

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is one of the major causes of morbidity and mortality worldwide12 and is characterized by persistent airflow limitation, which is associated with an enhanced chronic inflammatory response to noxious particles or gases in the airways and the lung.3 The current pharmacological treatment of COPD is mainly symptomatic and focuses on bronchodilators, such as inhaled β2-adrenergic agonists and anticholinergics. Inhaled corticosteroids (ICS) improve lung function, symptoms, and quality of life and reduce the frequency of exacerbations in COPD patients with a forced expiratory volume in 1 second (FEV1) of <60% predicted.4 However, ICS are associated with a greater prevalence of oral candidiasis and hoarse voice, as well as an increased risk of pneumonia.5 Thus, an orally active non-steroidal anti-inflammatory agent is needed for patients with COPD. Phosphodiesterase 4 (PDE4), an isoenzyme of the PDE family, is the major regulator of cyclic adenosine monophosphate present in the inflammatory cells of the airway that are involved in the pathogenesis of COPD.6 Roflumilast has demonstrated modest improvements in lung function and reduced the frequency of exacerbations in patients with COPD.7891011 However, roflumilast also has significant adverse effects, primarily gastrointestinal and psychiatric problems.12 Recently, roflumilast received restricted approval by both the US and Korean Food and Drug Administrations for the treatment of severe COPD (post-bronchodilator FEV1 <50% predicted) and chronic bronchitis in patients who have a history of frequent exacerbations. Previous studies of roflumilast have predominantly involved Caucasian populations.7891011 However, ethnic differences may contribute to differences in drug responses and cause unexpected therapeutic and adverse effects. 13 Thus, further study is necessary to determine the efficacy and safety of roflumilast in Korean COPD patients. The JADE study, a phase III randomized trial, investigated the effect of roflumilast on pulmonary function in Asian patients with COPD.14 This post-hoc subgroup analysis evaluated the efficacy and safety of roflumilast in a Korean population and compared the efficacy among subgroups based on the Korean COPD classification guidelines.
MATERIALS AND METHODS
Patients and study design
The JADE study (ClinicalTrials.gov identifier NCT00242320) was a 12-week, double-blinded, placebo-controlled, parallel-group, phase III trial of roflumilast conducted in 35 outpatient centers in South Korea, Hong Kong, Malaysia, Philippines, and Taiwan. Korean COPD patients were recruited from 15 tertiary university hospitals. The study was approved by the Institutional Review Board or Independent Ethics Committee at each center, and all patients gave written informed consent. The inclusion criteria and main results of the study have been published previously.14 Key inclusion criteria included adults aged ≥40 years with a history of COPD as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria (post-bronchodilator FEV1/forced vital capacity ≤70%, post-bronchodilator FEV1 30–80% predicted, and FEV1 increase ≤15% and/or ≤200 mL after receiving 400 µg salbutamol). Eligible patients were stratified according to smoking status and then randomized to receive either roflumilast (500 µg) or placebo once daily. A single-blind 4-week run-in period was followed by a double-blind 12-week treatment period. Pre- and post-bronchodilator spirometry was performed at the start of the run-in period and repeated at baseline and at 4, 8, and 12 weeks during the treatment period. Patients were not allowed to take ICS, inhaled long-acting β2 agonists, oral β2 agonists, and inhaled long-acting anticholinergics during the treatment period, although salbutamol was allowed as a rescue medication. Medication history, routine physical examination, chest radiograph, resting 12-lead electrocardiogram, standard laboratory tests, vital signs, and smoking status were assessed at each visit. Patients were withdrawn from the study if they experienced a severe exacerbation or two moderate exacerbations during the treatment period. The primary efficacy endpoint was the mean [least-squares mean adjusted for covariates (LSMean)] change in post-bronchodilator FEV1 from baseline to each post-randomization visit. Secondary efficacy endpoints included the mean changes in pre- and post-bronchodilator spirometric parameters from baseline to each post-randomization visit and rate of exacerbation. Safety endpoints included adverse events (AEs), changes in laboratory values, and changes in vital signs and electrocardiograms.
