

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Season of birth (SOB) can reflect a particular early life environ- ment during gestation and the first months or year of life, and can influence subsequent traits and disease risks.123 Despite the absence of any clear understanding of the biological underpinnings, day length, seasonal changes in maternal nutritional status and vitamin D levels, and seasonal alterations in the incidence of some common infectious disorders have been seen as associated with SOB.4 Some chronobiological studies have suggested that SOB can have an impact on the later development of several psychiatric disorders including schizophrenia,5 bipolar disorder,6 suicide,2 obsessive-compulsive disorder,7 eating disorder,8 personality features,9 and smoking.10
Depressive disorders have been an important issue in a realm of mental health globally.11121314 Since depressive disorder is a complex disease, due to both genetic and environmental factors,15 it would be useful to investigate any association between SOB and the epidemiological and clinical characteristics of depressive disorder. To our knowledge, the effect of SOB on depressive disorder has little been studied. In a preliminary study of 45 patients with major depressive disorder (MDD), Fountoulakis, et al.16 found a tendency for spring-born patients to have the greater severity of depression whereas summer-born patients had a higher level of anxiety, although statistical significance was not evaluated. Most MDD patients who failed to respond to the 1 mg dexamethasone suppression test were born during the autumn/winter. More specifically, in a study of 553 outpatients with winter-type seasonal depressive disorder, individuals with melancholic depression were more often born in autumn/winter, whereas those with atypical depression were more often born in spring/summer. In addition, seasonal affective disorder has been shown to peak in May.17 However, differences in SOB patterns between depressed patients and controls have been paradoxical.1618 In addition, in a large sample of suicide completers from Hungary, Döme, et al.2 found a significant association between SOB and risk of completed suicide. Thus, using the comprehensive data from a cohort study of Korean patients with depressive disorders, we aimed to analyze the distribution and potential clinical correlates of SOB in patients with unipolar non-psychotic MDD.
As described elsewhere,11 the Clinical Research Center for Depression (CRESCEND) study was the first, largest, clinical study of a nationwide sample of patients with depressive disorders in Korea. In the CRESCEND study, from January 2006 to August 2008, 1183 patients beginning psychiatric treatment for first-onset or recurrent depressive disorder were recruited from 18 centers (16 university-affiliated hospitals and 2 general hospitals) in Korea. The Relevant Institutional Review Boards of all the centers approved the protocol and consent forms of the study (receipt number: CUMC07U001). All the subjects gave written informed consent before the start of the study.
Our inclusion criteria were as follows: 1) age ≥18 years and ≤80 years, 2) diagnosis of unipolar non-psychotic MDD according to the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV),19 confirmed by a Structural Clinical Interview based on DSM-IV (SCID),20 3) total score on the Hamilton Depression Rating Scale (HAMD)21 ≥8 points, by the severity classification of Zimmerman, et al.,22 and 4) availability of definite SOB. Patients with diagnoses of psychotic MDD, dysthymic disorder, or depressive disorder not otherwise specified, were excluded to enhance the homogeneity of study subjects. Finally, 891 patients with non-psychotic MDD were enrolled.
Based on the daily duration of sunshine in Seoul, South Korea (127° 00' eastern longitude and 37° 06' northern latitude), seasons were defined as follows: spring, March to May, summer, June to August, autumn, September to November, and winter, December to February. Using the definitions of Fountoulakis, et al.16 and Pjrek, et al.18 SOB was encoded as a dichotomous variable including spring/summer- and autumn/winter-births.
Based on the definitions of major depressive episode (DSM-IV),19 the presence/absence of each depressive symptom (depressive mood, markedly diminished pleasure, weight gain or loss, insomnia or hypersomnia, psychomotor retardation or agitation, fatigue or loss of energy, feelings of worthlessness, diminished concentration, and suicidal ideation) was evaluated. The presence/absence of specific MDD symptoms were determined from the SCID.20
In addition, the HAMD,21 Hamilton Anxiety Rating Scale (HAMA),23 Brief Psychiatric Rating Scale (BPRS),24 Scale for Suicidal Ideation (SSI-Beck),25 Clinical Global Impression of severity (CGI-S),26 Social and Occupation Functional Assessment Scale (SOFAS),27 WHO Quality of Life assessment instrument-abbreviated version (WHOQOL-BREF),28 Alcohol Use Disorder Identification Test (AUDIT),29 and Temperament and Character Inventory (TCI)30 were used to evaluate depression, anxiety, overall symptoms, suicidal ideation, global severity, social function, quality of life, drinking, and temperament and character, respectively. Each of the scales had been formally translated into Korean and its psychometric validity had been clearly confirmed in the Korean population.31323334353637 More severe symptoms or greater illness burden were indicated by higher scores on the HAMD, HAMA, BPRS, SSI-Beck, CGI-S, and AUDIT, and lower scores on the SOFAS and WHOQOL-BREF.
Using independent t-tests for continuous variables and χ2 tests for discrete variables, we compared the demographic and clinical characteristics of non-psychotic MDD patients with spring/summer versus autumn/winter births. Statistical significance was set at p<0.05 (two-tailed). All the statistical analyses were performed with SPSS 21 for Windows (SPSS Inc., Chicago, IL, USA).
