

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Many studies have consistently reported an association between obesity and asthma.123 Obesity-related reductions in pulmonary function as well as leptin and tumor necrosis factor-α production by adipose tissue have been suggested as the mechanisms underlying asthma development in obese individuals.4 On the other hand, however, few studies have demonstrated an association between asthma and physical activity/seden-tary time/sleep time. Physical activity, sedentary time, and sleep time interact with each other, and they are also linked to obesity.567 Physical activity is inversely associated with sedentary time, while low physical activity and high sedentary time are related to obesity.89 Long sleep time is linked to obesity as an extension of sedentary time, whereas short sleep is also related to obesity.91011 Hence, it is essential to evaluate these conditions with a sophisticated model that accounts for all of these factors to identify those that contribute to asthma.
The relation between obesity and allergic rhinitis/atopic dermatitis is controversial. Allergic rhinitis was not associated with obesity in some reports;121314 however, it was clearly associated with obesity in another report.15 Atopic dermatitis is associated with obesity in North America and Asia, but not in Europe.16 Therefore, the association between obesity and allergic rhinitis/atopic dermatitis should be further evaluated. Furthermore, to the best of our knowledge, there has been no study on the relations between allergic rhinitis, atopic dermatitis, physical activity, sitting time, sleep time, and obesity after adjusting for these factors in the same model.
In this study, we evaluated the relation between asthma/allergic rhinitis/atopic dermatitis and physical activity/sedentary time/sleep time/obesity, using a nationwide representative sample of Korean adolescents. We hypothesized that lower physical activity, longer sitting time for study or leisure, short sleep time, long sleep time, and obesity would be associated with these allergic diseases.
MATERIALS AND METHODS
Study population and data collection
The Institutional Review Board (IRB) of the Centers for Disease Control and Prevention of Korea (KCDC) approved this study (2014-06EXP-02-P-A). Written informed consent was obtained from each participant prior to the survey. Because this web-based survey was performed at the schools with huge participants, the informed consent from their parents was exempted. This consent procedure was approved by the IRB of KCDC.
This study was a cross-sectional study using data from the Korea Youth Risk Behavior Web-based Survey (KYRBWS). The study covered one nation using statistical methods based on designed sampling and adjusted weighted values. The data from KYRBWS that were collected in 2013 by KCDC were analyzed. Korean adolescents from 7th through 12th grade voluntarily and anonymously completed the self-administered questionnaire. The validity and reliability of the KYRBWS were documented by other studies.1718 The surveys evaluated the data from the South Korean adolescents using stratified, two-stage (schools and classes) clustered sampling analyses based on data from the Education Ministry. The sampling was weighted by statisticians, who performed post-stratification and considered the non-response rates and extreme values.
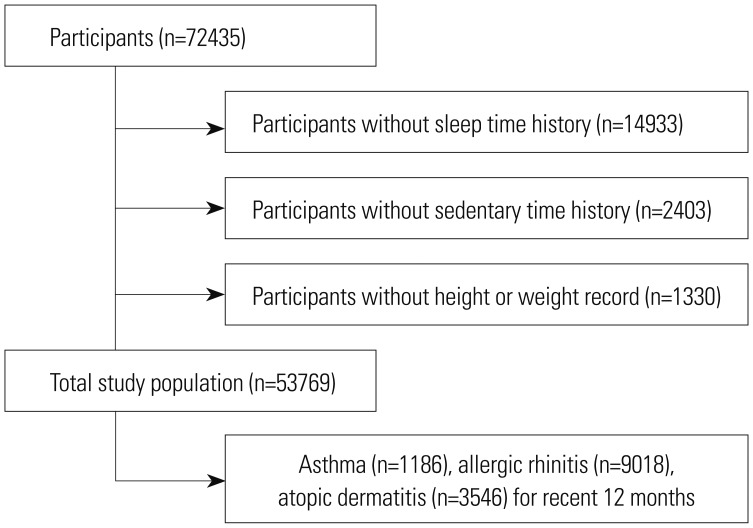
Of a total of 72435 participants, we excluded the following participants from this study: participants who did not provide their sleep time or who slept less than 2 h per night (14933 participants), participants who did not record their sitting times for study or leisure (2403 participants), and participants who did not record their height or weight (1330 participants). Finally, 53769 participants (26819 male; 26950 female) aged 12 through 18 years were included in this study (Fig. 1).