Statistical analysis
Data are presented as mean and standard deviation (SD) unless otherwise indicated. Comparisons between groups were assessed using Student's t-test or the Mann-Whitney U test for continuous variables except for lung function endpoints, or χ2 or Fisher's exact test for categorical variables. Efficacy data were analyzed by intention to treat (ITT) in randomized patients receiving at least one dose of study medication. The per-protocol (PP) population was comprised of patients in the ITT population who had no documented major study protocol violations. Lung function changes were analyzed using a repeated-measures analysis of covariance (ANCOVA) for all visits from baseline to the final scheduled visit at week 12. Additionally, supportive analyses were performed using an ANCOVA model with the last observation carried forward. LS means for each treatment and the difference between treatments were calculated together with the corresponding 95% confidence interval (CI) and two-sided p-values. Safety analyses were assessed in all randomized patients who took at least one dose of the trial treatment, and patients were analyzed under the treatment they actually received. Adverse events were compared using χ2 or Fisher's exact tests. All statistical analyses were carried out using SAS for Windows XP, Version 9.1.3 (SAS Institute, Cary, NC, USA) or PROC StatXact (for nonparametric analyses) for SAS (Version 6.2, SAS Institute).
RESULTS
Demographics of study participants
A total of 260 Korean COPD patients were recruited. Of these patients, 207 (male, n=206) were randomized to roflumilast (n=102) or placebo (n=105) and included in the ITT and safety analyses. All but one randomized patient were male. A total of 72 patients in the roflumilast group and 74 patients in the placebo group had post-bronchodilator FEV1 <60% predicted. Of the 207 randomized patients, 181 completed the study, and 164 were included in the PP analyses (roflumilast, n=79; placebo, n=85) (Fig. 1). Of the 164 patients, the mean (SD) age was 66.9 (7.3) years, the mean body mass index was 22.6 (2.8) kg/m2, and the mean post-bronchodilator FEV1 was 51.7% (13.9) of the predicted value, respectively. No significant differences in baseline demographic characteristics or spirometric parameters were observed between groups (Table 1).
Efficacy analysis
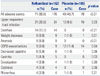
The primary endpoint (LSMean post-bronchodilator FEV1) increased by 43 mL in patients receiving roflumilast and decreased by 60 mL in those receiving placebo after 12 weeks of treatment (Table 2). The inter-treatment difference of 103 mL was statistically significant (p<0.0001), demonstrating the superiority of roflumilast for improving post-bronchodilator FEV1 in patients with COPD. Similar analyses of LSMean pre-bronchodilator FEV1 also demonstrated the superiority of roflumilast over placebo (inter-treatment difference: 119 mL, 95% CI 61–153 mL, p<0.001). Furthermore, differences in pre- and post-bronchodilator FEV1 were observed between roflumilast- and placebo-treated patients after 4 weeks of treatment and were maintained to the end of the study (Fig. 2). Subgroup analyses based on the Korean COPD classification guidelines showed a significant improvement in FEV1 in roflumilast-treated patients relative to placebo irrespective of baseline FEV1. No significant differences in the frequency of COPD exacerbations were observed between groups.
Safety analysis
During the treatment period, a higher percentage of patients in the roflumilast group (69.6%) reported AEs than did those in the placebo group (45.7%). AEs related to study medication were reported from 25 patients (24.5%) in the roflumilast group and from five (4.8%) in the placebo group. Eight patients (7.8%) in the roflumilast group and two (1.9%) in the placebo group discontinued the study due to AEs. Serious AEs were reported from nine patients (8.8%) in the roflumilast group and from two (1.0%) in the placebo group. No deaths occurred during the treatment period in either group.
