

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alcoholic liver disease (ALD) presents as a wide spectrum of liver disease, including fatty liver, acute alcoholic hepatitis, and alcoholic liver cirrhosis (ALC), and hepatocellular carcinoma.12 It is well known that almost all alcohol abusers develop hepatic steatosis; however, only a small portion develop signs of liver disease, suggesting that some of the genetic variations are involved in the etiology of ALD.34
Aldehyde dehydrogenase 2 (ALDH2), belonging to a low-Km mitochondrial ALDH, is the second enzyme to eliminate most of the acetaldehyde generated during alcohol metabolism. The human ALDH2 gene is located on chromosome 12q24.2 and composed of 13 exons, spanning 46031 bp.5 There are several polymorphism sites in the ALDH2 gene, and the Glu487Lys polymorphism (rs671, also named Glu504Lys, with the glutamate corresponding to *1 allele, and lysine corresponding to *2 allele) has been the most frequently studied. This variant could partially determine blood acetaldehyde concentrations after alcohol consumption: heterozygotes or homozygotes for the ALDH2*2 allele showed 6- and 19-fold higher blood acetaldehyde concentrations than individuals with homozygous common-allele, respectively.6 Furthermore, the variant ALDH2*2 allele is prevalent in East Asian, but is rare in non-Asians.7 Up to now, many studies have investigated the association between the ALDH2 polymorphism and the risk of alcoholic cirrhosis.8910111213141516171819202122232425 However, the results remain controversial. Therefore, in the current study, we conducted a meta-analysis in order to get a robust conclusion about the association between the polymorphism and alcoholic cirrhosis risk among East Asians.
MATERIALS AND METHODS
Search strategy
We searched the electronic literature PubMed, Web of Science, CNKI, Wanfang and Veipu databases for all relevant articles. The last search update was January 10, 2015, using the search terms: "aldehyde dehydrogenase 2 or ALDH2" and "genetic polymorphism or polymorphisms or variant" and "alcoholic liver disease or ALD or alcoholic liver cirrhosis or ALC or cirrhosis". The references of the retrieved literature were also hand-search for additional studies. There was no restriction on time period, sample size, population, language, or type of reports.
Inclusion and exclusion criteria
The studies included must meet the following criteria: 1) evaluate the association between the ALDH2 polymorphism and the risk of ALC, 2) case-control study in design, 3) provide sufficient data for calculation of the odds ratios (ORs) with the corresponding 95% confidence interval (CI). Studies were excluded if one of the following existed: 1) review articles and meta-analysis, 2) studies without the usable data of the ALDH2 genotype, and 3) duplicate publications.
Data extraction
Data were extracted independently by two investigators. The following information was extracted from each study: name of the first author, publication year, country of origin, age, gender, genotyping methods, numbers of genotypes in cases and controls, and evidence of Hardy-Weinberg equilibrium (HWE) in controls. Any encountered discrepancies were resolved by consensus.
Statistical analysis
HWE was evaluated for each study using an internet-based HWE calculator (http://ihg.gsf.de/cgi-bin/hw/hwa1.pl). The risk of ALC associated with the ALDH2 polymorphism was estimated for each study by OR and 95% CI. The heterogeneity among the results was assessed by χ2-based Q test as well as the I2 statistic.26 When a significant Q test (p>0.1) or I2<50% indicated homogeneity across studies, the fixed effects model was used,27 or the random effects model was used.28 Then, we performed stratification analyses on country. Analysis of sensitivity was performed to evaluate the stability of the results. The Begg's funnel plot and Egger's regression test were used to assess the publication bias.2930 All statistical analyses were carried out using the Cochrane Collaboration RevMan 5.2 and STATA package version 12.0 (Stata Corporation, College Station, TX, USA).
RESULTS
Study characteristics
The flow chart of study selection is presented in Fig. 1, a total of 67 articles were identified through database searching. 18 studies8910111213141516171819202122232425 were included based on the inclusion criteria. Because three studies202122 were conducted on non-Asians, they were excluded. Moreover, we excluded three studies because they did not present detailed genotyping information.232425 Therefore, as shown in Table 1, there were 12 case-control studies on ALDH2 polymorphism with 1003 cases and 2011 controls. Of the 12 eligible studies, four studies891011 were conducted on Chinese populations, five studies1516171819 on Japanese populations and three studies on Korean populations.121314 The distribution of genotypes in the controls was consistent with the HWE for all selected studies, except for two studies.1319
Quantitative data synthesis
Overall, the ALDH2 polymorphism was associated with a decreased risk of alcoholic cirrhosis (*1/*2 vs. *1/*1: OR=0.78, 95% CI: 0.61–0.99) (Fig. 2).
In stratification analyses by country, no significant associations were observed among Chinese (OR=0.77, 95% CI: 0.48–1.25), Korean (OR=0.65, 95% CI: 0.29–1.44), and Japanese populations (OR=0.97, 95% CI: 0.42–2.25) (Fig. 3).
