

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lacunar stroke is a subtype of ischemic stroke, accounting for about 20% of brain infarcts.1 Lacunar stroke lesions are commonly located in the basal ganglia, thalamus, internal capsule, and brainstem. This type of stroke has distinct clinical features and a risk factor profile compared to other stroke subtypes such as large artery atherosclerosis or cardioembolism.2 Lacunar stroke presents with small ischemic lesions that result from small vessel disease manifesting as occlusion of a single perforating artery.3 However, the mechanism of lacunar stroke is not clearly understood. Pathologic studies have suggested that the characteristic vascular finding is lipohyalinosis and/or microatherosclerosis involving single perforating end-arteries.3 Patients with lacunar stroke share characteristics common to other forms of small vessel disease, such as increased microvascular resistance, impaired endothelial function, and reduced cerebrovascular reactivity.1
Transcranial Doppler ultrasound (TCD) is a safe and non-invasive technique widely used in clinical practice for cerebrovascular disease. Unlike other angiographic studies, which mainly provide information on the large cerebral arteries (stenosis or occlusion), TCD can provide information on various parameters for structural, functional, and hemodynamic conditions of cerebral circulation, including blood flow velocity and pulsatility index (PI).45 PI values are easily calculated from the waveform of blood flow in the cerebral artery examined. PI increases in accordance with distal vascular resistance and is considered a marker of small vessel disease and microangiopathic changes in brain.67 Indeed, PI is increased in patients with vascular risk factors or pre-existing microangiopathy including hypertension, diabetes mellitus (DM), retinopathy, nephropathy, and white matter disease.89
Based on the current understanding of lacunar stroke as a manifestation of small vessel disease, we hypothesized that the PI, a marker of cerebral small vessel disease, might also be associated with the degree of ischemic injury in acute lacunar stroke. To better understand the role of small vessel disease in lacunar stroke, we undertook this study to determine whether the PI value measured in acute lacunar stroke has an influence on the size of infarct volume.
MATERIALS AND METHODS
Study design and subjects
The study candidates were patients admitted for acute lacunar stroke to our hospital between February 2005 and October 2014. Only those patients who completed both diffusion-weighted MRI (DWI) and TCD examination within 7 days from stroke onset were included. Patients with a poor temporal window for TCD and those with cardiac arrhythmia, which could interfere with exact measurements of PI in TCD, were excluded. Acute lacunar stroke was defined as a DWI finding showing focal high signal intensity in the territory of a single perforating artery (in deep gray or white matter of the cerebral hemispheres or brainstem) compatible with clinical presentation. Patients with acute ischemic lesions extending to the cerebral cortex, those with multiple lesions, and those whose lesions were greater than 20 mm in maximum diameter were excluded, as these cases were generally not considered to be caused by the occlusion of a single perforating artery.10 To exclude the potential effects of large artery disease on PI and infarct volume, only those patients who had no significant stenosis on magnetic resonance angiography or CT angiography were included. We also excluded patients with a mean blood flow velocity of the middle cerebral artery (MCA) of >120 cm/sec in TCD, which suggested significant narrowing of the vessel. In addition, patients with potential sources of cardioembolism such as atrial fibrillation and those who received thrombolytic therapy were excluded. In the end, this study included 64 patients with acute lacunar stroke. The Institutional Review Board at CHA Bundang Medical Center approved this study and waived informed consent from the subjects due to the retrospective and observational nature of the study.
Characteristics and risk factors
We collected information regarding sex, age, presence of hypertension, DM, current smoking, and previous stroke. Criteria for the diagnosis of hypertension were the use of antihypertensive medication, a systolic blood pressure (SBP) of ≥140 mm Hg, or a diastolic blood pressure (DBP) of ≥90 mm Hg on repeated measurements. A diagnosis of DM was based on a fasting plasma glucose level of ≥7.0 mmol/L or treatment with oral antidiabetic medication or insulin. Current smokers were defined as those who had smoked within one year. We also collected laboratory findings obtained at admission including white blood cell count, hematocrit, serum creatinine, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, C-reactive protein (CRP), and homocysteine. On the day of TCD examination, SBP/DBP over brachial artery, and heart rate (HR) were recorded.
