

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nasopharyngeal carcinoma (NPC) is the most commonly diagnosed head and neck malignancy in Southeast Asia, especially in Southern China.12 With the application of intensity modulated radiotherapy (IMRT), the loco-regional control of NPC has been improved dramatically.345 Nevertheless, distant metastasis (DM) remains as the main failure pattern,6789 with the DM rate estimated at approximately 20–30%.4510 Bone metastasis is one of most common metastatic sites of NPC.8
Several studies have reported on treatment outcomes of NPC with bone metastasis, either for patients with bone metastases at primary diagnosis or with recurrent bone disease after definitive chemoradiotherapy (CRT). Therein, the median overall metastasis survival (OMS) time is reported to be 12–23.5 months.111213 These data indicate that bone metastasis patients may differ greatly in terms of survival; however, methods have not yet to be developed for evaluating prognoses and stratifying these patients into different risk groups before treatment, especially those with bone-only metastasis after definitive CRT.
In this retrospective study, we analyzed 80 NPC patients with bone-only metastasis after radical CRT in an attempt to investigate the prognostic factors affecting survival of this subgroup of patients and to stratify patients into different risk groups based on the presence of risk factors before re-treatment.
MATERIALS AND METHODS
Patients and data collection
Between October 2005 and December 2010, a total of 2139 histologically proven NPC patients without DM were treated by definitive radiotherapy with or without chemotherapy at our institution, either two-dimensional radiotherapy (2D-RT) or three-dimensional conformal radiotherapy/IMRT. At time of censorship, a total of 171 patients developed bone metastasis, with or without local-regional recurrence and distant failure at other sites. Among them, 80 patients with bone-only metastasis were retrospectively analyzed in this study, excluding 52 patients with local-regional recurrence and/or co-existed with other types of metastases and another 39 bone metastases patients who had not received any treatment.
Bone-only metastasis was defined as only bone-type metastasis without non-skeletal metastasis at the time of their initial diagnosis of metastatic NPC. Bone metastasis was diagnosed based on the presence of symptoms and imaging checks, including bone scan, computed tomography (CT), magnetic resonance imaging, or positron emission tomography. All patients were restaged according to the 7th edition of American Joint Committee on Cancer. The median metastases free interval (MFI) was defined as the interval between the date of the first consultation and the date of first diagnosis with DM. Solitary bone metastasis was defined as a single site bone lesion within a two month period after diagnosis of bone metastasis. Multiple-site bone metastasis comprised two or more sites of bone metastasis. Serum lactic dehydrogenase (S-LDH) and serum alkaline phosphatase (S-ALP) before treatment were estimated employing the optimized standard method recommended by the German Society of Clinical Chemistry.14 S-LDH >245 IU/L and S-ALP >110 IU/L were considered a sign of high levels thereof. Hemoglobin (Hb) levels <11.0 g/dL were considered to indicate anemia according to World Health Organization standards for cancer patients.15
Treatment of bone metastases
Of the 80 patients, 48 received combined chemotherapy and palliative radiation of the bone, while 10 and 22 patients underwent chemotherapy alone and palliative radiotherapy alone, respectively. Palliative radiation comprised long course radiotherapy (39 patients with 2D-RT and 21 patients with IMRT), with a median dose of radiation of 30 Gy (range 30–66 Gy). Among patients who underwent palliative radiotherapy, most of them (40 patients) underwent 30 Gy irradiation in 10 fractions; 20 patients received a dose of 36–45 Gy (2–2.5 Gy/fraction); and the remaining 10 patients received 46–66 Gy irradiation (2 Gy/fraction) for non-spine metastasis sites.
In total, 58 patients underwent platinum-based chemotherapy (range 1–8 cycles; median: 3 cycles). Forty-three patients received platinum plus gemcitabine, and the other 15 patients used platinum plus paclitaxel. In our series, 64 patients also underwent bisphosphonate therapy, ranging from one to six cycles (median: 2 cycles).
Follow-up and statistical analyses
Patients were evaluated for response every two cycles during systemic chemotherapy and then every three months until death, based on CT or isotopic bone scan. OMS was measured and calculated from the first day of diagnosis of bone metastasis to the date of death or final follow up. Survival data were analyzed with SPSS software, version 18.0 (SPSS Inc., Chicago, IL, USA). Survival curves were created with the Kaplan-Meier method and compared with the log-rank test. Multivariate analyses were performed to test the independent significance of potential prognostic factors by a Cox proportional hazards model. Two-tailed p-values ≤0.05 were considered statistically significant.
