

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ischemic stroke shares common risk factors with coronary artery occlusive disease (CAOD). Myocardial infarction is one of the leading causes of death during long-term follow-up in patients with an ischemic stroke.1234 CAOD was present in about 70% and significant (≥50%) stenosis was noted in about 30% of stroke patients without a history of CAOD in studies using autopsy or coronary catheter angiography.56 However, evaluation of asymptomatic CAOD in stroke patients is not commonly undertaken in routine clinical practice.
Recently, multi-detector coronary computed tomography (MDCT) has been introduced for evaluating coronary arteries. MDCT accurately detects the presence of CAOD,7 and is a convenient and safe test. MDCT-based coronary findings have been found to be strong predictors of future cardiovascular events or death in patients with or without known CAOD.8910 Previous studies using MDCT showed that CAOD was present in 48–70% and significant CAOD was present in 18–33% of ischemic stroke patients without a previous history of CAOD.1112 MDCT has additional benefits in stroke patients, as it can detect the potential cardiac or aortic sources of embolism.13
Diagnosis of asymptomatic CAOD and hidden cardiac or aortic causes of stroke in stroke patients may help to reduce the risks of cardiovascular events and recurrent strokes. However, it remains unknown whether evaluation using MDCT in stroke patients affects long-term outcomes. Therefore, we investigated whether long-term cardio-cerebrovascular outcomes differ between patients who underwent MDCT during the acute stage of stroke and those who did not.
MATERIALS AND METHODS
Study design and population
This was a retrospective study of a prospective cohort of ischemic stroke patients designed to evaluate the usefulness of MDCT. This cohort included consecutive patients with acute cerebral infarction or transient ischemic attack within 7 days after symptom onset who were admitted to the neurology department of the Severance Stroke Center, Yonsei University in Seoul, Korea. Upon admission, all patients were thoroughly evaluated to determine demographic data, medical history, clinical manifestations, and vascular risk factors.14 All patients underwent brain CT and/or magnetic resonance imaging with cerebral angiographic studies, standard blood tests, and 12-lead electrocardiography. Most patients were admitted to a stroke unit and were monitored continuously with electrocardiography during their stay (average 4.9 days). Holter monitoring was also performed if a cardiac embolism was suspected on the basis of infarction pattern, patient age, or previous cardiac history. Transesophageal echocardiography was a part of the routine examination, unless it could not be performed due to either the patient’s condition or failure to obtain informed consent.
For determination of the presence of asymptomatic CAOD in stroke patients, since July 2006, MDCT was consecutively performed when a patient had at least one of the following: 1) presence of atherosclerosis in an intracranial or extracranial cerebral artery; 2) presence of ≥2 risk factors for CAOD, such as hypertension, diabetes mellitus, dyslipidemia, cigarette smoking, and central obesity; and 3) old age (males >45 years, females >55 years).12 MDCT was not performed if patients had 1) known CAOD; 2) high pulse rates that were not controlled with beta-blockers at the time of MDCT; 3) poor cooperation; 4) impaired renal function; or 5) failure to obtain informed consent. When significant (≥50%) stenosis of the coronary artery was observed on MDCT, the patients were routinely referred to cardiologists at our cardiovascular center. CAOD was then managed at the discretion of the cardiologists and neurologists, which included percutaneous coronary intervention with stent (PCI) and coronary artery bypass graft (CABG). This study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System. Informed consent was waived due to the retrospective nature of the study.
Clinical variables
We collected data on vascular risk factors for coronary heart disease, such as hypertension, diabetes mellitus, hyperlipidemia, and current smoking. The presence of valvular heart disease, atrial fibrillation, congestive heart failure, previous ischemic or hemorrhagic stroke, peripheral arterial occlusive diseases, metabolic syndrome, underlying malignancy (cancer diagnosed within 6 months prior to the index stroke, ongoing treatment for cancer, or recurrent or metastatic cancer), chronic kidney disease (estimated glomerular filtration rate < 30 mL/min/1.73 m2), and prior medication before the index stroke were also investigated. Initial stroke severity was determined based on the National Institute of Health Stroke Scale (NIHSS). Cerebral atherosclerosis was defined as having at least ≥1 steno-occlusive lesion of >50% based on the North American Symptomatic Carotid Endarterectomy Trial (for extracranial arteries)15 or on the Warfarin vs. Aspirin for Symptomatic Intracranial Disease method (for intracranial arteries).16 Framingham risk scores were calculated for each patient. Data on lipid profiles were also obtained.
