

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The growth of older adult populations has led to increases in the number of nursing home residents globally. In 30 years, about 40% of the adults worldwide will be staying in a nursing home or long-term care facility.1 In Korea, 12.7% of the population was older than 65 years in 2014 and this will reach about 14% in 2017.2 In 2009, there were 201226 patients using nursing hospitals and 80025 in nursing homes, and these numbers increased to 296728 and 132235 people, respectively, in 2012.3 Among the residents in long-term care facilities, the most common cause of hospitalization, morbidity, and mortality was pneumonia.4 Of potentially preventable diseases, pneumonia is the most common.5 Nursing home-acquired pneumonia (NHAP) is one form of healthcare-associated pneumonia (HCAP).6 In 2005, the American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) suggested that HCAP patients, including those with NHAP, should be treated with the same broad-spectrum antibiotics as hospital-acquired pneumonia to cover multidrug resistant (MDR) pathogens.6 However, treating NHAP and HCAP has been controversial, although the mortality rate of NHAP is higher than that of community-acquired pneumonia (CAP). The microbial distributions of NHAP vary among nations, regions, study designs, and disease severity.7 The British Thoracic Society guidelines for CAP in 2009 mentioned nursing home residents as a specific population group of CAP and did not recommend specific management for NHAP, in contrast to the 2005 ATS/IDSA guidelines.8 The nursing home setting has attributes that differ from those of other health care settings in terms of patient age, comorbidities, disease severity, functional status, realistic treatment goals, and aggressive disease monitoring.9 In addition, it is not clear whether the increased frequency of MDR pathogens leads to inappropriate antibiotic therapy and higher mortality.10 Therefore, we conducted this study to analyze factors contributing to the mortality rates of NHAP, in comparison to those for CAP, among elderly patients.
MATERIALS AND METHODS
Study design and patients
We retrospectively analyzed patients older than 65 years old admitted to a single teaching hospital (600 beds) in South Korea with either CAP or NHAP from January 2008 to December 2014. Categories of HCAP other than NHAP were excluded: hospitalization for 2 days or more in the preceding 90 days, long-term dialysis within 30 days of entering the study, immunocompromised status including AIDS, active malignancy receiving chemotherapy, history of solid-organ transplantation on immunosuppressive agents, or immunosuppressive therapy including 10 mg prednisone/day for at least 30 days or equivalent. The patients who had do-not-resuscitate (DNR) status were excluded. We analyzed medical records for baseline characteristics, orientation disturbance, functional status, the degree of aspiration, comorbidities, severity, pathogen, antibiotics, and clinical outcomes. This study was approved by the local Ethics Committees of the Institutional Review Board of the Dongguk University Hospital.
Definitions
The diagnosis of pneumonia was based on the following criteria: 1) new or persistent pulmonary infiltrate and 2) two or more symptoms and signs, including body temperature greater than 38.5℃ or less than 35.5℃, leukocyte count greater than 12000/mm3 or less than 4000/mm3, and purulent sputum. NHAP and CAP were divided according to ATS/IDSA guidelines.6 Pneumonia severity was evaluated using CURB-65 score, which consists of five variables: confusion of new onset, blood urea nitrogen greater than 7 mmoL/L (19 mg/dL), respiratory rate of 30 breaths per minute or greater, blood pressure less than 90 mm Hg systolic or diastolic blood pressure 60 mm Hg or less, and age of 65 years or older.11 Patients with poor functional status were defined as being bedridden or those who used a wheelchair. Probable aspiration was defined as any witnessed aspiration before hospital admission or aspiration confirmed by video associated swallowing test.12 Patients with tube feeding were defined as the administration of liquefied foods through a nasogastric tube or percutaneous endoscopic gastrostomy tube. Initial treatment failure was defined as death during initial antibiotics treatment or change of antibiotics from first agents to others after 48 hours due to clinical instability.12
Microbiological evaluation
Respiratory samples such as sputum, endotracheal suction and bronchoalveolar washing, blood cultures, urinary antigen test for Streptococcus pneumonia and Legionella species, were obtained and investigated. Standard serologic methods were used to determine antibodies against atypical agents, such as Mycoplasma pneumoniae. MDR pathogens included methicillin-resistant Staphylococcus aureus (MRSA), Pseudomonas aeruginosa, extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae, carbapenem resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia.613 Pseudomonas species were included as MDR pathogens regardless of the drug susceptibility test.