Survey
Independent variables
The days of physical activity were measured as the days in the most recent 7 days on which exercise was performed for more than 60 minutes, sufficient to increase heart rate or respiration. Because the mean physical activity day value was 1.9, physical activity was divided into the ≤2 d group (low physical activity) and >2 d group (high physical activity). The sitting time for study and leisure time within 7 days of the questionnaire was surveyed; sitting time for study included sitting time at school or a private institute, using a computer for studying, and watching educational broadcasting. Sitting time for leisure included watching TV, playing videogames, conducting internet searches not related to studying, and participating in online chats. Sitting time for study was measured in hours and minutes. The mean daily sitting time was calculated by adding the weekday sitting time and weekend sitting time and by assigning them 5/7 weight and 2/7 weight, respectively. Because the mean sitting times for study and leisure times were 6.3 h and 3.0 h, respectively, sitting time for study was divided into the ≤6 h group (low study sitting) and the >>6 h group (high study sitting), and sitting time for leisure was divided into the ≤3 h group (low leisure sitting) and the >3 h group (high leisure sitting). Sleep time in the most recent 7 days was surveyed. Times of falling asleep and waking up were measured by the hour in 10-minute increments. The sleep time duration was calculated by subtracting the falling asleep time from the waking up time. The mean daily sleep time was calculated by adding the weekday sleep time and weekend sleep time and by assigning them 5/7 weight and 2/7 weight, respectively. Sleep time was divided into 4 groups: <6 h, 6 h ≤time <7 h, 7 h ≤time <8 h, and ≥8 h. The National Sleep Foundation suggested that appropriate sleep duration for adolescents is 8 to 10 h. In Korea, only 1.1% of the participants reported sleeping >10 h per day. This >10 h sleep group was too small to be categorized as an additional group (long sleep group), therefore, we called the ≥8 h sleep group the 'relatively long sleep group', despite most of the sleep times being in the normal range. The obesity levels were categorized into 4 groups according to the Centers for Disease Control and Prevention guidelines regarding body mass index (kg/m2) for children and teens:19 obese, ≥95th percentile; overweight, ≥85th percentile and <95th percentile; healthy weight, ≥5th percentile and <85th percentile; and underweight, <5th percentile.
Covariates
The region of residence was divided into 3 groups based on administrative district: large city, small city, and rural area. Economic status was classified into 5 levels, from highest to lowest. The participants were asked to report how many days they had smoked in the last month and, based on these data, the participants were divided into 4 groups: 0 days per month, 1–5 days per month, 6–19 days per month, and ≥20 days per month. The stress level of participants was divided into 5 groups: severe, moderate, mild, a little, no stress.
Dependent variables
The participants were asked about history of their allergic rhinitis, asthma, and atopic dermatitis in the most recent 12 months and over their entire life. For example, the participants were asked, “In the past 12 months, have you been diagnosed with allergic rhinitis by a doctor?” and “Have you ever been diagnosed with allergic rhinitis by a doctor?” The participants who had been diagnosed by a medical doctor were recorded as positive.
Statistical analysis
The differences in mean age, physical exercise days, sitting time for study, and sitting time for leisure according to asthma, allergic rhinitis, and atopic dermatitis history (entire life and most recent 12 months) were compared using linear regression analysis with complex sampling. The differences in sleep time, obesity, gender, region of residence, economic level, and smoking were compared using chi-square tests with Rao-Scott corrections.