Outcome data
Outcomes measured in this study were death and first occurrence of cardiovascular events or recurrent ischemic stroke. We obtained data for vascular events and death (date and causes of death) by review of the medical records and face-to-face or telephone interviews carried out by the stroke research nurse and stroke specialists. For mortality data, the date and cause of death were also identified using data from the Korean National Statistical Office. These mortality data are known to be reliable because they are collected based on a unique 13-digit identification code assigned to subjects at birth and on the death certificate. The causes of death are coded according to the International Classification of Disease, 10th Revision (ICD-10). Cardiovascular events were defined as nonfatal or fatal myocardial infarction (ICD-10 code I20-21), chronic ischemic heart disease (I25), sudden cardiac death (R96), death due to ventricular fibrillation (I49), or congestive heart failure (I50). The ICD-10 code used for coding fatal or nonfatal ischemic stroke was I63. The date of censoring was December 31, 2012.
Statistical analysis
Continuous variables are expressed as mean±standard deviation, and categorical data are expressed as number (percentage). The chi-square test or Student’s t-test was used to compare groups for categorical variables and continuous data, as appropriate. A Kaplan-Meier estimate of survival was used to compare the differences in rates of cardiovascular events or recurrent ischemic stroke between the MDCT (+) group and the MDCT (−) group. Differences were determined by the log-rank test. To identify independent factors for the events, multiple Cox regression analysis was used.
Further, to reduce the potential effects of selection bias and confounding factors in this retrospective cohort study, we estimated propensity scores for each of the entire patients enrolled in this study to match the patients who had undergone MDCT to those who had not. This was computed for each patient with a logistic regression model, including variables of age, sex, hypertension, diabetes, hypercholesterolemia, current smoking status, valvular heart diseases, atrial fibrillation, congestive heart failure, previous ischemic or hemorrhagic stroke, peripheral arterial occlusive diseases, metabolic syndrome, underlying malignancy, chronic kidney disease, prior antiplatelet/anticoagulant/statin use, initial stroke severity, concomitant cerebral atherosclerosis, and lipid profiles. Each patient was then assigned an estimated propensity score, which was the predicted probability of undergoing MDCT on the basis of patient’s observed baseline characteristics. Then, we divided the cohort into five strata defined by quintiles of estimated propensity scores. Cox proportional hazards models were employed separately within each stratum to compare the overall survival of patients undergoing MDCT with that of patients not undergoing MDCT. The five hazard ratios (HR) estimated from each stratum were combined into an overall HR for the whole cohort.
We also used Cox models for adjusting differences between the groups in other ways. First, regression adjustment was performed with inclusion of the propensity score as a linear predictor in the model. Second, the inverse probability of treatment weighting was used. We used Cox regression analysis to adjust the inverse probability of treatment weighting, as well as baseline characteristics. Finally, propensity score matching was conducted between paired patients who underwent MDCT and those who did not undergo MDCT. After matching, the baseline characteristics were compared with McNemar’s test and the paired t-test. Clustered Cox regression analysis was also performed. All calculated p-values were two-sided, and p<0.05 was considered to be statistically significant. Statistical analyses were performed using the Windows IBM SPSS software package (version 20, IBM Corp., Armonk, NY, USA) and SAS (version 9.2, SAS Inc., Cary, NC, USA).
