center for Health Statistics.22 The MEPS survey provides nationally representative estimates of health care use, expenditures, sources of payment, and health insurance coverage for the US civilian non-institutionalized population. The panel design of the survey, comprising five rounds of interviews covering two full calendar years, allows for the examination of person-level changes in expenditures, health insurance coverage, and health status. Eight years of pooled MEPS-HC data were merged with the full-year consolidated file using unique identifiers to ensure sufficient sample size and produce estimates with high reliability.22 For the pooled analysis, survey weights provided by MEPS were used to generate nationally representative results.
Study population
Patients with an asthma diagnosis were identified using International Classification of Diseases, 9th Revision (ICD-9) codes (493.xx), the Clinical Classification Code (CCC) (128), or a MEPS self-report of asthma. To estimate productivity loss costs, the study population was limited to working patients aged 18 to 64 years, who were selected if they answered yes to the question "are you currently employed or employed" during the reference period (i.e., time period between the date of the previous round's interview and the date of the current round's interview)" at least once for the employment status question in each round. Exclusion criteria included a diagnosis of malignancy (ICD-9 code: 140–239, CCC: 011–045, or if they answered "yes" to "Have you ever been diagnosed as having cancer or a malignancy of any kind?"), pregnancy (ICD-9 code: 633–650 or CCC: 177–196), kidney dialysis (ICD-9 code: V56 or CCC: 158), human immunodeficiency virus (ICD-9 code: 042, 043, 996, V08, V42, V43, V49, or CCC: 005), or BMI <18.5 kg/m2.
Study outcomes
Study outcomes included treatment costs and productivity loss costs. All-cause health care costs were derived from the sum of expenditures associated with medical services (e.g., hospitalizations, office-based/outpatient visits, and emergency department visits) and prescription drugs. These expenditures in MEPS were defined as the sum of the direct payments for care provided during the year, including out-of-pocket payments and payments through private insurance, Medicaid, Medicare, and other sources. Payments for over-the-counter drugs and alternative care services were excluded.22
Productivity loss costs were estimated based on missed work days due to illness, injury, or mental or emotional problems during the reference period, and were valued using the average hourly wage by occupation, obtained from the Unites States Bureau of Labor Statistics in 2015.23 Since the number of work days lost were provided in MEPS as ≥0.5 days, we could not distinguish half versus full days missed; one missed day was considered to be 6 hours, consistent with previous studies using MEPS.24 Annual missed work days were calculated using the reference period (the period of time during which the data for each person were collected).
Study variables
To examine the impact of overweight and obesity on costs, asthma patients were classified into three groups based on BMI calculated using self-reported height and weight from MEPS: normal (18.5 kg/m2 ≤BMI <25 kg/m2), overweight (25 kg/m2 ≤BMI <30 kg/m2), and obese (BMI ≥30 kg/m2).2526 Self-reported patient characteristics were also evaluated to adjust for factors that may potentially confound the association between BMI status and study outcomes, including patient age, gender, race/ethnicity, insurance status, smoking status, marital status, income, and occupation. Insurance status was categorized into public, private, both public and private, or uninsured types. Smoking status was categorized into former/never smoker and current smoker types.
Comorbidities included the following: cardiovascular disease [ICD-9-CM code: 410–417, 428, 429, 798; CCC: 101–104, 108; or if they answered "yes" to "Have you ever been diagnosed as having heart disease (coronary heart disease, angina, angina pectoris, heart attack, myocardial infarction, or any other kind of heart disease or condition)?"]; cerebrovascular disease (ICD-9-CM code: 430–438, CCC: 109–113, or if they answered "yes" to "Have you ever been diagnosed as having had a stroke or transient ischemic attack?"); hypertension (ICD-9-CM code: 401–405, CCC: 98–99, or if they answered "yes" to "Have you ever been diagnosed as having high blood pressure?"); diabetes (ICD-9-CM code: 250, CCC: 49–50, or if they answered "yes" to "Have you ever been diagnosed with diabetes?"); hyperlipidemia (ICD-9-CM code: 272, 440, 445; CCC: 53, 114, 116; or if they answered "yes" to "Have you ever been diagnosed as having high cholesterol?"); mental disorder (ICD-9-CM code: 295, 296, 300, 311; CCC: 657, 659, 670; or if they answered "yes" to "Have you ever been diagnosed as having attention deficit hyperactivity disorder or attention deficit disorder?"); and a respiratory disease other than asthma (ICD-9-CM code: 460–492, 494–516; CCC: 122–127, 134; or if they answered "yes" to "Have you ever been diagnosed as having emphysema or chronic bronchitis?").