RESULTS
Patients characteristics
Sixty-two of the 80 patients developed bone metastasis in the first two years after diagnosis of a primary tumor. The median MFI was 15 months (ranging 3 to 66 months). Twenty-seven and 53 patients presented with solitary and multiple bone metastases, respectively. Other clinical characteristics of the patients enrolled are listed in Table 1.
The median follow-up period after the diagnosis of bone metastasis for the entire cohort was 15.5 months (range, 2–63 months).
Survival
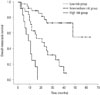
Thirty-nine patients had expired at the time of analysis, with a median OMS time and a 2-year estimate OMS rate to be- 26.5 months and 52%, respectively (Fig. 1A). In particular, patients with CRT had a median overall metastases survival of 40.0 months, which was significant longer than that of patients treated with radiotherapy alone (17.4 months) (p=0.043) or chemotherapy alone (12.6 months) (p=0.018). However, the difference in median OMS time between patients in the chemotherapy alone group and the radiotherapy alone group showed no statistical significance (p=0.570) (Fig. 1B).
Univariate and multivariate analysis
Potential prognostic factors, including patient factors [gender, age, Karnofsky Performance Status at diagnosis of bone metastasis], disease factors (clinical stage, number of bone metastases sites, bone metastasis sites, and MFI), laboratory factors [Hb level, albumin level (ALB), S-LDH, and S-ALP] and treatment factors (chemotherapy, radiotherapy, bisphosphonates) were analyzed by the log-rank test, as shown in Table 2. In additiona to treatment modality, log-rank test indicated that multiple bone metastases, MFI ≤12 months, Hb <11.0 g/dL, ALB <40 g/L, and S-LDH ≥245 IU/L were associated with poorer OMS.
Multivariable analysis showed that treatment modality, MFI, number of metastases sites, and S-LDH level remained as significant predictors for OMS. However, Hb and ALB failed to enter the final Cox model, as shown in Table 2.
Prognostic evaluation and risk groups
In order to evaluate the prognosis of patients with bone-only metastasis, all included patients were stratified into three different risk groups based on the presence of the independently significant prognostic factors (MFI, number of metastases sites, and S-LDH level), except treatment modality, as follows: group A (without any adverse factor or with only one factor), low-risk group; group B (with two adverse prognostic factors), intermediate-risk group; and group C (with three adverse prognostic factors), high-risk group. There were 42, 26, and 12 patients in these three groups, respectively.
As shown in Fig. 2, the OMS curves for the risk groups were significantly different (p<0.001). All patients in group C had expired within two years. The 2-year estimate OMS rates of group A, B, and C were 75.3%, 39.9%, and 0%, respectively, with the median OMS time of groups B and C to be 21 and 9 months, respectively. The median OMS time of group A could not be estimated, because the follow-up time of this group was not long enough and most patients were still alive.
DISCUSSION
DM has heterogeneity, as different metastatic characteristics show different prognoses.8 Bone metastasis is one of the predominant failure sites of NPC, the treatment outcome of which is far from satisfactory.8111213 Our series indicated a median OMS time of 26.5 months, with a 2-year OMS rate of 52%. Multivariate analysis identified MFI, numbers of bone metastasis, S-LDH level, and treatment modality as significant prognosticators. According to the presence of three independent predicting factors, except treatment modality, patients can be well stratified into three different risk groups, with OMS curves significantly different from each other.
Several studies have evaluated the survival and prognostic factors of NPC patients with bone metastasis.11121316 A recent report from China indicated a median OMS of 12 months, in which 70 NPC patients with bone metastasis at their first visit were enrolled.12 Among them, 29 co-existed with other metastatic sites, including lung and/or liver, althgouh no further prognostic analysis were performed in this series.12 Another Chinese study by Jin, et al.11 demonstrated that patients who received zoledronic acid (ZA) combined with chemotherapy had significant longer median OMS (23.5 months) than those who received chemotherapy alone (17.5 months). In their study, a total of 307 cases were included, and bone metastasis was diagnosed either at the time of the first visit or during the follow-up time after definitive treatment; patients with other types of DM were included as well.11 Besides ZA, chemotherapy cycles, vertebral metastases, serum ALP level, and skeletal-related events were found to be significant prognostic factors for OMS in multivariate analysis.11 Recently, analysis of a relatively large sample of 312 NPC patients with an initial diagnosis or developing bone-only metastasis during follow-up time found CRT, number of bone metastasis, and spine metastasis to be prognostic factors. The median OMS thereof was 23.4 months.13 The only other study to evaluate the survival of NPC patients who developed bone-only metastasis after radical treatment was initiated by Cao, et al.16 in 116 cases. They indicated that CRT, age, local recurrence, subsequent metastasis, and disease free interval (DFI) were independent predicting factors for OS; the median OS time was 33.3 months.16 Using a different and more objective endpoint, the present study estimated a median OMS time of 26.5 months, which was comparable to that reported by Li, et al.13 Also, the patients enrolled in our study were similar to those in Cao, et al.16 Our Cox model indicated that MFI (similar to DFI in Cao, et al.'s study), treatment modality, S-LDH, and numbers of metastasis sites were independent factors that significantly affected treatment outcomes.