Clinical outcomes
The primary outcome was in-hospital mortality. Secondary outcomes were length of stay and intensive care unit (ICU) stay.
Statistical analysis
All statistical analysis was performed using Statistical Package for the Social Science ver. 12.0 (SPSS Inc., Chicago, IL, USA). Shapiro-Wilk's W test was performed for normality of the data. For inter-group comparisons, continuous variables were analyzed using Student's t-test, and when data were not normally distributed, the non-parametric Mann-Whitney U test was used. Descriptive variables were analyzed using chi-squared test or Fisher's exact test if more than 20% of the expected cell frequencies <5. Logistic regression analysis was used to assess the risk factors of mortality. Further, variables that were associated with in-hospital mortality at p values less than 0.1 in univariate analysis (age and sex) were included in multivariable logistic regression analysis. Assessment of the applicability of multicollinearity indicated no multicollinearity issues (tolerance >0.1 and variance inflation factor values <10) between the chosen independent variables in this study. p values less than 0.05 were considered statistically significant. The contribution of each potential risk factor was denoted by the odds ratio (OR) and associated 95% confidence interval (CI).
RESULTS
Patient characteristics
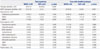
A total of 317 patients with pneumonia aged 65 years or more were analyzed. One hundred five patients had NHAP, and 212 patients had CAP. The baseline characteristics of the patients with NHAP and CAP are presented in Table 1. The median age of the patients with NHAP was 80 years, and that of patients with CAP was 75 years. NHAP patients had a lower body mass index (BMI), compared to CAP patients (p<0.001), and fewer current smokers (p=0.005). NHAP patients had a higher frequency of poor functional status (66.7% vs. 9.4%; p<0.001), confusion rate (68.6% vs. 10.4%; p<0.001), use of tube feeding (23.8% vs. 0.5%; p<0.001), and probable aspiration (48.6% vs. 13.2%; p<0.001) than CAP patients. The incidence of chronic respiratory disease, heart disease, diabetes mellitus, and chronic renal diseases were not different between the two groups. Patients with cerebrovascular disease (50.5% vs. 16.5%; p<0.001) and other neurologic disease (54.3% vs. 6.6%; p<0.001) were more frequent in NHAP patients than in CAP patients.
Initial clinical features and severity at presentation
The initial clinical characteristics and severity in the NHAP and CAP groups are shown in Table 2. The time from symptom to admission was shorter in NHAP patients, compared with CAP patients. CURB-65 was higher in NHAP patients than in CAP patients. NHAP patients had higher rates of mechanical ventilation (MV) use (21% vs. 9%; p=0.003) and ICU admission (47.6% vs. 18.4%; p<0.001) than CAP patients. Laboratory findings, such as C-reactive protein level or leukocytosis, revealed no differences between two groups, although NHAP patients had more severe pneumonia on chest X-ray, as defined by bilateral involvement of pneumonia, compared with the CAP patients.
Microbiology and initial antibiotics
The microbes identified in the NHAP and CAP groups are listed in Table 3. The numbers of both the total population and cases with any pathogen are shown in Table 3. The patients identified with causative pathogens accounted for 51.4% of NHAP and 29.2% of CAP cases. Streptococcus pneumoniae was the most frequent pathogen in both groups. MDR pathogens were isolated more frequently in NHAP patients than in CAP patients (21.9% vs. 1.4%; p<0.001). MDR pathogens were isolated in 42.6% of NHAP patients with any identified pathogens. In particular, MRSA was a common MDR pathogen in NHAP patients. Pseudomonas species was not frequently identified. Mixed bacteria were detected in 5 patients among NHAPs and 3 patients among CAPs. The antibiotics used initially and failures of initial antibiotics are presented in Table 4. Patients with CAP received more combinations of antipneumococcal β-lactamase and macrolide. However, patients with NHAP received more antipseudomonal penicillin. Failure of initial antibiotics (6.7% vs. 1.4%; p=0.017) were more frequent in NHAP patients than in CAP.
