

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cerebral palsy (CP) is primarily a permanent disorder that involves movement and posture, causing limitations in activity due to non-progressive disturbances that occur in the developing fetal or immature infant brain. Medical treatment is focused on younger patients with CP; however, this disease is a lifelong condition. The overall survival rate among all children with CP until 20 years of age is 90%.1 Cathels and Reddihough2 reported that young adults with CP had considerable, continuing impairment and disability. Thus, they require ongoing and periodic treatment.
To precisely assess the patient and prepare management plans, a medical history should be obtained, and a physical examination, functional assessment, medical imaging studies, and gait analysis should be performed. A physical examination is the most useful and crucial factor for determining the presence or absence of an underlying pathology. Therefore, clinicians need to know the normal ranges of physical examination variables to evaluate a patient for CP.
The physical examination of a child with CP has been studied extensively.345678910 In addition, numerous authors have reported the normal range of motion (ROM) in healthy adults.11121314151617 However, these reports do not include essential components needed for evaluating CP during a physical examination, such as the popliteal angle and Staheli test or Silfverskiöld test. For example, the clinical significance of a popliteal angle of 45° in a 5-year-old patient is different from that in a 35-year-old patient. It has been reported that the popliteal angle tends to increase with age in younger populations.18 However, there are few such studies including both adolescents and adults.
The purpose of this study was to establish normative values and evaluates age-related changes of the physical examination variables, which are commonly used for patients with CP.
MATERIALS AND METHODS
This prospective study was approved by the Institutional Review Board of the Seoul National University Bundang Hospital (IRB No. B-1511/321-003). Informed consent was obtained from all participants or their legal guardians.
Participants
This study was conducted with healthy adolescents and adults. One hundred four healthy volunteers were enrolled and divided into four age groups: 13−20, 21−35, 36−50, and 51 years and older. There were 26 participants in each group with an equal number of men and women (Table 1). A medical history and lower extremity teleroentgenogram were obtained for each patient. Participants with musculoskeletal diseases, a previous orthopedic surgery, or a medical or neurologic disease capable of affecting normal gait were excluded.
Physical examination
A consensus-building session was held by five orthopedic surgeons, each of whom had 5−15 years of orthopedic experience, to select the appropriate components of a physical examination for patient with CP. A literature review focusing on the physical examination used to diagnose CP was performed. From the pooled articles, the physical examination components that were considered reliable by several authors were chosen.371920212223242526 Table 2 displays the studies that evaluated the physical examination tests for CP and their reliability. All decisions regarding inclusion of a physical examination and associated measurement protocols required unanimous agreement.
Selected items were: Thomas test, Staheli test, hip flexion, internal rotation of the hip, external rotation of the hip, adduction of the hip, abduction with hip extension, abduction with the hip at 90° flexion, trochanteric prominence angle, flexion contracture of the knee, knee flexion, unilateral popliteal angle, bilateral popliteal angle, ankle dorsiflexion with knee extension, ankle dorsiflexion with the knee at 90° flexion, and ankle plantar flexion. Hamstring shifting was defined as the difference between the bilateral popliteal angle and unilateral popliteal angle.
The measurements were taken by three orthopedic surgeons (SJM, BCC, and MKC) and each surgeon evaluated part of the patients. A rater or orthopedic surgeon positioned the patient, and a research assistant maintained each patient's position. Measurements were performed by the rater using a standard universal goniometer with an arm length of 18 cm and 1° increments. The method used to obtain physical measurements is described in detail in Table 2.
Statistical analysis
All data were analyzed with SPSS, version 22 (IBM, Corp., Armonk, NY, USA). We used the average value of the bilateral measurement for statistical independence when performing statistical analysis.27 One-way analysis of variance (ANOVA) with Bonferroni post hoc analysis was used to compare the age groups. p values less than 0.05 were considered statistically significant.
RESULTS
Participants' mean age was 36.1 years [standard deviation (SD) 15.2 years; range 13−69 years]. There were 52 male participants and 52 female participants. Participants' average body mass index was 23.5 kg/m2 (SD 3.0 kg/m2; range 15.9−30.7 kg/m2).
The Thomas test yielded a mean angle of 0.2° (SD 0.9°), whereas the Staheli test yielded a mean angle of -18.4° (SD 3.9°). The mean unilateral popliteal angle was 35.2° (SD 9.1°), and the mean bilateral popliteal angle was 25.5° (SD 8.5°). The mean hamstring shift was 9.7° (SD 4.6°). The mean angle of ankle dorsiflexion with knee extension was 11.3° (SD 4.8°), and the mean angle of ankle dorsiflexion with the knee at 90° flexion was 19.8° (SD 5.2°). The difference between the ankle dorsiflexion with knee extension and the ankle dorsiflexion with the knee at 90° flexion was 8.5°. The mean hip internal rotation was 39.1° (SD 9.0°), and the mean hip external rotation was 41.3° (SD 8.3°). The difference between the internal and external rotations was 2.2°; both rotations were almost symmetrical. The mean trochanteric prominence angle was 18.4° (SD 4.9°). The mean thigh-foot angle was 13.7° (SD 5.5°) (Table 3).