RESULTS
Study population
A total of 4381 consecutive patients were registered between July 2006 and December 2012. This comparative analysis was designed to investigate the usefulness of MDCT among patients who had no previous history of CAOD. Consequently, of the 4381 patients, we first excluded 938 patients who had a history of CAOD (myocardial infarction, angiographically confirmed CAOD, unstable angina, PCI, or CABG) or who underwent coronary angiographic evaluation within 1 year prior to the index stroke. We further excluded 160 patients who did not have any of the inclusion criteria for screening of asymptomatic CAOD with MDCT. Patients with unavailable data on initial NIHSS scores (n=19), estimated glomerular filtration rate (n=20), or incomplete lipid profiles (n=100) and those who died of acute index stroke within 7 days of symptom onset (n=27) were also excluded. Finally, 3117 patients were included in this study. Among them, 1842 patients underwent MDCT and 1275 patients did not undergo MDCT (Fig. 1). In the MDCT (−) group (n=1275), the reasons for not performing MDCT could be determined as follows: medical reasons (52.5%, 669/1275), such as poor cooperation or general condition (34.0%), renal or contrast agent-related factors (10.0%), and rapid heart rate (8.5%); and nonmedical reasons (47.5%, 606/1275), including a failure to obtain informed consent or no specific documented reasons.
Baseline characteristics of the MDCT (+) and MDCT (−) groups
The mean age of the 3117 ischemic stroke patients enrolled in this study was 65.7±12.0 years, and 60.5% of patients were men (n=1886). On the basis of Framingham risk scores, 28.6% of patients were classified into a low risk group (10-year risk <10%), 33.2% into a moderate risk group (10–20%), and 38.2% into a high risk group (>20%). In the MDCT (+) group (1842 patients), asymptomatic CAOD was detected in 1237 patients (67.2%): minimal CAOD in 725 (39.4%), 1-vessel disease in 301 (16.3%), 2-vessel disease in 149 (8.1%), and 3-vessel disease in 62 (3.4%).
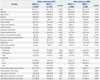
Compared to patients of the MDCT (+) group, those of the MDCT (−) group were more likely to be older, female, and non-smokers and to have hypertension, valvular heart disease, atrial fibrillation, congestive heart failure, previous ischemic stroke, peripheral arterial occlusive diseases, underlying malignancy, chronic kidney disease, prior anticoagulant treatment, more severe stroke, concomitant cerebral atherosclerosis, and relatively low triglyceride, low density lipoprotein, or high density lipoprotein levels (Table 1). In terms of medication at discharge, statins were more frequently prescribed in the MDCT (+) group (n=1773, 96.3%) than in the MDCT (−) group (n=1148, 90.0%) (p<0.001). There were similar trends in prescribing antithrombotics [n=1810 (98.3%) in MDCT (+) vs. n=1202 (94.3%) in MDCT (−), p<0.001] or beta-blockers [n=631 (34.3%) in MDCT (+) vs. n=287 (22.5%) in MDCT (−), p<0.001].
Cardiovascular and cerebrovascular outcomes
Outcomes in the original population
During a follow-up of 38.0±24.8 months (range: 0–85.9 months), 486 patients (15.6%) died. Recurrent stroke developed in 297 patients (9.5%) [fatal stroke in 106 (3.4%) and nonfatal stroke in 191 (6.1%)] and cardiovascular events in 60 patients (1.9%) [fatal myocardial infarction or sudden cardiac death in 27 (0.9%), nonfatal myocardial infarction in 29 (0.9%), and congestive heart failure in 4 (0.1%)]. The frequency of receiving revascularization therapy was statistically different between the two groups (p<0.001) in that 96 patients (5.2%) received PCI (n=87) or CABG (n=9) in the MDCT (+) group, while 13 patients (1.0%) received PCI (n=9) or CABG (n=4) in the MDCT (−) group, during follow-up. The occurrence of cardiovascular events was not associated with the Framingham risk score stratification (p=0.400).