Statistical analysis
Differences in demographic and clinical characteristics stratified by BMI category were compared using the chi-squared test and analysis of variance test. Unadjusted average all-cause annual medical costs and productivity loss costs were calculated, and a 95% confidence interval (CI) was obtained using bootstrap methods with 1000 iterations, since these costs did not follow a normal distribution.527
A generalized linear model (GLM) with log link function and a gamma distribution was used to identify the significant factors associated with medical costs in asthma patients and to estimate regression coefficients.352829 The dependent variable in the model was patient BMI, classified as either overweight, obese or normal-weight, and independent variables included age, gender, race/ethnicity, insurance status, marital status, income, and comorbidities. To estimate health care costs attributable to overweight or obesity, the recycled prediction method was used.29303132 Using the calculated coefficients of the study covariates, costs were estimated by assuming that everybody was obese (i.e., by treating the indicator variable as equal to 1), and then re-estimated by assuming that everybody was normal (i.e., by treating the indicator variable as equal to 0). The mean difference between the two estimated costs was calculated to reflect the costs attributable to obesity in asthma patients. The same process was used to estimate the medical costs attributable to overweight in asthma patients.
Productivity loss costs were calculated using the two-part model
since many patients incurred zero productivity loss costs.53033 In the first part of the two-part model, a logistic model was used to predict the probability of any costs, and in the second part, a GLM with a log link function and a gamma distribution was used to predict productivity loss costs for positive costs only. In both models, costs were estimated adjusting for age, gender, race/ethnicity, insurance status, marital status, income, occupation, and comorbidities. Productivity loss costs attributable to overweight or obesity in asthma patients were estimated using the same methodology as for medical costs described above.
For all analyses, MEPS sampling and variance adjustment weights were considered to reflect the survey design structure for the estimation of national representative values. All costs were converted to 2015 US dollars using the consumer price index (CPI).34 Data were analyzed using SAS 9.2 (SAS Institute, Cary, NC, USA) and STATA 10.1 (STATA Corporation, College Station, TX, USA).
RESULTS
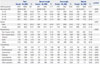
Among 381682 subjects in MEPS from 2003 to 2013, 11670 workers were identified as asthma patients aged 18 to 64 years based on study selection criteria. Of these patients, 3761 (33.0%) were overweight, and 4428 (35.2%) were obese. Demographic characteristics of asthma patients stratified by BMI category are shown in Table 1. Obese patients with asthma were significantly more likely to be older, female, and non-Hispanic white. Obese patients with asthma were more likely to have cardiovascular disease, hypertension, hyperlipidemia, and other respiratory disease as comorbidities.
Obese patients with asthma incurred significantly higher annual medical costs across all service categories than normal-weight and overweight asthma patients (Table 2). An unadjusted average annual medical costs for obese patients with asthma were $5412 (95% CI: $4899–$5817) per patient, 40% higher than overweight patients ($3873; 95% CI: $3395–$4226) and 60% higher than normal-weight patients ($3385; 95% CI: $2527–$4191). Furthermore, regardless of BMI category, outpatient visits accounted for the highest proportion of treatment costs, followed by prescription drugs, inpatient visits, and ED visits.
Obese patients with asthma also had higher productivity loss costs than overweight or normal-weight patients (Table 2). The unadjusted average annual productivity loss costs for obese patients were $745 (95% CI: $664–$826) per patient, 72% higher than those of overweight ($434; 95% CI: $381–$487) and over two times those of normal weight ($353; 95% CI: $312–$393). The increasing productivity loss costs by BMI category resulted from the increasing effect of BMI on missed work days. Total missed work days averaged 2.7 (95% CI: 2.4–3.0) in normal-weight patients, 3.3 days (95% CI: 2.9–3.7) in overweight patients, and 5.6 days (95% CI: 5.0–6.3) in obese patients. Obese and overweight patients experienced an additional mean of 2.9 and 0.6 days lost from work per year, respectively, compared to normal-weight patients.
Average annual medical costs for working asthma patients increased with patient age (Fig. 1), and the increasing effect of BMI on average annual medical costs was consistent across all age groups. Average annual productivity loss costs increased for the 41 to 50 years age group but declined for the 51 to 64 years age group, suggesting a lower labor force participation rate in the latter age group among the general population (Fig. 2).
Annual total treatment costs for working asthma patients increased significantly when patients were obese, older, female, or had comorbid cardiovascular disease, hypertension, or hyperlipidemia (Table 3). Obese patients with asthma had significantly higher treatment costs (cost ratio: 1.20; 95% CI: 1.04–1.39) than normal-weight patients after adjusting for the study variables. Obese patients with asthma had productivity loss costs 46% higher (cost ratio: 1.46; 95% CI: 1.24–1.72) than those of normal-weight patients after adjusting for the study variables.
Fig. 3 depicts the treatment costs and productivity loss costs attributable to obesity and overweight in working asthma patients. The average total costs attributable to obesity were $1103 (95% CI: $1085–$1122), nearly four times the costs attributable to overweight (mean: $280; 95% CI: $274–$286).