The most common AEs were upper respiratory tract infection, diarrhea, weight loss, and anorexia (Table 3). Routine physical examinations and laboratory tests, including complete blood count, blood chemistry and urine analyses, and electrocardiograms, did not reveal any clinically relevant AEs. The mean change in body weight from baseline to last study visit was -2.0 (2.4) kg in the roflumilast group and +0.1 (2.0) kg in the placebo group (LSMean difference, -2.07, p<0.001).
DISCUSSION
The major findings in this study were that roflumilast improved lung function in moderate to very severe Korean COPD patients, and the AE profile was comparable to those reported in other Asian and Western populations. Results from the JADE study, which included a heterogeneous population of Asian patients with COPD from different cultural and ethnic backgrounds in Hong Kong, Malaysia, the Philippines, Taiwan, and South Korea, have already shown that the improvement in lung function and the AE profile in response to roflumilast are similar to those of Western patients with COPD.14 Differences in ethnicity may affect the pharmacological response to respiratory medications in patients with COPD, as previous studies of asthma-related medications show differences in drug pharmacology between different races, which may contribute to differences in treatment response and AEs.151617 Thus, demonstrating the efficacy and AE profile of roflumilast across different ethnic groups is clinically relevant.
Previous studies have also reported similar improvements in lung function in Western patients with COPD treated with roflumilast alone or in combination with long-acting bronchodilators.91011 The effect of roflumilast on lung function in our Korean patients was comparable to that reported in the A COPD Study Investigating Roflumilast on Safety and Effectiveness (ACROSS) study, which included 626 severe to very severe COPD patients of Chinese, Malay, and Indian ethnicities.18 Although roflumilast has no direct effects on bronchodilation, it may improve lung function by suppressing airway inflammation.
Recent Korean guidelines proposed a new classification system for COPD with a different spirometric severity cut-off value (FEV1 <60% predicted) than GOLD (FEV1 <50% predicted) to help identify those at higher risk of future exacerbations. One recent Korean cohort study demonstrated that the Korean COPD classification system is more useful for predicting COPD exacerbations than the GOLD classification system.19 Using a subgroup analysis based on the FEV1 cut-off value of the Korean guidelines, we also demonstrated that the improvement in FEV1 after roflumilast treatment was not limited to the Korean COPD group "da," as patients with FEV1 60–80% predicted also showed significantly greater improvement in FEV1 with roflumilast treatment than did those taking placebo. The beneficial effect of roflumilast on lung function was demonstrated previously in a 6-month study of Western patients with moderate to severe COPD.9 A pooled analysis of the two roflumilast studies (M2-124 and M2-125) also demonstrated that roflumilast improves lung function regardless of age, smoking status, or geographic region.20
FEV1 is the standard measurement for the diagnosis and staging of COPD and has been used as a primary measurement of lung function in many clinical trials. Although a minimum clinically important difference (MCID) for FEV1 has not been firmly established, a suggested MCID for FEV1 is 100–140 mL in patients with COPD.21 One cross-sectional study reported that a 112-mL difference in FEV1 was associated with a noticeable improvement of dyspnea in patients with COPD.22 Bronchodilator-induced improvements in FEV1 of 75–100 mL are known to improve the quality of life in patients with COPD.23 In the TOwards a Revolution in COPD Health (TORCH) trial, treatment with fluticasone alone and in combination with salmeterol improved the mean FEV1 by 47 mL and 92 mL, respectively, when compared to placebo.4 Those FEV1 improvements were associated with significantly improved quality of life scores and reduced frequency of exacerbations. A recent meta-analysis of eight trials demonstrated that roflumilast significantly improves pre-bronchodilator FEV1 (pooled effect size 55 mL; 95% CI 42–68).12 More importantly, the study showed that roflumilast treatment reduces moderate to severe exacerbations by 27% when compared to placebo.12 In this study, roflumilast improved FEV1 significantly more than placebo in moderate and severe COPD patients. The JADE study did not allow concomitant long-acting bronchodilators and ICS, which might have caused a significant FEV1 decline (60 mL) during the study period in the placebo group and might have also induced statistically significant differences when compared to the roflumilast-treated group. The recent Roflumilast and Exacerbations in patients receiving Appropriate Combination Therapy (REACT) trial demonstrated that roflumilast improves lung function and reduces exacerbations in patients with severe COPD who are at risk of exacerbations despite ICS/long-acting beta-2 agonist (LABA), even in triple combination with tiotropium.24 Roflumilast also increased post-bronchodilator FEV1 from baseline to week 52 more than placebo, with a mean difference of 56 mL (95% CI 38–73 mL).24 Additional long-term large clinical trials are required to confirm that roflumilast add-on therapy can also contribute to an improved quality of life and reduced frequency of exacerbations in Korean COPD patients.