TCD examination
TCD studies were performed using a Power M mode transcranial Doppler (PMD-100/150, 2 channels, Spencer Technologies Inc., Seattle, WA, USA) with a 2-MHz probe.11 TCD examination was performed along the full segments of the MCA; the depths of insonation were 45–60 mm for the MCA. Systolic, diastolic, and mean blood flow velocity (SFV, DFV, MFV) were calculated automatically by the TCD device. Values with the highest MFV were selected from several measurements on each side. PI was derived using the formula [PI=(SFV-DFV)/MFV]. We used the mean values of TCD parameters including PI, obtained from the bilateral MCAs, for analysis.
Measurement of infarct volume and Fazekas scale on MRI
Brain MRI including DWI sequence was performed using one of three 1.5-T systems (Sonata, Siemens Medical, Erlangen, Germany; Signa Excite, GE Healthcare, Milwaukee, IL, USA; Signa HDx, GE Healthcare, Milwaukee, IL, USA). Acute ischemic lesions were defined as high-signal intensities on the DWI. Infarct volume was measured using the three-dimensional image analysis software Mango (Multi-Image Analysis GUI, Ver. 3.1.2 for Windows, Research Imaging Institute, San Antonio, TX, USA; http://ric.uthscsa.edu/mango/). For each axial DWI, the greyscale value of each pixel was measured, and the regions with higher grey-scale values than adjacent normal brain tissue were captured as the region of interest (ROI) using a semi-computerized, intensity-threshold method. Infarct volume (mm3) was calculated as the product of the sum of the ROI on each axial DWI slice multiplied by the slice thickness (5 mm).
Using axial T2-weighted or fluid attenuation inversion recovery MRI, the degree of white matter changes was classified according to the Fazekas scale (0, 1, 2, 3; 0 indicates absent and 3 severe) as an another marker for cerebral small vessel disease.1213 The two investigators (Y.K. and J.K.) independently determined the MRI-based parameters, infarct volume and Fazekas scale, blind to both clinical and laboratory data. Interrater reliability for the Fazekas scale was assessed using kappa statistics, and the kappa value was 0.718. Disagreements on the Fazekas scale were resolved by consensus. The interrater difference of infarct volume measured by the Mango software was evaluated using a paired t-test, and the difference was not significant (p>0.05). For the analyses, the mean of infarct volume measured by the two investigators was used. Across the three 1.5-T MRI systems, there were no significant differences in terms of infarct volume or Fazekas scale (p>0.05).
Statistical analysis
Categorical data are expressed as number (%), and continuous data are expressed as mean±standard deviation (SD) or median (interquartile range). To evaluate the association between infarct volume and PI value, we performed univariate and multivariate linear regression analyses with infarct volume as a continuous, dependent variable. In the regression models, we treated PI as a continuous variable and calculated the coefficient and the 95% confidence interval (CI) per one SD increase in PI. Adjustments were performed for traditional risk factors (sex, age, hypertension, DM, current smoking, previous stroke), homocysteine, CRP, and Fazekas scale based on prior knowledge. We additionally adjusted for the variables with p<0.10 in the univariate analysis for infarct volume. All statistical analyses were performed using the R package for Windows (version 3.2.2, R Foundation for Statistical Computing, Vienna, Austria). A two-sided p value of <0.05 was considered statistically significant.
RESULTS
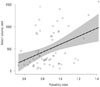
This study included 64 patients with acute lacunar stroke according to the study criteria. Among them, 46 (71.9%) were men, and the mean age was 58.17±10.23 years (Table 1). The mean infarct volume measured on DWI was 482.18±406.40 mm3 (Table 2). The mean PI was 0.86±0.18. On univariate linear regression between PI and infarct volume, PI was significantly associated with infarct volume (p=0.001) (Table 3). Fig. 1 demonstrates the proportional increase of infarct volume with PI. The Supplementary Table 1 (only online) presents the results of univariate analyses of other collected variables with infarct volume. Except for PI, all other parameters of TCD were not significantly associated with infarct volume. To evaluate the independent effect of PI, we conducted multivariate linear regression. Using a multivariate model adjusted for sex, age, hypertension, DM, current smoking, previous stroke, homocysteine, CRP, and Fazekas scale, an increase of PI was significantly associated with an increase of infarct volume (p<0.001; Model 2 in Table 3). In the final model with additional adjustments for other variables with p<0.10 in the univariate analysis, the effect of PI remained significant (p=0.022; Model 3 in Table 3). To take into account the possible confounding influence from blood pressure or MCA flow velocity at TCD measurement, we conducted sensitivity analyses with adjustments for the values (SBP, DBP, HR, SFV, DFV, and MFV), all of which failed to disprove the significance of PI on infarct volume (data not shown).
