

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
To perform a thorough decompression of the foramen during anterior cervical discectomy or corpectomy procedures, it is advantageous to mobilize the longus colli muscle laterally to expose the lateral edge of the uncinate processes. This should be done carefully to avoid injury to the sympathetic trunk, as well as the vertebral artery. It has been reported that the distance between the medial border of the cervical sympathetic chain and the medial border of the longus colli muscle is 11.6 mm to 17.4 mm123 and that the distance between the medial border of vertebral artery and the medial border of the longus colli muscle is 8.0 mm to 11.6 mm, depending on the cervical level.456
While there have been reports concerning the inter-muscular distances between the medial border of the longus colli muscles, as a reference for exposing disc spaces,1257 to our knowledge, there are no reports concerning the extent to which one must elevate the longus colli muscle to expose the uncinate processes. The purpose of the present study was to elucidate the anatomic relationship between the longus colli muscle and the uncinate process of the cervical spine. Further, we sought to determine the ease with which we could utilize MRI and CT scans to measure the extent to which the longus colli muscle needs to be dissected to expose the lateral border of the uncinate process.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board (IRB) at Hallym University Sacred Heart Hospital (IRB number: 2014-I002). This study involved 120 patients randomly selected from 333 Korean patients who had a cervical spine MRI and CT because of symptomatic cervical spine issues, including neck pain, pain radiating through the arm, or walking difficulty, from January 2003 to October 2013. There were 60 males and 60 females. They were subdivided into six groups according to their age: 20–29, 30–39, 40–49, 50–59, 60–69, and 70+years. We excluded patients with a previous history of cervical trauma and any spinal operations for infective spondylitis, spinal tumor, or severe deformity. All MRIs were obtained using a 1.5-T superconductive imager (Intera, Koninklijke Philips Electronics N.V., Amsterdam, the Netherlands) under the following settings: oblique T2-weighted fast spine-echo imaging (repetition time/echo time 3500/148.58, thickness of slice 2 mm, field of view 249 mm, matrix size 512×247, number of excitation 3).
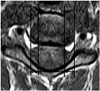
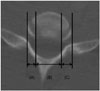
We measured three parameters on the MRI scans at C3–4, C4–5, C5–6, C6–7, and C7–T1 disc levels (Fig. 1). In addition, we measured three parameters on axial CT scans from C3–4 to C7–T1 (Fig. 2).
All statistical analyses were performed with SPSS software, version 13.0 for Windows (SPSS Inc., Chicago, IL, USA). Values are expressed as mean values with the standard deviation. Differences in continuous variables between the two groups were examined with a paired or unpaired t test. Differences in continuous variables between the different age groups were examined with ANOVA test. Correlation of continuous variables between the two groups was examined with a Pearson correlation. It was considered significant when p was less than 0.05.
In the preliminary study, all twenty patients were measured for intra-observer and inter-observer reliability. The intra-observer and inter-observer reliability were calculated using the reliability statistics by intraclass correlation (ICC). The ICC values were graded using previously described semiquantitative criteria: excellent for values in the 0.9–1.0 range, good for 0.7–0.89, fair/moderate for 0.50–0.69, low for 0.25–0.49, and poor for 0.0–0.24. Intra-observer reliability and inter-observer reliability for the uncinate process were good at 0.998 and 0.994, respectively, using ICC reliability statistics. Intra-observer reliability and inter-observer reliability for the longus colli were good at 0.997 and 0.993, respectively, using ICC reliability statistics.
RESULTS
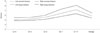
The mean values were 5.9±1.6 mm for the left longus colli distance, 15.3±2.6 mm for the inter-longus colli distance, 6.5±1.9 mm for the right longus colli distance, 5.4±1.0 mm for the left uncinate distance, 17.0±2.3 mm for the inter-uncinate distance, and 5.4±1.1 mm for the right uncinate distance (Table 1). The longus colli distances, uncinate distances, and inter-uncinate distances increased from C3 to T1 (Table 1, Fig. 3). The interlongus colli distances increased from C3 to C7 (Table 1). One hundred six patients were right-handed (88.3%) and fourteen were left-handed (11.7%). The right-handed patients had longer longus colli distances on the right side than those on the left side at disc level C6–7 (p<0.05) (Table 1). The mean body mass index of the subjects was 21.05±5.3 kg/m2 (range: 13.5–37.1 kg/m2).
To fully expose the uncinate processes, the longus colli muscles had to be dissected laterally 5.1±1.0 mm on the left and 5.5±1.2 mm on the right at C3–4, 5.2±1.7 mm on the left and 5.6±1.5 mm on the right at C4–5, 5.6±1.2 mm on the left and 6.0±1.4 mm on the right at C5–6, 6.3±1.3 mm on the left and 7.3±1.7 mm on the right at C6–7, and 7.2±1.6 mm on the left and 8.1±2.1 mm on the right at C7–T1 (Table 1).
There was no difference in the longus colli distances and uncinate distances between males and females (Table 2). The inter-longus colli distances and inter-uncinate distances were larger in males than females, except the inter-longus colli distances at C4–5 and C7–T1 (p<0.05) (Table 2). There were no differences in the longus colli distances, inter-longus colli distances, uncinate distances, and inter-uncinate distances among the different age groups (Table 3). The longus colli distances were weakly correlated with uncinate distances from C3 to T1 on the right side only (p<0.05) (Table 4).