Differences in COPD phenotypes have been noted between Asian and Western populations.25 According to one observational study, most Japanese patients with COPD have an emphysema-dominant phenotype, whereas Western patients tend to have a chronic bronchitis phenotype.26 In the Korean Obstructive Lung Disease (KOLD) cohort, chronic bronchitis was present in about 15% of COPD patients,27 and the difference in clinical phenotype was found to possibly affect the response to pharmacological treatment.28293031 Previous clinical trials in patients with severe or very severe COPD show that roflumilast reduces the frequency of exacerbations in a subset of COPD patients with chronic bronchitis.11 Regrettably, our study did not have sufficient power to evaluate the effects of treatment on the frequency of exacerbations. Previous history of exacerbation and severity of airflow limitation are the most powerful predictors of future exacerbations.3233 However, a history of exacerbations was not required for inclusion in this study, and the majority of our patients had moderate rather than severe COPD. Therefore, more than 90% of patients in both groups completed the 12-week treatment period without experiencing a COPD exacerbation. Consequently, due to the study duration, the effect of roflumilast on the exacerbation rate could not be confirmed in this trial.
Although roflumilast has been generally well-tolerated in clinical trials to date, it does contribute to adverse effects. In a pooled analysis of over 8000 patients participating in a clinical trial, the incidence of AEs and discontinuation of treatment was significantly more frequent in patients taking roflumilast than in those taking placebo.12 In our study, gastrointestinal (diarrhea, nausea, and decreased appetite), nervous system (headache, dizziness and tremor, and insomnia), and weight loss AEs were significantly more frequent in patients taking roflumilast than in those taking placebo. The incidence of these AEs in our Korean patients with COPD was similar to those reported in other Asian and Western studies.791018 However, the increased incidence of serious AEs associated with taking roflumilast, such as atrial fibrillation, psychiatric disturbance, and possible carcinogenesis, are considerable concerns.612 Phase IV post-marketing studies that are currently ongoing will reveal the long-term safety profile of roflumilast. Theophylline, a nonselective PDE inhibitor, has a mechanism of action comparable to roflumilast. Although theophylline has a small therapeutic ratio and wide range of toxic side effects, it is still widely used in Asian countries, including Korea. Theophylline also improves lung function and respiratory symptoms and reduces exacerbations in patients with COPD.34 In a meta-analysis of 20 randomized controlled trials, the mean improvement in FEV1 with theophylline was 100 mL more than with placebo, similar to what we found with roflumilast in this study.35 Clinical studies that compare the efficacy and safety of theophylline and roflumilast are needed to determine which medication has a better risk-benefit ratio.
This study had several limitations. Firstly, this study did not include patient-centered outcomes, such as dyspnea, quality of life, and exercise capacity as indicators of efficacy. Secondly, as all included patients except one were male, our conclusions may not be applicable to female Korean COPD patients. Another limitation was that concomitant treatment with long-acting bronchodilators and/or ICS was not permitted during the study. The effect of roflumilast when given as an add-on therapy to these medications is currently unknown. However, a large randomized controlled trial is currently investigating this question.
In conclusion, roflumilast significantly improved lung function and had a tolerable safety profile in Korean patients with COPD irrespective of the severity of airflow limitation.




 XML Download
XML Download