

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke and transient ischemic attack (TIA) are the most common neurologic manifestations of antiphospholipid syndrome (APS).12 APS is suspected when a young patient presents with thrombotic stroke with no overt risk factors for cerebrovascular disease. The most recent international consensus criteria for APS classification (revised Sapporo criteria) require persistently positive results for antiphospholipid antibodies (aPL) on two or more occasions at least 12 weeks apart and a medium or high titers of anticardiolipin antibody (aCL) or anti-β2-glycoprotein-1 (anti-β2-GPI) antibody in association with clinical manifestations.3 Although these classification criteria were designed for research purposes, they are used in clinical practice for diagnosing APS. To confirm the diagnosis of a patient who presents with ischemic stroke and aPL positivity as definite APS, the positivity and titer of aPL are serially checked. However, the clinical relevance of persistence and medium to high titers of aPL has not yet been identified.
The prevalence of aPL in a healthy population was reported to be 8% for lupus anticoagulant (LA), 6.5% for immunoglobulin G (IgG) aCL, and 9.4% for IgM aCL in cross-sectional studies,45 whereas that of persistent aPL positivity was <2% in normal subjects who were initially found to have aCL. Moreover, in 522 healthy blood donors who were incidentally found to have aCL, no thrombotic events were found.5 However, persistent aPL positivity was more strongly associated with thrombotic events than transient aPL positivity.6 These findings imply the importance of the persistence of aPL. Nevertheless, the clinical implications of transient aPL positivity on the clinical progress of patients with ischemic stroke are uncertain.
Questions also remain concerning titers of aPL, as there are conflicting data. There are studies demonstrating that a moderate to high titer of aCL is more strongly associated with vascular thrombosis. High titers (>40 U) of aCL confer increased risk for subsequent thrombo-occlusive events after cerebral ischemia, compared with low titers (<40 U).7 Ruffatti, et al.8 showed medium to high titers of aCL to be a risk factor for thrombotic events in asymptomatic aPL carriers. On the other hand, there was a study showing that high titers of aCL caused no difference in the vascular and pregnancy risk, compared with moderate titers of aCL.9 Furthermore, comparing low titers with moderate to high titers of aPL showed no differences in vascular and obstetric events.101112
In a systematic review, a significant association between aPL and cerebrovascular events was noted, with a cumulative odds ratio of 5.48 [95% confidence interval (CI) 4.42−6.79];13 however, the risk of recurrence of thrombosis associated with aPL after the first episode of a cerebrovascular event is not well defined.14 The Antiphospholipid Antibodies and Stroke Study (APASS), a prospective cohort study within the Warfarin Aspirin Recurrent Stroke Study (WARSS), showed that the presence of either LA or aCL did not predict subsequent thrombotic events after the first ischemic stroke.15 In this study, aPL status was measured only once before randomization, and low titers of aCL were included. Moreover, anti-β2-GP1 was not included in the evaluation of aPL status. These features did not satisfy the current diagnostic criteria; therefore, they could not verify the implication of persistence or low/high titer of aPL on the risk of recurrent thrombosis.
The treatment recommendations for patients with ischemic stroke with aPL are based on APASS data, which revealed that warfarin and aspirin appear to be equivalent for subsequent thrombosis events after the first episode of ischemic stroke with aPL.15 These differ from the treatment recommendations for patients with venous thrombosis and aPL, which is to start life-long anticoagulation therapy to prevent recurrent thrombosis.16 However, as mentioned earlier, the APASS population is not confined to definite APS criteria; hence, the optimal treatment of patients with ischemic stroke who satisfy the definite APS criteria is controversial.
The aim of this study was to investigate the risk of subsequent thrombotic events in patients with ischemic stroke with aPL positivity in terms of aPL status. Furthermore, we compared the recurrence rate of thrombosis between patients treated with antiplatelets and those treated with anticoagulants.
MATERIALS AND METHODS
Patients
We collected the data of 99 patients with ischemic stroke who had at least one or more aPL-positive result (i.e., positivity for aCL, anti-β2-GPI, and LA antibodies) who presented to Yonsei University Health System, Severance Hospital. We extracted the data using the clinical data retrieval system and reviewed the medical records of patients (Supplementary Fig. 1, only online). To address the issue of the effect of persistent and medium- or high-titer of aPL on the risk of recurrence of thrombosis, we classified the 99 patients into two groups according to whether they satisfy the laboratory criteria for APS. According to laboratory criteria for APS regarding revised Sapporo classification criteria, the patients should have medium- or high-titers of aPL on two or more occasions at least 12 weeks apart.3 Forty-six of 99 (46.5%) patients were classified as having “definite APS,” meaning that they met the laboratory criteria for APS along with a clinical history of stroke. Fifty-three of 99 (53.5%) patients were classified as having “indefinite APS,” meaning that they have a clinical history of stroke and aPL positivity, but fell short of the laboratory criteria for APS.