Our series indicated that patients could benefit, in terms of survival, from combined treatment, which is consistent with the results reported by Cao, et al.16 and Li, et al.,13 who suggested that chemotherapy or radiotherapy alone is not sufficient to control metastatic tumors. We recommended that long-course radiotherapy could be better, as has been demonstrated by Hartsell, et al.17 and Howell, et al.18 Compared with single fraction radiotherapy, long-course radiotherapy could reduce retreatment rates. In our cohort, at least one cycle of bisphosphonate was used in about 80% patients, although no survival benefit was indicated. This result concurred closely with that noted in Li, et al.13 However, Jin, et al.11 found that bisphosphonate could improve OMS in NPC patients with bone metastasis. A possible reason for this inconsistency may be associated with different immune microenvironments.19 Zhang, et al.20 showed that T-cell deficiency reduces the antitumor effects of bisphosphonate, compared with immune-competent mice, in animals with bone metastases.
As have been reported in other studies,132122 we also found that multiple-bone metastases was an adverse prognostic factor of survival. Elevated S-LDH is frequently observed in cancer patients, which could be attributed to the release of enzymes from malignant cells.23 Patients with abnormally elevated S-LDH had significantly worse treatment outcome than those with normal S-LDH level. Other investigators have also identified that elevated S-LDH is associated with poor prognosis in metastatic and loco-regionally advanced NPC.2425 Another independent predicting factor was MFI. Patients with MFI ≤12 months were associated with poor survival, and similar results have also been presented in other reports.81626 The possible reason could lie in emerging chemotherapy or radiotherapy resistant clones within the tumor of those patients who developed DM in a short time after treatment.
In order to evaluate the prognosis of patients with bone-only metastasis, these patients were stratified into three different risk groups, with the 2-year estimate OMS rates for low, intermediate, and high risk groupto at 75.3%, 39.9%, and 0% (p<0.001). All 12 patients in the high risk group were deceased with in the first two years. Among them, seven received CRT; patients who underwent CRT showed relative higher OMS than those who received chemotherapy or radiotherapy alone, although the difference showed no statistical significance (data no shown). Considering the unfortunate results of the high-risk group, management should aim to improve end-stage quality of life, and more efficient systematic treatment (i.e., immune treatment) may need to be introduced and evaluated in multicenter studies. For those in the low and intermediate risk groups, more aggressive treatment (i.e., combined CRT) should be considered.
Several limitations should be addressed for our series. First is the retrospective nature of the study. Secondly, our results were concluded from a relatively small sample from a single institution (80 cases); however, they were derived from 2139 patients treated over 2005 and 2010. Accordingly, our results should be validated in a relatively large group of patients collected from multiple centers. Thirdly, the modes of chemotherapy and radiotherapy used in our series varied, which might have had a confounding effect. Finally, the present study did not report the incidence of skeletal-related events, as not all the patients had regular follow-up and it was difficult to obtain such information in patients who had died at the time of censorship.
Our results indicated that multiple bone metastases, short MFI, high level S-LDH, and RT or CT alone are associated with short metastasis survival. Different prognostic factors were associated with different outcomes for patients who developed bone-only metastasis after primary treatment. Grouping patients according to the presence of these risk factors could well distinguish patients with different outcomes. Considering it was convenient and efficient, clinicians could use the number of adverse prognostic factors present to evaluate the prognosis of these patients. From both a therapeutic and research point of view, our prognostic grouping may be helpful in improving the design of clinical trials involving NPC patients with bone-only metastasis and in guiding individualized treatment.



 XML Download
XML Download