Four studies891014 reported the alcohol consumption in ALC and control groups. Of which two studies found no significant difference between them, while other studies found that the amount of daily alcohol consumption and/or the duration of alcohol consumption history in ALC group were lower than control group (Table 2). In addition, two studies analysed the usual alcohol consumption between the ALDH2 *1/*1 and ALDH2 *1/*2 genotype in alcoholics. Interestingly, the results were inconsistent. Nagata, et al.16 found that the daily amount of ethanol used was smaller in patients with ALDH2 *1*2 than in patients with ALDH2 *1*1, while the study conducted by Yokoyama, et al.19 showed no significant difference between the ALDH2 genotype groups.
A single study was removed from meta-analysis each time to determine the influence of its individual data sets to the pooled ORs, and the estimated pooled ORs were not materially altered.
Test of heterogeneity
There was no significant heterogeneity for overall comparisons (*1/*2 vs. *1/*1: p=0.10, I2=36%). In the subgroup analysis by country, results were similar among Chinese and Korean populations (p=0.56, I2=0%, p=0.25, I2=29%, respectively), whereas significant heterogeneity between studies was observed in Japanese population (p=0.02, I2=67%).
Publication bias
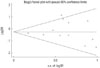
Begg's funnel plot and Egger's test were performed to assess publication bias. As reflected by the funnel plots (Fig. 4) and the corresponding Egger's test, no publication bias was detected in any comparisons (*1/*2 vs. *1/*1: p=0.655).
DISCUSSION
The metabolism of alcohol consists of two steps, it is first catalytically oxidized into acetaldehyde, and then acetaldehyde is metabolized into harmless acetate by ALDH.31 ALDH2 is the major enzyme for acetaldehyde elimination, and its polymorphism determines blood acetaldehyde concentrations after alcohol consumption. It is known that the ALDH2 *2 allele produces a catalytically inactive isozyme, which has greatly reduced or no ability to metabolize acetaldehyde.32 The accumulation of acetaldehyde in the blood and repeated high exposure to acetaldehyde after drinking might contribute to the development of ALC.33 However, the results of studies in this area are inconsistent. Chao, et al.8 reported that the ALDH2 polymorphism may contribute to susceptibility for ALC. Whereas, some studies have reported that no statistically significant association exists between the ALDH2 polymorphism and ALC risk.1434
Recently, Li, et al.35 conducted a meta-analysis and evaluated the association between ALDH2 polymorphism and the risk of alcoholism and alcohol-induced medical diseases in Asians. The results confirmed the involvement of the human ALDH2 gene in the pathogenesis of alcohol dependence as well as alcohol-induced medical illnesses in East-Asians. However, only 5 studies focusing on ALC were included in the above meta-analysis, due to the limited studies, and further analyses was not conducted. In this study, however, we conducted a comprehensive literature search in different databases (i.e., Web of Science, CNKI, Wanfang and Veipu) and added 8 studies, thus allowing for a larger number of subjects and more precise risk estimation. Thirteen case-control studies included 1025 cases and 2566 controls. In the present study, we found that the ALDH2*2 allele is associated with ALC; individuals with the ALDH2*2/*2 and/or *1/*2 genotype had a lower risk of developing ALC compared to individuals with the ALDH2*/1*1 genotype. The results of our meta-analysis seem to contradict the observations of functional studies of ALDH2, which had suggested that ALDH2 played an important role in the development of ALC. This inconsistency might partly be explained by the fact that ALDH2*1/*2 and *2/*2 subjects with high blood acetaldehyde levels after alcohol consumption could develop intense facial flushing responses with nausea, headache, drowsiness and so on.36 This unpleasant discomfort may prevent people from consuming alcohol and may keep them from developing alcoholism, so that they have much smaller chance to expose to the acetaldehyde, and then decrease the risk of developing ALC.37 In addition, a previous study examined the lifetime drinking history of alcoholics, and the results showed that the ALDH2*1/*1 group experienced the onset of each event in their drinking history, including the onset of habitual, excessive, binge drinking, and alcohol dependence, earlier in life than the ALDH2*1/*2 group.38 Although reactive acetaldehyde is a candidate for the causal agent of the organ injuries in alcoholics, the increased peak blood acetaldehyde levels of alcoholics was found to be inversely correlated with the depressed hepatic ALDH activity.39 Yokoyama, et al.40 found that the levels of blood acetaldehyde in the active ALDH2*1/*1 alcoholics, are comparable with the levels of the inactive heterozygous ALDH2*1/*2 alcoholics with less active ADH1B*1/*1.
In this study, we did not detect a significant publication bias in this meta-analysis, confirming the reliability of our results. As for the heterogeneity, no significant heterogeneity was found in overall comparison, when stratified by country; the heterogeneity was partly decreased or removed among Korean and Chinese populations. However, heterogeneity existed in Japanese population. The above results suggest that the ethnic background might be the source of heterogeneity.
Some limitations should be addressed when explaining the results. First, only published studies were retrieved, publication bias might be possible. Second, our results were based on unadjusted estimates, hence the effect estimates were relatively imprecise. In addition, all studies were conducted in Japan, Korea, and China, which may generate selective bias. More studies focused on other Asians are needed.
In conclusion, the results of this meta-analysis suggest that the ALDH2 polymorphism may be an important protective factor for alcoholic cirrhosis in East Asians.





 XML Download
XML Download