Subgroup analysis
We subtracted 19 patients whose aPL was checked only once. We divided the remaining 80 patients whose aPL was checked more than twice into two groups: 13 of 80 (16.3%) were classified as “patients with transient aPL,” defined as patients who had a positive aPL result only once; 67 of 80 (83.7%) were classified as “patients with persistent aPL,” defined as patients who had a positive aPL result more than two times.
Furthermore, we evaluated the number of aPL-positive categories (aCL, β2-GPI, and LA) at each time and classified the patients into two subgroups according to the variation of aPL-positive categories. “Patients with increasing variety of aPL” were defined as patients whose number of aPL-positive categories had increased during the follow-up period, whereas “patients with decreasing variety of aPL” were defined as those whose number of aPL-positive categories had decreased during the follow-up. We compared these two subgroups with patients whose number of aPL-positive categories had not been increased or decreased to analyze the influence of aPL patterns on the outcome.
Data collection
The following parameters were reviewed: 1) demographic data (age and sex); 2) vascular risk factors (hypertension, diabetes mellitus, cholesterol levels, cardiac valvulopathy, arrhythmia, coronary arterial disease, prior pregnancy morbidity, and smoking status); 3) follow-up duration since the first episode of stroke or TIA and the time to recurrence; 4) treatment with antiplatelets or anticoagulants; 5) duration of anticoagulation, if received; and 6) mean international normalized ratio (INR) in patients with anticoagulation.
aPL assays
We checked the IgM and IgG isotypes of aCL and the IgM and IgG isotypes of anti-β2-GPI and LA.
The serum levels of both aCL and anti-β2-GPI were measured by using an automated fluorescence enzyme immunoassay (EliA; Phadia, Freiburg, Germany) according to the manufacturer's instructions. We used the Sydney criteria cut-off of >40 GPL/MPL units for medium or high titers of aCL IgG and IgM for patients with definite APS. The cut-off values for positivity of aCL IgG and IgM, we used 10 GPL/MPL units as proposed by the manufacturer. As there is no proposed Sydney criteria cut-off for anti-β2-GP1, we used the 99th percentile cut-off for anti-β2-GP1 for patients with definite APS, which was 18 U/mL for IgG and 7 U/mL for IgM. The cut-off values for positivity of anti-β2-GP1 IgG and IgM were 7 U/mL as suggested by the manufacturer.
LA testing was performed as follows. Peripheral blood samples were collected in 3.2% sodium citrate tubes, and platelet-poor plasma (validated by using a platelet count of <10×109/L) was obtained through double centrifugation for 15 min at 1500 rcf and 15 min at 2500 rcf at room temperature. Both screening and confirmatory tests for LA were conducted on an ACL TOP 700 coagulation analyzer (Instrumentation Laboratory, Milan, Italy) with an assay kit utilizing diluted Russell's viper venom (HemosIL Diluted Russell's Viper Venom Time Screen/Confirm kit, Instrumentation Laboratory). Initially, screening tests were conducted, and the samples with test results within normal ranges, defined as screening ratio [patient screening result (sec)/mean of normal screening range (sec)] <1.2, were reported as “negative.” Those with screening results exceeding normal ranges were subjected to a confirmatory test, and the results from the confirmatory test were compared with the screening result to deduce the normalized ratio as follows:
The results of the confirmatory test were reported according to the normalized ratio as follows: <1.2, LA negative; 1.2−1.5, LA weakly positive; and >1.5, LA positive.
Statistical analysis
All statistical analyses were performed with IBM SPSS software, version 23.0 (IBM Corp., Armonk, NY, USA). Categorical data are expressed as absolute and relative frequencies, and continuous data are presented as mean±standard deviation. The group differences were assessed by using the t-test for continuous variables, and the chi-square test or Fisher's exact test for categorical variables. The Kaplan-Meier survival method with log-rank test was used to assess the association of the time to thrombotic events and aPL status. Furthermore, univariate and multivariate Cox proportional hazard models were applied to determine the predictive value and to adjust for variables that were imbalanced and other potential confounders, including traditional stroke risk factors. A p-value of <0.05 was considered significant.