The odds ratios (ORs) of physical exercise days, sitting time for study, sitting time for leisure, sleep time, and obesity for asthma, allergic rhinitis, and atopic dermatitis (entire life and most recent 12 months) were calculated by simple logistic regression analysis with complex sampling (unadjusted) and multiple logistic regression analysis with complex sampling adjusted by age, gender, region of residence, economic level, smoking, physical activity, sitting time for study, sitting time for leisure, sleep time, obesity, asthma, allergic rhinitis, and atopic dermatitis (adjusted model).
Two-tailed analyses were conducted, and p values less than 0.05 were considered to indicate significance. The 95% confidence intervals were also calculated. After applying the weighted values recommended by KYRBWS, all of the results were presented as weighted values. The results were analyzed with SPSS ver. 21.0 (IBM, Armonk, NY, USA).
RESULTS
Compared with the control group, the participants with asthma showed higher mean physical activity, higher rates of overweight and obese, a higher proportion of males, higher economic levels, and a higher smoking rate. The participants with allergic exhibited higher mean physical activity, economic level and mean sitting time for study as well as a lower mean sitting time for leisure and less sleep time. The participants with atopic dermatitis exhibited higher mean sitting times for study and leisure, a greater prevalence of females, a higher smoking rate, and less sleep time (Table 1). The general characteristics according to the entire life histories are described in Supplementary Table 1 (only online).
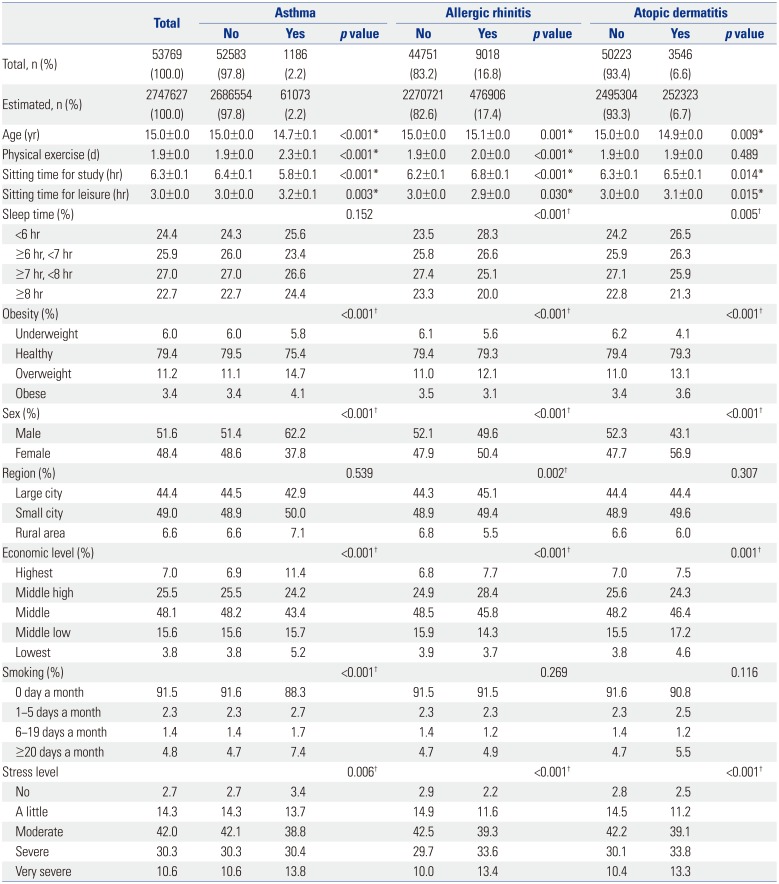
Table 1
General Characteristic of Participants According to History of Asthma, Allergic Rhinitis, and Atopic Dermatitis (Recent 12 Months)
![]()
In the unadjusted model, higher physical activity was associated with asthma and allergic rhinitis, higher sitting time for study was associated with asthma, allergic rhinitis and atopic dermatitis, less sitting time for leisure was associated with allergic rhinitis, less sleep time was associated with allergic rhinitis and atopic dermatitis, and overweight was linked to all the above three diseases (Table 2).
