

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thymic hyperplasia is frequently accompanied by Graves' disease. In 38% of patients with Graves' disease, histologic abnormalities in the thymus were present.1 However, thymic enlargement is minimal in most cases, and detectable massive enlargement of the thymus has been described in only a small number of case reports.2,3,4 To the best of our knowledge, there are no reports demonstrating dynamic changes in thymic size (decreasing and increasing repetitively) proportional to Graves' disease activity. Furthermore, the pathophysiological mechanisms of such changes in thymic hyperplasia have remained incompletely described.
CASE REPORT
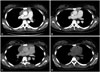
A 22-year-old woman diagnosed with Graves' disease was admitted, as an X-ray had incidentally detected mediastinal widening. A chest computed tomography (CT) scan showed a 7.6×2.0×7.7 cm [maximum cross-sectional area (MCSA) 1265.14 mm2] thymic enlargement (Fig. 1A). Fluorine-18 fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) results indicated that 18F-FDG uptake in the thymus was increased and heterogeneous. Therefore, the patient underwent a CT-guided needle biopsy due to our concern for possible thymoma; however, the pathologic results revealed non-neoplastic thymic tissue. The patient was treated with methimazole 15 mg/day. Her thyroid functions, measured using a radioimmunoassay kit (RIAKEY, Shin Jin Medics Inc., Goyang, Korea), were as follows: free thyroxine (T4), 1.02 ng/dL (reference range 0.70–1.80 ng/dL); total triiodothyronine (T3), 109 ng/dL (reference range 87–184 ng/dL); and thyrotropin (TSH), 0.22 µIU/mL (reference range 0.40–4.10 µIU/mL). Her serum thyrotropin binding inhibiting immunoglobulin (TBII) titer was not determined (Table 1, visit #1). After 1 year, laboratory testing indicated poorly controlled hyperthyroidism; the patient had shown poor compliance with antithyroid medication. Serum TBII, measured as serum thyrotropin receptor (TSH-R) antibodies by using a first-generation porcine radioreceptor kit (RSR, Cardiff, UK), was 31.4% (reference range <15%). Therefore, we prescribed methimazole at an increased dose of 20 mg/day (visit #2). After 20 months at this antithyroid drug increment, the serum thyroid hormone levels and TBII were approximately normalized (Table 1, visit #3), and the size of the thymus had decreased to 6.9×1.0×6.0 cm (MCSA 359.12 mm2) in a follow-up CT scan (Fig. 1B). Subsequent to visit #3, she discontinued the antithyroid medication for over 1 year against medical advice and developed thyrotoxic symptoms including sweating and weight loss. Laboratory results obtained at 54 months after the initial visit were as follows: free T4, 4.88 ng/dL (reference range 0.70–1.80 ng/dL); total T3, 282 ng/dL (reference range 87–184 ng/dL); and TSH, <0.05 µIU/mL (reference range 0.40–4.10 µIU/mL). The TBII level, measured using a second-generation recombinant human radioreceptor kit (BRAHMS, Berlin, Germany), was 14.7 IU/L (reference range 0–1.0 IU/L) (Table 1, visit #4). The patient's antithyroid medication was restarted at a methimazole dose of 30 mg/day. Nevertheless, hyperthyroidism remained present after 9 months of therapy (Table 1, visit #5). The size of the thymic hyperplasia increased again and measured 9.8×3.2×9.5 cm (MCSA 1759.58 mm2) in a CT scan (Fig. 1C). For treatment of Grave's disease refractory to the antithyroid medication, the patient underwent a total thyroidectomy after visit #5, as she preferred surgery to radioactive iodine therapy. She started to take 0.1 mg/day of levothyroxine as a thyroid hormone replacement yet took the medicine irregularly. Six months after surgery, thyroid function tests indicated that she was in a hypothyroid state, and the TBII level was not checked at that time (Table 1, visit #6). A CT scan revealed marked shrinkage of the thymus to 6.2×1.0×6.0 cm (MCSA 305.47 mm2) (Fig. 1D). She was advised to take levothyroxine regularly. Eighteen months after surgery, laboratory tests revealed a free T4 level of 1.11 ng/dL (reference range 0.70–1.80 ng/dL), a total T3 level of 130 ng/dL (reference range 87–184 ng/dL), a TSH level of 6.73 µIU/mL (reference range 0.40–4.10 µIU/mL), and a decreased TBII level of 0.9 IU/L (BRAHMS, Berlin, Germany; reference range 0–1.0 IU/L) (Table 1, visit #7).
We performed an immunohistochemical study using the goat polyclonal antibodies for TSH-R (Santa Cruz Biotechnology, Santa Cruz, CA, USA) on the patient's thyroid and thymic tissue samples and on the thymic tissue of a person without Graves' disease as a negative control (Fig. 2). The patient's thyroid and thymic tissues showed positive TSH-R results. The follicular epithelial cells of her thyroid showed weakly positive staining results (Fig. 2A). In her thymus, the medullary portion of the thymic lobules was predominantly stained by antibodies for TSH-R (Fig. 2B). Furthermore, TSH-R expression was observed in Hassall's corpuscles and epithelial reticular cells rather than in lymphocytes (Fig. 2C). In contrast, the thymic tissue of the person without Graves' disease was negative for TSH-R (Fig. 2D).
DISCUSSION
The mechanisms that produce thymic hyperplasia in Graves' disease are not well established. The first possible mechanism is that the presence of TSH-R in the thymus may produce an autoimmune response and lead to thymic hyperplasia, as it has been reported that TSH-R in the orbit and fibroblasts results in Graves' ophthalmopathy and dermopathy.5 Murakami, et al.6 identified the presence of TSH-R in non-neoplastic thymic tissues obtained from non-thyroidal disease patients. In the present case, we firstly demonstrated TSH-R expression in a Graves' patient who presented with thymic hyperplasia, thus supporting the first possible mechanism. Moreover, the patient's TSH-R antibody titer was elevated in the presence of thymic hyperplasia and declined at the time of thymic regression.
A second possible mechanism is that thyroid hormone excess may induce thymic hyperplasia. In experimental animal studies, thymus enlargement after the administration of a thyroid hormone7 and regression after thyroidectomy8 have been demonstrated. Levels of thymulin, a thymic hormone that enhances differentiation and proliferation of T-lymphocytes, have been reported to be higher in patients with hyperthyroidism and lower in patients with hypothyroidism compared to levels in normal subjects.9 These results suggest that thyroid hormones can affect thymic endocrine function and the development of lymphoid hyperplasia. In our case, however, normal levels of total T3 and free T4 at the subject's initial visit (Fig. 1A) do not support this second possible mechanism.
With regard to management for thymic hyperplasia in Graves' disease, current recommendations are to treat for hyperthyroidism with close monitoring radiologically and to delay invasive intervention.3,10 In general, immediate thymic biopsy for diagnosis is not recommended; however, in the present case, we performed needle biopsy due to the suspect results obtained by PET. After confirming the presence of benign thymic tissue, the patient was advised to take an antithyroid drug. In a follow-up CT scan, the patient's thymic hyperplasia had nearly disappeared.
Dynamic changes in thymic hyperplasia proportional to Graves' disease activity and the presence of TSH-R in the thymus of a Graves' patient with dynamic thymic changes were observed in the subject of this case report. Clinicians should be aware of the association between thymic hyperplasia and Graves' disease to avoid unnecessary invasive investigations.


 XML Download
XML Download