Clinical outcomes
The clinical outcomes of patients with NHAP and CAP are shown in Table 5. The proportion of in-hospital mortalities was over two-fold higher in the NHAP group than the CAP group (10.5% vs. 3.3%; p=0.009). NHAP patients had a longer duration of hospital day, ICU stay, and antibiotics use than CAP patients.
Contributing factors to in-hospital mortality
Table 6 lists the risk factors for in-hospital mortality by logistic regression analysis models. According to univariate analysis, mortality was significantly associated with NHAP, CURB-65, confusion, involved lobes in chest X-ray, initial ICU care, MV use, and presence of MDR pathogen. After adjustment for age, sex, and other confounding factors, the number of involved lobes in chest X-ray (OR=1.708; 95% CI, 1.120 to 2.605; p=0.013) and MV use (OR=9.537; 95% CI, 1.635 to 55.632; p=0.012) were significantly associated with increased in-hospital mortality.
DISCUSSION
This study revealed significant differences in mortality and contributing factors between NHAP and CAP, especially in hospitalized elderly patients. The significant findings of this study were that overall in-hospital mortality of NHAP is about twice as high as that of CAP (10.5% vs. 3.3%) and patients with NHAP had more frequent cerebrovascular disease, neurologic disease, poor functional status, aspiration tendency, and tube feeding than those with CAP. In addition, the patients with NHAP had more severe pneumonia in terms of the clinical and radiological findings, MV use, and ICU admission. NHAP patients had more frequent MDR pathogens, especially MRSA, and higher incidences of initial treatment failure. We treated most patients with NHAP (85%) with antipseudomonal penicillin, with/without fluoroquinolones as recommended in the ATS/IDSA 2005 guidelines, to cover potential MDR pathogens, such as Pseudomonas or MRSA.6 Excess mortality was related to disease severity, such as the MV use and the number of the involved lobes in chest X-ray, but not to the presence of MDR pathogens. To avoid the effect of age, we restricted the analysis to patients aged 65 years or more. Klapdor, et al.14 showed that NHAP in older adult patients was different from younger patients. CAP in older adults also has different clinical characteristics and outcomes, compared with CAP, in younger patients.15 Our study is in line with another study of NHAP in terms of mortality. In other studies, the reported 30-day mortality of NHAP ranged from 16.8% to 26.6%, as in our study (19.5%).101416171819 The higher mortality in NHAP, compared with CAP, is well known, while greater detection of MDR pathogens is controversial. In our study, the prevalence of MDR pathogens was 21.9% (MRSA: 10.5%, Pseudomonas 6.7%, ESBL 4.8%) for the total NHAP population and 1.4% for CAP; the most common pathogen was Streptococcus pneumonia in both groups. However, the identification of MDR pathogens differs across countries and studies. In the United States, Dhawan, et al.9 reported that the most frequent pathogens of NHAP were gram-negative bacteria (GNB) (up to 55%), Streptococcus pneumoniae (up to 48%), Staphylococcus aureus (up to 33%), and Pseudomonas aeruginosa (up to 7%). In severe pneumonia, Staphylococcus aureus and GNB were detected more frequently.20 A prospective German cohort study of 518 NHAP patients aged 65 years and older found that MDR pathogens were very rare (5%), and MRSA was relatively more frequent in the NHAP patients (2.3% of all NHAP).10 A Spanish study detected potential MDR pathogen in 7%, MRSA in 2%, Pseudomonas in 1%, and GNB in 3%.17 In a prospective cohort study of 116 NHAP patients aged 65 years and older in Hong Kong, Ma, et al.21 found that the patients with NHAP had more viral infections (55.9%), whereas those with CAP had more bacterial infections (69.9%). MDR pathogens were found only in six patients in the entire study population. In a Japanese study of 138 NHAP aged 65 years or older, MRSA (8.7% vs. 2.3%), Klebsiella pneumoniae (11.6% vs. 3.9%), and Proteus mirabilis (2.9% vs. 0%) were identified more frequently in NHAP than in CAP patients.22 Our study had similar results for MDR pathogens as Japanese, while the rate was higher in the United States and lower in Europe. There are a few reported Korean studies on NHAP, while there are several studies on HCAP. In a Korean study of 58 NHAP patients, potential drug-resistant pathogens were detected more frequently in the NHAP group (22.4% vs. 9.9%; p=0.018), compared to CAP, and Pseudomonas aeruginosa and MRSA were detected in 8.6% and 