The Staheli test was statistically significantly different among the different age groups (p=0.002), according to one-way ANOVA. The post hoc test showed that the mean hip extension was 2.7° higher in the 13−20-year-old group than in the 21−35-year-old group (p=0.046), 3.8° higher in the 13−20-year-old group than in the 36−50-year-old group (p=0.002), and 2.8° higher in the 13−20-year-old group than in the over 51 years old group (p=0.037).
DISCUSSION
Our study presents normative data that can be widely used as a reference for evaluating patients aged 13 years and older with CP. There was no significant difference in the measures of physical examination among all the age groups, except for the Staheli test.
There was a statistically significant difference in the Staheli test. The increase in the 13−20-year-old group was 2.7°, which was low compared to the other age groups. This result may be explained by physiological change in the musculoskeletal system that occurs as part of normal ageing. Such changes include the loss in the resilience of cartilage, decreased strength of the skeletal muscle, reduced elasticity of the ligaments, and fat redistribution.29 However, this small difference seems to be clinically insignificant.
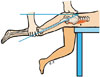
The present study showed that the bilateral popliteal angle had a tendency to increase in those over 36-years-old. Previous studies have demonstrated that the popliteal angle is increased in children and adolescents.518 The age of the cohorts in these previous studies ranged from 1−5 years. The unilateral popliteal angle with lordosis and an anteriorly tilted pelvis is a measure of functional hamstring contracture, and the bilateral popliteal angle with a loss of lordosis and neutral pelvis is a measure of the true hamstring contracture (Fig. 3). A hamstring shift greater than 20° is usually indicative of excessive anterior tilt from tight hip flexor musculature, weak abdominals, or a weak hip extensor.30 Popliteal angles are commonly used during physical examination to determine the necessity for distal hamstring lengthening in patients with CP. Some authors suggest that a popliteal angle >40−50° is an indication for distal hamstring lengthening.3132 However, Katz, et al.5 investigated the normal ranges of popliteal angle in 482 healthy children and showed that the ranges were up to 50° at ≥5 years of age. The current study also showed that 31 participants (30%) had a unilateral popliteal angle greater than 40°. Therefore, it is important to know that a popliteal angle of 40° or more is not an absolute indication of distal hamstring release. In addition, the popliteal angle should be interpreted with caution when determining whether surgery is necessary and age-related changes should be considered because weakening the hamstrings increases anterior pelvic tilt, which may actually worsen knee flexion.3334
The Silfverskiöld test is used to measure the range of ankle dorsiflexion with the knee extended and with the knee flexed 90°. If ankle dorsiflexion is decreased with the knee extended and the knee flexed 90°, a contracture of the gastrocnemius and soleus muscles is confirmed. If ankle dorsiflexion increases within the normal range with the knee flexed, an isolated contracture of the gastrocnemius muscle is confirmed. DiGiovanni, et al.35 defined the gastrocnemius contracture as less than 5° of dorsiflexion with the knee in extension, and the gastrocnemius-soleus contracture was defined as less than 10° of dorsiflexion with the knee in 90° flexion. In our study, the mean value of ankle dorsiflexion with knee extension was 11.3° [95% confidence interval (CI): 10.4−12.3°], and that of ankle dorsiflexion with the knee 90° flexion was 19.8° (95% CI: 18.8−20.8°). The mean difference between these values was 8.5°, and there was no significant difference among all the age groups. A similar result has been reported in children,18 suggesting that normal gastrocnemius muscle length is not affected by age in healthy people.
Our study has several strengths. We used a well-designed study model. Each age group consisted of an equal number and ratio of men and women. Several studies have investigated the normative value of a few items that do not apply to all kinds of physical examinations for evaluating patients with CP. However, we comprehensively suggest normative data of physical examinations that are primarily used to evaluate patients with CP.
There is a limitation to this study. We used a goniometer to measure the ROM during the physical examinations, and we held a consensus-building session to reduce variability in the value. Several authors have introduced different tools to improve the accuracy and reliability of ROM measurements such as ultrasonography or an inertial sensor, which is an optoelectronic system used to measure three-dimensional orientation.36 We need to consider using these tools to obtain a more accurate value when we conduct further research. Nevertheless, goniometric measurements are frequently used in the clinical setting, therefore, our results may be useful to clinicians.
We documented normative values that can be widely used for evaluating CP in patients 13 years and older. Further research is needed to determine correlations between physical examination findings and gait kinematic variables in healthy adolescent and adult populations.





 XML Download
XML Download