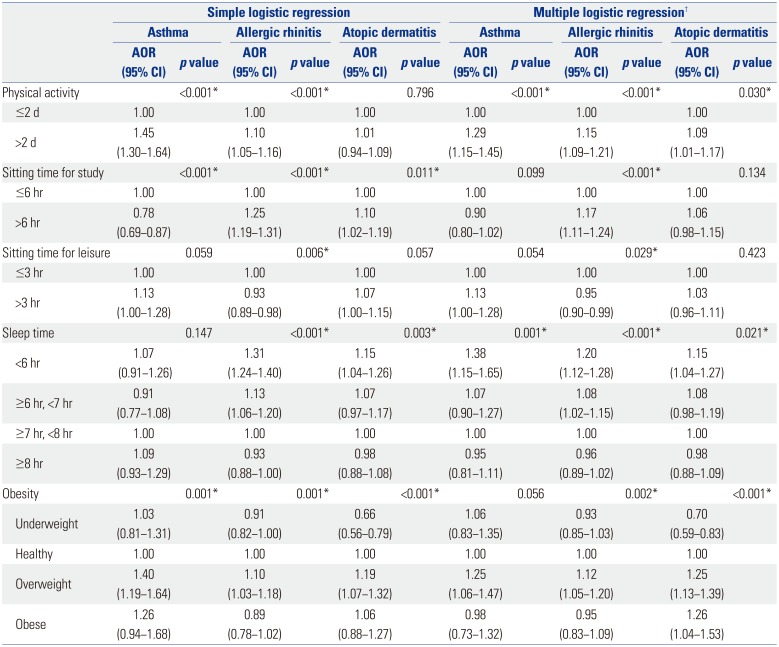
Table 2
Odds Ratios of Physical Activity, Sitting Time for Study, Sitting Time for Leisure, Sleep Time, and Obesity for Asthma, Allergic Rhinitis, and Atopic Dermatitis (Recent 12 Months) Using Simple and Multiple Logistic Regression Analysis with Complex Sampling
![]()
We analyzed the relation between the subjects' recent 12- month history and these diseases (asthma, allergic rhinitis, and atopic dermatitis) (Table 2). Higher physical activity was positively associated with all of them. Sitting time for study was positively associated with allergic rhinitis, whereas sitting for leisure was negatively associated with allergic rhinitis. Less sleep time was clearly associated with all of the above three diseases. Underweight was negatively associated with atopic dermatitis. Overweight was associated with allergic rhinitis and atopic dermatitis. Obese was only linked to atopic dermatitis. The results of simple and multiple logistic regression analyses of entire life history of asthma, allergic rhinitis, and atopic dermatitis are described in Supplementary Table 2 (only online).
DISCUSSION
High physical activity and less sleep time were consistently associated with asthma, allergic rhinitis, and atopic dermatitis. Sitting times for study and leisure were associated with allergic rhinitis. Atopic dermatitis clearly showed dose-dependent association with obesity.
In 90% of asthma patients, the disease can be exacerbated by exercise.20 Therefore, many children with asthma should restrict their exercise,21 but exercise can reduce the risk of asthma.22 We hypothesized that asthma might be associated with lower physical activity; however, the observed result was opposite. Asthma has been associated with lower physical activity.22324 whereas it has been linked to higher physical activity1325 or not associated with physical activity.262728 Participants with asthma might have exercised more to improve their health, or participants with high physical activity might have been over diagnosed with asthma due to exercise-induced symptom aggravation compared with those with low physical activity.25 Sweating is the most commonly reported exacerbating factor for itching in patients with atopic dermatitis.29 Consistent with a previous study,13 we found that high physical activity was related not only to asthma but also to allergic rhinitis and atopic dermatitis. Confounding factors that we did not consider, such as residential environment, dietary habits, and the number of people in the household, might have affected these associations.