RESULTS
Comparison of baseline variables between patients with definite APS and those with indefinite APS
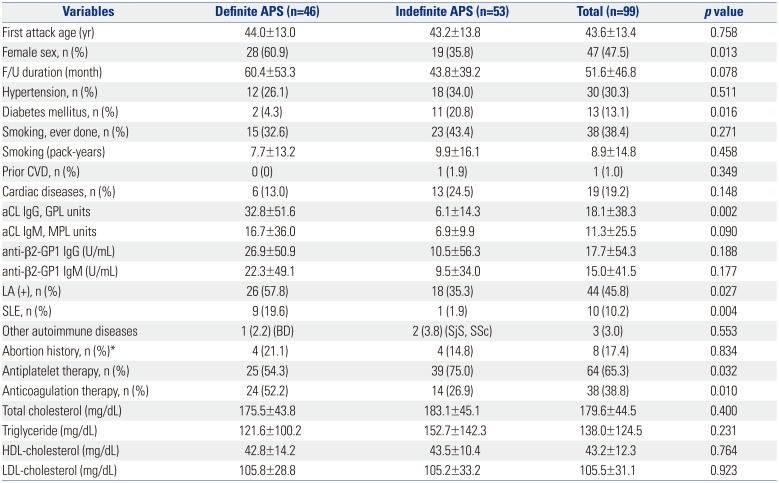
The mean age at the first event of ischemic stroke or TIA was 43.6 years, and there was no difference between patients with definite APS and those with indefinite APS. The mean follow-up duration was 51.6 months, and patients with definite APS were followed longer, although there was no statistical significance. The group with definite APS had a higher proportion of female patients and a lower incidence of comorbid diabetes mellitus than the group with indefinite APS. There were no differences in the presence of hypertension, history of cigarette smoking, prior cardiovascular diseases such as myocardial infarction or peripheral arterial occlusive diseases, combined cardiac diseases including cardiac valvulopathy, arrhythmia, coronary arterial disease, and prior pregnancy morbidity between the two groups. Nine patients among patients with definite APS and 1 patient among patients with indefinite APS had concomitant systemic lupus erythematosus (SLE). The baseline total cholesterol, triglyceride, high-density lipoproteins, and low-density lipoproteins showed no statistical differences. Among patients with definite APS, 9 patients (19.6%) were on aspirin, 3 patients (6.5%) were on clopidogrel, 10 patients (21.7%) were on aspirin+clopidogrel, 21 patients (45.7%) were on warfarin, and 3 patients (6.5%) were on warfarin+aspirin. Among patients with indefinite APS, 12 patients (23.1%) were on aspirin, 8 patients (15.4%) were on clopidogrel, 3 patients (5.8%) were on cilostazol, 15 patients (28.8%) were on aspirin+clopidogrel, 13 patients (25.0%) were on warfarin, and 1 patient (1.9%) was on warfarin+aspirin. Patients with definite APS were more frequently on anticoagulation therapy than those with indefinite APS (52.2% for definite APS vs. 26.9% for indefinite APS, p=0.010), whereas patients with indefinite APS were more frequently on antiplatelet therapy than those with indefinite APS (54.3% for definite APS vs. 75.0% for indefinite APS, p=0.032) (Table 1).
Additionally, we compared the baseline clinical characteristics between the patients with or without recurrent thrombotic events regardless of definite or indefinite APS for more information (Supplementary Table 1, only online).
Comparison of subsequent thrombotic events between patients with definite APS and those with indefinite APS
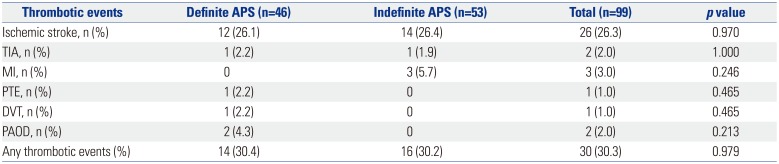
Table 2 shows the subsequent thrombotic event outcomes in patients with definite APS and those with indefinite APS. Recurrent ischemic stroke was the most common thrombotic event, which is consistent with previous studies indicating that recurrent thrombotic event occurs in the same vascular beds.
There was no increased risk of any subsequent thrombotic events, including ischemic stroke, TIA, myocardial infarction, pulmonary thromboembolism, deep vein thrombosis, and peripheral arterial occlusive diseases in patients with definite APS, compared with those with indefinite APS (30.4% for definite APS vs. 30.2% for indefinite APS, p=0.979).
There were no differences in the time to any thrombotic events between patients with definite APS and those with indefinite APS (log-rank p=0.321) (Fig. 1). After adjusting for confounders that showed imbalance between the two groups (Cox proportional hazard model), including sex, comorbid diabetes mellitus, comorbid SLE, history of anticoagulation, and antiplatelet agent, there was no increased risk of subsequent thrombotic events associated with definite APS, compared with indefinite APS [hazard ratio (HR) 1.039, 95% CI 0.449−2.404; p=0.930].