DISCUSSION
This study demonstrates that the PI value measured by TCD in acute lacunar stroke is strongly associated with infarct volume. Pathologic studies suggest that lacunar stroke is a consequence of lipohyalinosis, microatheroma, or embolic occlusion of small penetrating vessels.14 These insults lead to narrowing of cerebral small vessels and increase distal vascular resistance. This in turn causes the pattern of blood flow to be more pulsatile (increased systolic flow and decreased diastolic flow) in cerebral vessels, leading to a higher PI value on TCD assessment. Therefore, PI is regarded as a surrogate marker for cerebral small vessel disease.6 We showed that underlying severe small vessel disease (higher PI) was associated with greater ischemic injury (infarct volume) following acute lacunar stroke. Our finding indicates that small vessel disease affecting cerebral circulation is involved in the development of ischemic injury in lacunar stroke.
There are several mechanisms that can possibly explain the positive association between PI and infarct volume. As mentioned above, PI has been recognized as a marker of cerebral small vessel disease. PI is increased in those with other features of cerebral small vessel disease such as white matter disease and microbleed, which are established poor prognostic markers in acute stroke by themselves.131516171819 Higher PI may not only imply a higher severity of small vessel disease but also contribute to further vascular injury and progression of atherosclerosis in cerebral vasculature. Higher PI signifies increased transmission of pulsatile flow to distal cerebral small vessels, which could induce stretch, necrosis, calcification, fibrosis, and hypertrophy of endothelium and smooth muscle cells in cerebral circulation.720 The brain is one of the organs most susceptible to an excess of pulsatile flow, with a consistently high blood flow and low resistance.21
In lacunar stroke, early hemodynamic factors are crucial in determining whether the hypoperfused area will be transformed into a permanent infarct.2223 PI is positively associated with elevation of intracranial pressure, which results in decreased cerebral perfusion pressure.2425 The excessive pulsatile flow of cerebral circulation is accompanied by the reduction of total cerebral blood flow.26 Under normal conditions, increased pulsatile flow could be compensated for by autoregulation of the cerebrovascular system. However, as vascular reactivity is impaired in acute stroke, transmission of the excessive pulsatile flow may overwhelm the autoregulatory reserve, causing further brain damage.427 The increased pulsatile flow pattern is also associated with unfavorable conditions, including vasospasm, endothelial dysfunction, insulin resistance, oxidative stress, and inflammation.2829 Recent studies have suggested that the significance of PI is not limited to cerebral circulation only; it also reflects increased pulsatile blood pressure in systemic circulation and arterial stiffness.7920 In acute stroke, arterial stiffness is associated with progressive neurological deficits, poor functional outcome, and increased long-term mortality.3031
This study had several potential limitations. Our results were obtained from a retrospective study with a small sample size. As patients who had not completed TCD and those with a poor temporal window were excluded, the possibility of selection bias was present. The PI values could have also been affected by various clinical factors. For example, medication history, particularly that of antihypertensive agents, could have influenced both PI and brain perfusion. We did not have data on long-term outcomes including functional outcome, stroke recurrence, and mortality. Due to the limitation of the cross-sectional design, we could not definitively answer the question of whether PI is merely a marker of underlying small vessel disease or also a cause of greater ischemic injury during the acute phase of stroke. However, the effect of PI on infarct volume was significant even after adjusting for multiple risk factors including CRP, a marker of inflammation, and the degree of white matter change, which is another established marker of small vessel disease.13 There are many potential mechanisms through which increased pulsatile flow could induce structural and functional deterioration of cerebral vasculature and impair cerebral perfusion, resulting in brain injury. Therefore, we supposed that excess pulsatile flow, expressed as a high PI value, might aggravate ischemic injury in acute lacunar stroke. Further studies are needed to evaluate the mechanism behind pulsatile flow in cerebral circulation during acute stroke and the therapeutic potential of strategies for reducing pulsatile flow and consequently PI. Cilostazol, one of the antiplatelet agents frequently used in stroke prevention, can lower PI in acute stroke by reducing vascular resistance in cerebral circulation through vasodilation.532 High doses of statins may reduce PI by upregulation of endothelial nitric oxide synthase activity and downregulation of superoxide production.33
In conclusion, we demonstrated that PI has a significant positive association with infarct volume in acute lacunar stroke. The easily obtainable PI value on non-invasive TCD study may be a surrogate marker of infarct volume in acute stroke. Further studies are needed to explore the role of cerebral pulsatile flow and small vessel disease in acute ischemic injury.



 XML Download
XML Download