Compared to patients in the MDCT (+) group, those in the MDCT (−) more frequently experienced death (27.9% vs. 7.1%, p<0.001), cardiovascular events (3.5% vs. 0.8%, p<0.001), and recurrent stroke (13.3% vs. 6.9%, p<0.001). Kaplan-Meier curves showed that the MDCT (−) group had higher risks of death, cardiovascular events, and recurrent ischemic stroke than the MDCT (+) group (Fig. 2). The mean annual risk of death, cardiovascular events, or recurrent ischemic stroke was higher in the MDCT (−) group than in the MDCT (+) group (9.34% vs. 2.47% for death, 1.20% vs. 0.29% for cardiovascular events, and 4.70% vs. 2.56% for recurrent ischemic stroke). After adjusting for all demographic and clinical characteristics in multivariate Cox proportional hazard models, there were significantly higher risks of death, cardiovascular events, and recurrent stroke in the MDCT (−) group than in the MDCT (+) group (Table 2).
Outcomes in the propensity score-matched population
Propensity score matching resulted in well-balanced matching between the MDCT (+) group and the MDCT (−) group. All characteristics of the two groups were well balanced with those of the unmatched cohort (Table 1). The baseline characteristics in the five strata adjusted for propensity scores are shown in Supplementary Table 1 (only online).
Kaplan-Meier curves showed that the MDCT (−) group was in higher risk of death and cardiovascular events (Fig. 3). All of the five propensity score-adjusted models consistently demonstrated that the MDCT (−) group was at a higher risk of death and cardiovascular events (Table 2). In stratified analysis based on the propensity score, the difference in the risk of death and cardiovascular events between the MDCT (−) group and the MDCT (+) group was remarkably significant among patients with high propensity scores. The MDCT (−) group seemed to also have a higher risk of recurrent stroke in most propensity score-adjusted models than did the MDCT (+) group. However, the increased risk of recurrent stroke was weaker than that of cardiovascular events. For example, in the MDCT (−) group, the HR for cardiovascular events in stratified analyses based on propensity scores was 2.692 [confidence interval (CI) 1.450–4.997, p=0.002], while that for recurrent stroke was 1.419 (95% CI 1.108–1.816, p=0.005) (Table 2). The results of 1:1 propensity matching analysis showed the MDCT (−) was related with death (HR 2.783, 95% CI 1.987–3.897, p<0.001) or cardiovascular events (HR 3.2, 95% CI 1.172–8.735, p=0.023), but not with the recurrent stroke (HR 1.173, 95% CI 0.810–1.698, p=0.398).
In addition, we performed comparative analyses using the data of the MDCT (+) group (n=1842) and 606 patients of MDCT (−) subgroup who had not undergone MDCT due to nonmedical reasons (Supplementary Table 2, only online). Kaplan-Meier curves and Cox proportional hazards models showed patients in the MDCT (−) subgroup had significantly higher risks of all predetermined outcomes (Supplementary Fig. 1, Supple-mentary Table 3, only online). Propensity score analyses showed that compared with the MDCT (+) group, MDCT (−) group was higher risk of death and tended to be higher risk of cardiovascular events or recurrent stroke (Supplementary Fig. 2, Supplementary Table 3, only online).
DISCUSSION
In this study, we found that the risks of death, cardiovascular events, and recurrent stroke were higher in stroke patients who were not evaluated using MDCT during admission than in those who were evaluated. However, evaluation using MDCT was not randomized; consequently, many baseline characteristics differed between the MDCT (+) group and the MDCT (−) group. Therefore, we compared outcomes in a propensity score-matched population. Comparison using various models in this propensity score-matched population also showed significant differences in the risk of death, cardiovascular events, and recurrent stroke between two groups. In particular, the high strata group (the highest propensity) more frequently suffered from death, cardiovascular events, and recurrent strokes.
Diagnosis of asymptomatic, but significant CAOD, using MDCT could change a treatment strategy. Likely, physicians and patients might be more motivated to manage modifiable risk factors for cardiovascular disease and to stick to treatment with medication if they recognized the presence of asymptomatic CAOD. When it comes to revascularization therapy, there has been no strong evidence of the usefulness of routine PCI for reducing cardiovascular events in patients with stable CAOD.1718 However, because the severity of silent CAOD was a strong predictor of future cardiovascular events in stroke patients, despite the use of the best medical treatment based on guidelines118 and revascularization therapy, including CABG and PCI, may be helpful for specific group of patients, such as those with ≥50% stenosis of the left main coronary artery,1719 some patients in the MDCT (+) of our study might have benefitted from revascularization therapy.