DISCUSSION
In this study, we estimated that 68.2% of asthma patients were overweight or obese, which is comparable to the age-adjusted prevalence of overweight and obesity (68%) in the general US adult population.25 Mean annual all-cause health care costs for obese asthma patients were $5412 per patient, 40% higher than those for overweight ($3873) and 60% higher than those for normal weight ($3385) patients. Furthermore, mean annual productivity loss costs of obese asthma patients were $745 per patient, 72% higher than those of overweight ($434) and over two times those of normal weight ($353) patients. Health care costs attributable to obesity and overweight in working asthma patients were estimated to be $878 and $257 per person per year, respectively, and productivity loss costs attributable to obesity and overweight among working asthma patients were $256 and $26 per person per year, respectively.
In the current study, mean annual all-cause health care costs for asthma patients were $4260 per patient. Of these treatment costs, in our estimation, outpatient visits and prescription drugs were the largest components, accounting for 40.6% and 32.0% of total treatment costs, respectively. Previous studies have estimated the annual incremental health care costs associated with asthma: estimates per person range from $2340 (2015 US dollars) to $9337 (2015 US dollars) in adults and $3876 (2015 US dollars) in both adults and children.34535 Kamble and Bharmal3 also reported that prescription medications and physician office visits were the major drivers of total asthma-related expenditures, constituting 49% of the total incremental costs of asthma in adults. Similarly, Sullivan, et al.4 found that prescription drugs represented the largest contributor to all-cause health care expenditures for asthma patients, followed by hospitalization. While these previous studies provided valuable insight into the economic burden of asthma, they did not account for the possibility that the BMI status of asthma patients can also influence the direct medical costs associated with asthma.
We estimated the direct and indirect costs attributable to overweight and obesity in patients with asthma at $280 and $1103 (in 2015 dollars), respectively, suggesting that excessive weight in asthma patients can have an incrementally substantial economic consequence on asthma treatment costs. While the total incremental cost of overweight/obesity among patients with asthma has not previously been studied, Sarpong10 estimated that if younger adult obese patients with asthma were normal weight, total all-cause healthcare expenditures (including prescription medications) would be expected to be decreased by $2066 (2015 US dollars) and $4378 (2015 US dollars) respectively. The incremental cost of obesity among older adult asthmatic patients was estimated at $6204 (2015 US dollars) in all-cause health care costs.21
In addition to direct medical costs, asthma patients suffered productivity loss at the rate of four missed work days per year per patient on average, and these costs increased with increasing BMI. The average productivity loss cost for obese patients with asthma was estimated at $745 per patient per year, more than twice the cost of productivity loss for normal-weight asthma patients ($434). Our estimates of productivity loss costs, even for normal-weight patients, were greater than was the estimate ($353) of the value of additional days lost due to asthma calculated by Barnett and Nurmagambetov5 Moreover, our estimates of incremental productivity loss costs for obesity ($256) relative to normal weight were greater than the costs of absenteeism associated with obesity and morbid obesity estimated by Cawley, et al.,12 which were $152 (2015 dollars) and $314 (2015 dollars) per worker, respectively, regardless of disease.
Although this study found that concurrent obesity in asthma patients had a strongly negative impact on productivity loss, further research is needed to examine how the incremental negative consequences of obesity on productivity among asthma patients compare to the other segments of the population. Our findings suggest that the benefits of weight reduction in asthma patients could be substantial, especially when the effort is focused on those with higher BMI. In fact, it is well-documented that weight reduction can offer potential clinical benefits to asthma management.36 Weight reduction among obese patients with asthma through low-calorie dieting was associated with a reduction in airway obstruction and peak expiratory flow variability in one study.37 Another randomized weight reduction program among obese people with asthma improved lung function variables such as forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) and the improved lung function was sustained even after the program ended.38 Additionally, the weight reduction was shown to be beneficial in reducing the number of asthma symptoms that obese asthmatic people experienced and improving physical activities that had previously been limited by breathlessness.
While our study provides valuable information on the total incremental cost of obesity in asthma using advanced estimation methods that have not previously been used, our findings must be interpreted in light of several study limitations. We examined the economic impact of comorbid obesity in asthma patients, but could not determine the causality between obesity and costs due to the cross-sectional nature of the study. Asthma patients were identified based on self-reported diagnosis or the Clinical Classification or ICD-9 code used by physicians rather than on confirmed diagnoses of asthma through pulmonary function tests. The unavailability of pulmonary function data also precluded the consideration of asthma severity in this study. In addition, this study may have underestimated the costs attributable to obesity or overweight in asthma patients, as we did not include caregiver time costs and mortality costs. Premature mortality associated with obesity can incur increased indirect costs to employers through increased life insurance premiums and to employees through lost earnings.39 Finally, the prevalence of obesity in asthma patients may have been underestimated since BMI was based on self-reported height and weight, as suggested by other studies.40
In conclusion, the direct and indirect costs attributable to overweight and obesity in patients with asthma are substantial. This study's findings highlight the importance of targeted public health interventions for obese patients with asthma to reduce the economic burden of asthma. Public health programs to promote weight reduction and weight management among obese and overweight patients with asthma may play an important role in curbing the economic burden of asthma.





 XML Download
XML Download