Previously, asthma was shown to be associated with sedentary behavior,226 and asthma/allergic rhinitis/atopic dermatitis with sedentary time.13 Furthermore, active and passive sedentary behaviors were found to be differentially associated with obesity.30 In the present study, we divided sedentary (sitting) time based on specific purposes. As shown sitting time for study (mean, 6.3 h) was twice long compared to sitting time for leisure (mean, 3.0 h). Therefore, sitting time for study showed a potential relation with allergic diseases, while the relatively short sitting time for leisure showed inconsistent results. Differences in study and leisure sitting time locations might have affected the relations with allergic diseases.
Short sleep time (<6 h and 6 h ≤time <7 h) was associated with all of the diseases, whereas relatively long sleep time (≥8 h) was not. In a previous report, asthma in children was associated with sleep apnea, which was influenced by obesity.31 In the present study, asthma was associated with a short sleep time, even after adjusting for obesity. Poor sleep hygiene in children with asthma and allergic rhinitis was previously reported.32 Patients with asthma, allergic rhinitis, and atopic dermatitis experience sleep disturbances because of their symptoms, such as coughing and dyspnea,33 nasal obstructions,34 and itching,35 respectively. Short sleep times are not only a consequence of these diseases but also a risk factor for them. In a healthy volunteer study, sleep deprivation was found to cause the release of various cytokines; IL-4 and IL-β, which increased in allergic diseases, were related to increased rapid eye movement sleep latency.36 In some studies, sleep time itself was not associated with asthma, whereas missed sleep was indicated as a risk factor for asthma by inducing anxiety. In a study using polysomnography, children with asthma exhibited short sleep durations.
Asthma has been associated with obesity in many studies.12 One study found this association specifically in women,3 and another report found this association only in underweight individuals.14 In many reports, allergic rhinitis was not associated with obesity,121314 and associations with atopic dermatitis were not consistent.1416 In our present study, underweight was negatively associated with atopic dermatitis, whereas obese was positively related to atopic dermatitis. On the other hand, the association between obesity and asthma was not statistically significant, and the relation between obesity and allergic rhinitis was inconsistent.
The primary advantage of the present study was the large sample population (53769 participants), which enabled us to evaluate a representative population to ensure external validity. Moreover, we analyzed various factors, such as physical activity, sedentary time according to purpose, sleep time, and obesity, as well as other confounding factors, such as region of residence, income level, and smoking status. In the present study, we examined short sleep time in conjunction with possibly related behaviors such as physical activity and sedentary time, and formed that short sleep time was associated with all three diseases after adjusting for obesity, whereas other study focused on obstructive sleep apnea and asthma.31
Despite these advantages, the present study had several limitations. First, the study used a self-reported survey. Therefore, physical activity, sedentary time, and sleep time were evaluated based on self-reporting, while asthma, allergic rhinitis, and atopic dermatitis history were determined by verbal evidence, not by medical reports. This approach might have introduced inaccuracies due to recall bias; however, this method made it easier to inexpensively gather information from a large cohort. Therefore, objective measurements of physical behavior using an accelerometer would be desirable. Second, we measured physical activity days, not daily physical activity time. In contrast, sitting and sleep times were surveyed as daily times. Therefore, we could not sum the daily activity. Additionally, we did not measure moderate or vigorous physical activity separately. Third, the study is subject to the same limitations of all cross-sectional studies, including possible reverse causality; therefore, our calculated ORs should be interpreted with caution. Fourth, ~25% of participants were excluded due to incomplete questionnaire, which could act as the bias in this study. In conclusion, high physical activity, and short sleep time were associated with asthma, allergic rhinitis, and atopic dermatitis. However, the associations between obesity and these allergic diseases were inconsistent after adjusting for other factors.
 XML Download
XML Download