Many of the patients who did not undergo MDCT in this study might have had significant CAOD that was undiagnosed on discharge. Indeed, about 18–33% of stroke patients have been reported to have asymptomatic but significant CAOD.5611 In this study, significant CAOD was detected in 28% of patients who underwent MDCT. Thus, patients with significant CAOD that was not diagnosed before discharge might have had a greater risk of cardiovascular events during follow-up.
Notably, in the MDCT (−) group, the annual risk was 4.2 times greater for cardiovascular events and 1.8 times greater for recurrent stroke than it was in the MDCT (+) group. This suggests that the effects of using MDCT were greater for reducing cardiovascular events than for reducing recurrent stroke. MDCT is also useful in diagnosing the causes of stroke, such as aortic plaques, intracardiac thrombi, and patent foramen ovale. Although the exact diagnosis of stroke mechanisms is helpful for better stroke prevention,20 many of the etiologies, which were detected on MDCT, might have been also detected by echocardiographic studies that were a part of standard stroke evaluation in our center.2122 As a result, the treatment strategy for the secondary prevention of stroke might have not been changed in most cases of our population even though cardiac or aortic causes of stroke were detected by MDCT. However, asymptomatic CAOD could not have been diagnosed if patients were not evaluated using MDCT. These might be partly responsible for the different risks for cardiovascular events and recurrent stroke in the MDCT (−) group in the present study.
The present study does not address which patients are appropriate candidates for coronary evaluation. However, a scientific statement by the American Heart Association/American Stroke Association in 2003 recommended routine noninvasive testing for coronary heart disease in high risk groups, including stroke patients with cerebral atherosclerosis or a Framingham risk score of ≥20%.23 Previous MDCT-based studies suggest that asymptomatic CAOD is common in stroke patients with multiple vascular risk factors and atherosclerosis of the cervicocephalic arteries.1112 The present study provides supportive evidence for the necessity of coronary evaluation in acute stroke patients. MDCT has some drawbacks, such as contrast agent-related side effects, radiation-related adverse effects, and the need for the patient’s cooperation to hold their breath for a while. However, this test has an advantage for stroke patients. In contrast to a treadmill test, MDCT can be performed in patients with the level of disability seen in many stroke patients.7 In addition, many cardiac and aortic causes of stroke can be diagnosed by MDCT, as described above. Therefore, this test can be useful especially in patients for whom transesophageal echocardiography cannot be performed.1324 Defining high-risk patients for future cardiovascular events that could benefit from cardiac evaluation using MDCT is required.
This study has merit in that it was performed in a large sample of stroke patients with a long-term follow-up. However, this study also has several limitations. First, evaluation using MDCT was not randomized. Although a previous report showed that asymptomatic CAOD is common regardless of the stroke mechanism6 and we balanced the baseline characteristics of patients using various propensity score matching models, there might still be other confounders of outcomes, such as socioeconomic status. Second, adherence to medication during follow-up was not thoroughly checked. Third, although all cardiologists managed patients with CAOD based on the same guidelines, management, including revascularization therapy, was not controlled. Fourth, this study was performed in a single university hospital in one Asian country. However, the presence of vascular risk factors and occurrence of vascular events (cardiovascular or cerebrovascular) can differ between different ethnicities.25 Therefore, these limitations should be considered in the interpretation of the results of the present study.
The present study showed that stroke patients who were not evaluated using MDCT during admission had increased risks of future death, cardiovascular events, or recurrent stroke. However, the overall cardiovascular events were lower in this study population. Therefore, further studies focusing on the selection of high-risk patients for future cardiovascular events or randomized clinical trials are needed to clearly demonstrate the clinical usefulness of MDCT.




 XML Download
XML Download