10.3%, respectively.19 In another Korean study of 66 NHAP patients, MDR pathogens were also highly detected in NHAP (39% vs. 10%), compared to CAP. However, the isolation rate of Pseudomonas aeruginosa and MRSA were 3.0% and 4.5%, respectively.23 These studies showed a similar rate of MDR pathogens in NHAP groups with our study. However, the rate of MDR pathogens in CAP patients was relatively higher than our study. Our study had a greater number of enrolled patients in both groups and included more patients living in the metropolitan area than previous Korean studies. As shown in this and other studies, the mortality in NHAP was higher than in CAP, although the incidence of MDR pathogens varied across the studies. However, there was little evidence that more MDR pathogens caused excess mortality in NHAP. Even for HCAP, including NHAP, the association between high MDR pathogens and high mortality remains controversial. In a meta-analysis, Chalmers, et al.24 showed that HCAP had increased risk of MRSA, Enterobacteriaceae, and Pseudomonas aeruginosa, although HCAP itself was not associated with a significant increase in mortality after adjusting for age and comorbid illnesses. In a British study of 437 NHAP patients, atypical pathogen, MRSA, Enterobacteriaceae, and poor functional status were risk factors for mortality.18 In a Spanish study of 150 NHAP patients, neurological disease, septic shock, pleural effusion, GNB, and MRSA accounted for the high mortality in NHAP.17 In our study, neither MDR pathogens in their entirety nor individual MDR pathogens were associated with mortality, even in the univariate analyses, unlike in some studies. Contrary to other studies that showed HCAP itself was an important risk factor for mortality,2526 significant risk factors for mortality in our study were the extent of pneumonia on chest X-ray and MV use after adjusting for age, sex, and other confounding factors. MDR pathogens, initial ICU admission, CURB-65, and NHAP were not significant after adjusting for other factors. Disease severity in terms of clinical and radiological severity, rather than MDR pathogen and NHAP, resulted in excess mortality in our study. This result was similar to another Korean study in which a higher pneumonia severity index score was significantly associated with mortality.27 Although we excluded patients who had DNR order, treatment restriction, such as a DNR order, may be more frequent in NHAP patients because NHAP patients are older, disabled, and have a poor functional status, and more neurological and cerebrovascular disease. Thus, NHAP may result in higher morality in real world situation. Unfortunately, in the present study, almost 85% of NHAP patients were treated with antipseudomonal penicillin without regard to the severity of illness, as recommended by the 2005 ATS/IDSA guidelines. Pseudomonas species were cultured in only 6.7%, leading them to recommend targeting these pathogens in all of their NHAP patients. Such overtreatment might lead to the development of resistant pathogens and increase costs.
This study has several limitations. First, the data were collected retrospectively from a single institution. Therefore, our results should be interpreted with caution. Second, most of the pathogens were defined based on a positive culture of sputum or endotracheal aspirate, instead of semiquantitative or quantitative cultures. Viral pathogens were not identified. Third, the proportion of patients with the causative pathogens identified was relatively low, especially in CAP (29.2%). Therefore, we could not determine whether the appropriateness of antibiotics was a significant risk factor for mortality or not. Although, more than half of the patients had normal flora in their sputum, we included only patients with positive sputum culture result. Most patients were tested with other microbiologic studies, such as blood culture and urinary antigen. Despite these limitations, our results include meaningful information about clinical and microbiological features and predictors of mortality in NHAP, compared with CAP, especially for Korean populations.
In conclusion, patients with NHAP had higher mortality rates than patients with CAP. However, the excess mortality was related to disease severity and not to the presence of multidrug-resistant pathogens or NHAP itself. Therefore, not all patients with NHAP may need broad-spectrum antibiotics, and other clinical predictive factors for specific MDR pathogens should be assessed in both CAP and NHAP.





 XML Download
XML Download