DISCUSSION
A number of studies have investigated the anatomical relationship between the longus colli muscle and the sympathetic chain, as well as the vertebral artery. Ebraheim, et al.2 found that the distance from the medial border of the sympathetic trunk to the medial border of the longus colli muscle was an average of 10.6 mm in a study with 28 adult cadavers. Civelek, et al.3 found that the distance from the medial border of the sympathetic trunk to the medial border of the longus colli muscle was an average of 11.6±1.6 mm in a study with 30 cadavers. The distances from the medial border of the sympathetic trunk to the medial border of the longus colli muscle decreased from C3 to T1 in one study with 24 cadavers.1 In contrast, the distance from the medial border of the vertebral artery to the medial border of the longus colli muscle gradually increased from C3 to C6 in a cadaveric study,5 as well as from C5 to C7 in a human CT study.6 Thorough knowledge of such anatomical relationships between the longus colli muscle and the sympathetic trunk, as well as the vertebral artery, can help reduce the risk of complications during anterior surgery. Similarly, knowledge about the anatomical relationship between the uncinate process and the longus colli can be of benefit. This is especially true when performing thorough decompressions of the foramen in arthroplasty cases. However, we were unable to find any reports concerning the extent to which the longus colli must be mobilized to fully expose the uncinate processes out to its lateral margin during anterior cervical surgery.
We found that the longus colli distances, uncinate distances, and inter-uncinate distances increase from C3 to T1. To fully expose the uncinate processes, the longus colli muscles had to be dissected laterally 5.1±1.0 mm on the left and 5.5±1.2 mm on the right at C3–4, 5.2±1.7 mm on the left and 5.6±1.5 mm on the right at C4–5, 5.6±1.2 mm on the left and 6.0±1.4 mm on the right at C5–6, 6.3±1.3 mm on the left and 7.3±1.7 mm on the right at C6–7, and 7.2±1.6 mm on the left and 8.1±2.1 mm on the right at C7–T1. We suggest rounding off these numbers to make it easier to remember, such that the longus colli muscles are dissected laterally approximately 5 mm at C3–5, 6 mm at C5–6, 7 mm at C6–7, and 8 mm at C7–T1. The right side required greater dissection than the left at all levels. There was no difference in the longus colli and uncinate distances between males and females. Except for the inter-longus colli distances at C4–5 and C7–T1, the inter-longus colli distances and inter-uncinate distances were larger in males than females. There were no differences in the longus colli distances, interlongus colli distances, uncinate distances, and inter-uncinate distances among the different age groups. We were able to determine these values at all levels on all MRI and CT scans.
There are several reports concerning the lateral dimensions of the longus colli muscles using ultrasonography. The lateral dimension of the longus colli was reported to be 10.61±1.53 mm on the left side and 11.73±2.23 mm on the right side in 15 healthy subjects between 19 to 41 years old muscles measured by ultrasonography.8 In an ultrasonographic study of 20 patients with chronic neck pain and 20 healthy matched controls, the lateral dimensions of the longus colli were not different between the two groups.9 The lateral dimension of the longus colli in the patient group was 10.89±2.07 mm on the dominant side and 10.86±1.87 mm on the nondominant side versus 10.95±2.08 mm on the dominant side and 10.76±1.48 mm on the nondominant side in the controls.9 These values are higher than the ones we found. This is because the definition of the longus colli distance in our study (i.e., the amount of longus colli muscle needed to be dissected to expose the uncinate process) is different from the ultrasonographic study, which measured the total width of the longus colli muscle. Our results are similar to the previous cadaveric studies in which the distances between the medial borders of longus colli muscles increased from C3 to C7.1257
Our results showing increasing uncinate distances from C3 to T1 are similar to two previous studies (Table 5).1011 However, another cadaveric study found no obvious pattern of increasing or decreasing distances from C3 to C7 (Table 5).7 This might be explained by the fact that they used different measuring methods: the width was measured from the medial to the lateral margins of the uncinate process at its base on the coronal plane,1011 or from the medial to the lateral surfaces of the uncinate process at the mid-portion of the uncinate process on the coronal plane.7
As with any study, the present investigation has several limitations. First, the study was done in Koreans, and lengths may be different in other races. Second, the measurements were made in 120 cases and there may be rare variations in anatomy. There may also be individual variations based on body size such that one cannot blindly trust the numbers that we describe for any given patient. Our finding that CT and MRI scans could be utilized in all 120 cases points out the utility of using such studies to make these measurements prior to surgery. Despite these shortcomings, to our knowledge, this is the first report providing anatomic measurements that can be used as a guide for dissection of the longus colli muscle to expose uncinate processes.
In conclusion, our results suggest that in most cases, one can safely dissect the longus colli muscle laterally approximately 5 mm at C3–5, 6 mm at C5–6, 7 mm at C6–7, and 8 mm at C7–T1 to expose the uncinate process during anterior cervical surgery. It should be noted that these numbers should only serve as a guide and that individual measurements may differ due to anatomic variations. Therefore, it is recommended that the surgeon examine pre-operative CT or MRI prior to performing such dissection.





 XML Download
XML Download