Comparison of subsequent thrombotic events according to aPL status in subgroup analysis
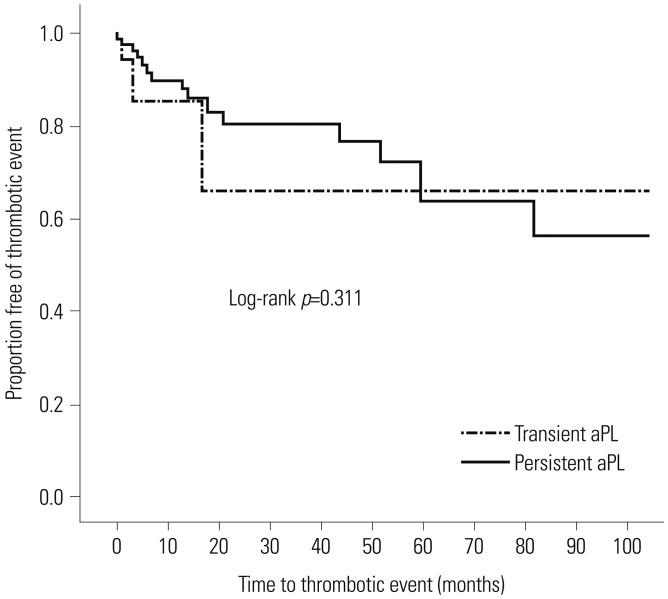
Subgroup analysis on the influence of persistence of aPL on the risk of subsequent thrombotic events was done. Thirteen patients with transient aPL had five events (38.5%) and 67 patients with persistent aPL had 18 events (26.9%), indicating that persistent aPL did not increase the risk of subsequent thrombosis in patients with stroke (log-rank p=0.311) (Fig. 2).
There were 13 patients with increasing variety of aPL and 22 patients with decreasing variety of aPL. Five patients among those with increasing variety of aPL had subsequent thrombotic events. When compared with patients without increasing variety of aPL, there were no differences in the risk of subsequent thrombotic events (38.5% vs. 24.1%; HR 1.724, 95% CI 0.603−4.930; p=0.310) (Table 3). Nine patients among those with decreasing variety of aPL had thrombotic events, which had no differences from patients without decreasing variety of aPL (40.9% vs. 24.1%; adjusted HR 1.214, 95% CI 0.512−2.882; p=0.660) (Table 4).
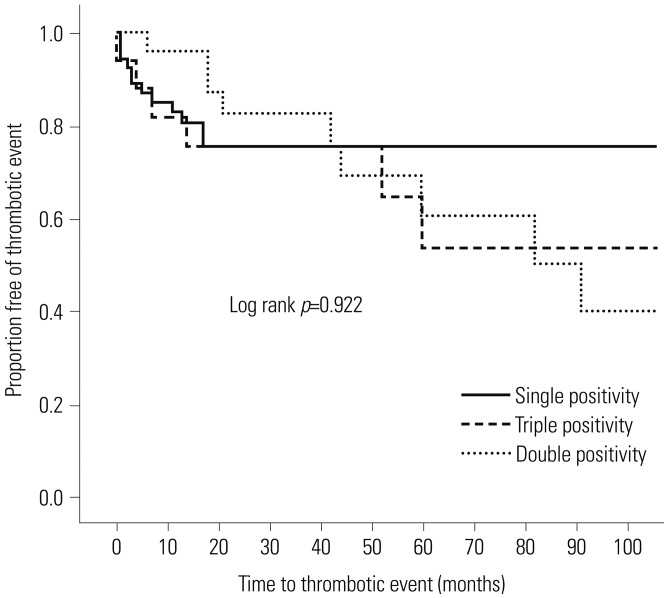
Also, we analyzed the effect of single, double, and triple positivity on subsequent thrombotic events. Among our total 99 study population, 55 patients had single positivity for aPL, 27 patients had double positivity for aPL, and 17 patients had triple positivity for aPL. There were no differences in the time to any thrombotic events between patients with single, double, and triple positivity for aPL (26.3% for single positivity vs. 40.7% for double positivity vs. 35.3% for triple positivity; log-rank p=0.922) (Fig. 3).
Comparison of subsequent thrombotic events with regard to treatment modality among patients with definite APS
About half of the patients with definite APS were receiving anticoagulation, and the other half were receiving an antiplatelet agent without anticoagulation. To evaluate the outcome according to treatment modality, we divided the patients with definite APS into two groups: 24 patients who were receiving anticoagulants and 22 patients who were receiving an antiplatelet agent only without anticoagulation. Three patients were receiving anticoagulants combined with antiplatelet agent, which we classified as the anticoagulants group. Six patients among those who were receiving an antiplatelet agent only and eight patients who were receiving anticoagulation had recurrent thrombotic events. There was no increased risk of recurrence depending on the treatment modality (27.3% vs. 33.3%; HR 0.992, 95% CI 0.341−2.891; p=0.989) (Table 5). The mean INR was 2.0 in patients who were receiving anticoagulation, and there was no difference in the INR between patients with and without recurrence.
DISCUSSION
We observed subsequent thrombotic outcomes in 99 patients who had been diagnosed as having ischemic stroke with aPL positivity at a single institution. We divided the patients into two groups by applying the APS criteria to reflect the effect of the persistence and titers of aPL and followed the patients for a mean of 51.6 months. There was no increased risk of subsequent thrombotic events after the first ischemic stroke according aPL status.
Satisfying the laboratory criteria for APS did not increase the risk of subsequent thrombotic events in patients with ischemic stroke, compared with those with aPL positivity but fell short of the laboratory criteria. Furthermore, there were no associations between aPL status with regard to the persistence or variation in the number of aPL and the risk of subsequent thrombotic events. This result is consistent with a previous APASS-WARSS study15 that showed no association between immunoreactivity to aPL and subsequent thrombotic events. However, the APASS-WARSS study checked aPL only once without considering the titers of aPL, and anti-β2-GPI was not analyzed. Owing to this limitation, the outcome of patients with stroke who fulfilled the criteria for APS was not clearly demonstrated.
Recently, a follow-up APASS-WARSS study evaluated the impact of anti-β2-GPI and the persistence of aPL on recurrent thrombotic events.17 The authors found that persistent anti-β2-GPI was associated with decreased time to thrombotic events; however, the overall event rate was not increased. Furthermore, the results were inconsistent with aCL, showing that having aCL positivity more than once was associated with a decreased risk of thrombotic events. In contrast, our data showed more consistent results showing that there were no associations between aPL and recurrent thrombotic risk, and the time to thrombotic event was not influenced by aPL.
Among our patients, 10 were diagnosed as having SLE, five of whom had underlying SLE before the first stroke event, and four were diagnosed as having SLE at the time of the first stroke event (i.e., SLE manifested with stroke). Only two patients were diagnosed as having an autoimmune disease after the stroke event during routine follow-up, one with SLE and the other with Sjogren's syndrome. No other patient was newly diagnosed as having an autoimmune disease.
Our study population was relatively young, as the mean age at the first ischemic stroke event was 43.6 years, and the mean lipid level was within the normal range, strengthening the possibility of aPL being a major risk factor in these patients. In a systemic review, the presence of aPL in young adults increased the risk by 5.48-fold for stroke or TIA.1318 However, after a diagnosis of stroke with aPL positivity, the impact of the titers or persistence of aPL on recurrence is controversial.19202122 Our data demonstrate that satisfying the criteria for APS does not constitute a higher risk for recurrence, and aPL positivity did not predict future autoimmune diseases.
We first hypothesized that an increasing variety of aPL would increase the tendency toward a more hypercoagulable status, as well as the risk of recurrent thrombosis, and that decreasing aPL might confer a lower risk of recurrence. However, neither the persistence nor variation in aPL had an influence on the risk of recurrence, implying that variation of aPL status does not provide valuable information for predicting further thrombotic events.
Although the population sample was small, we reviewed recurrence risk according to treatment modality. About half of the patients with definite APS were receiving anticoagulation and the other half were receiving antiplatelet therapy. Anticoagulation is considered to be superior to antiplatelet agents in patients with APS; however, the recurrence rate was not lower in patients treated with anticoagulants.
To our knowledge, this is the first study to apply the APS criteria with regard to recurrence in patients with ischemic stroke. Moreover, we observed the implication of aPL status. Furthermore, our study was performed at a single center that provides consistent laboratory reports on aPL, as well as standardized and experienced treatment for patients.
The limitations of this study include the retrospective nature of data from a relatively small size of patients. Moreover, concerning the LA results, it should be considered that the serial follow-up tests of LA were conducted after anticoagulation treatment, which may lead to false-positive results. Despite these limitations, this study demonstrated that the risk of subsequent thrombotic events was similar in patients with transient or low titers of aPL, compared with those with persistent and medium to high titers of aPL. However, further prospective studies with greater population are needed to confirm the role of aPL in recurrence in patients with ischemic stroke.




 XML Download
XML Download