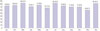
As shown in Table 1, the mean age of all subjects was 48.5 (SD=15.0) years. Most were women (76.2%), employed (74.9%), ever married (85.2%), and enrolled as outpatients (77.9%). About half were religiously affiliated (61.8%) and had a monthly income >2000 USD (52.5%). As shown in Fig. 1, the number (percent) of births in individual months ranged from 60 (6.7%; November) to 84 (9.4%; March). With respect to SOB, the number (percent) of subjects born in each season were 233 (25.8%) in spring, 234 (25.8%) in summer, 214 (24.3%) in autumn, and 214 (24.3%) in winter.
As shown in Table 1, there were no significant differences in age (t=-0.307, p=0.759), gender (χ2=0.111, p=0.739), employment (χ2=0.396, p=0.529), marriage (χ2=0.060, p=0.807), education (t=-0.673, p=0.501), religious affiliation (χ2=0.219, p=0.501), outpatient enrollment (χ2=0.028, p=0.866), and season when psychiatric treatment sorted (χ2=3.107, p=0.375) between MDD patients with spring/summer versus autumn/winter births. As shown in Table 2, MDD patients born in spring/summer were significantly younger at onset of first depressive episode (t=2.084, p=0.038), had diminished concentration (χ2=4.589, p=0.032), and higher scores on the self-directedness dimension of the TCI (t=2.256, p=0.025) than those born in autumn/winter. However, there were no significant differences in season when psychiatric treatment sorted (χ2=3.107, p=0.375), history of suicidal attempts (χ2=1.263, p=0.261), medical comorbidity (χ2=0.499, p=0.480), atypical features (χ2=0.230, p=0.632), HAMD (t=-0.184, p=0.854), HAMA (t=1.452, p=0.147), BPRS (t=-0.695, p=0.488), SSI-Beck (t=-0.031, p=0.975), CGI-S (t=0.007, p=0.995), SOFAS (t=0.067, p=0.946), WHOQOL-BREF (t=0.986, p=0.324), AUDIT (t=0.462, p=0.645), and the other characteristics between the two groups.
According to our data, spring/summer birth among MDD patients is associated with younger age at onset and more diminished concentration. In MDD, younger age at onset may be a potential predictive indicator of more severe clinical course.38394041 In 80 patients with MDD and comorbid alcohol dependence, younger age of onset of the first major depressive episode was associated with response to escitalopram treatment.38 In 1970 Han Chinese women with MDD, younger age of onset was associated with longer duration of illness, more MDD episodes, longer index episode, and higher comorbidity of anxiety disorders.39 In 4041 MDD patients who participated in the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, younger age at onset was related to poorer social and occupational function, higher medical and psychiatric comorbidity, and more lifetime depressive episodes and suicide attempts.40 Furthermore, in a sample of 1104 patients with current MDD in the Netherlands Study of Depression and Anxiety (NESDA),42 a greater loss of concentration was seen in subjects with early age at onset (<40 years) than in those with late age at onset (>40 years). In addition, diminished concentration was associated with a history of attempted suicide in 1970 Chinese women with recurrent MDD,43 and with vascular comorbidities in 39 older-elderly Taiwanese men with MDD.44 To our knowledge, our study is the first to report a link between spring/summer birth, younger onset of first major depressive episode, and diminished concentration in MDD patients. Hence, we may speculate that, in MDD patients, birth in the spring or summer may not only be an intervening variable between younger age at onset and diminished concentration, but also a potential indicator of greater illness burden.
In contrast, the potential positive relationship between self-directedness and birth in the spring or summer may suggest that MDD patients with spring/summer birth are associated with less illness burden than those with autumn/winter birth. The justifications for this idea are that: lower score on the self-directedness of the TCI has been associated with a shorter time to recurrence from remission in 69 MDD patients over a 4-year prospective follow-up,45 with a higher rate of future dysphoric episodes in a cohort of the general population,46 and with greater severity of depressive symptoms in the Young Finns Study.47 The contradictory trends of the clinical features of MDD patients associated with spring/summer birth cannot be simply explained. Based on the links between polymorphism in the serotonin transporter-linked polymorphic region (5-HTTLPR) and age at onset, and between 5-HTTLPR polymorphism and self-directedness,4849 we may surmise that the contradictory trends are partly connected with the actions of 5-HT. 5-HT has paradoxical effects of the following kinds: functional impairment of anterior 5-HT cells (dorsal raphe nucleus) can result in sensitization of the dopamine system leading to impulsivity and addiction, whereas functional impairment of posterior 5-HT cells (median raphe nucleus) innervating the hippocampus and cingulated gyrus, can result in melancholic mood, low self-esteem, and hopelessness.50 Further study of a possible association between the 5-HT system, e.g., 5-HTTLPR polymorphism, and SOB, could clarify the origin of the mixed features of MDD patients with spring/summer birth.
There are several limitations to our study. First, it was not possible to identify an MDD-specific SOB pattern by means of a comparison with controls, since no controls were enrolled. Second, the familywise error rate due to multiple comparisons may have been significant, since we did not use Bonferroni's correction. Thirdly, since the seasonal type of MDD was not subcategorized, differences between seasonal and non-seasonal types could not be detected. Despite these limitations, to our knowledge, our study has the virtue of pioneering the study of a possible relationship between SOB and clinical features in MDD. In conclusion, unipolar non-psychotic MDD patients with spring/summer birth tended to be younger at onset, have more severely diminished concentration, and higher scores on self-directedness in the TCI. Clinically, there was a trend for the MDD patients born in spring/summer to display the contradictory characteristics of more severe clinical course and less illness burden; this may have been partly due to a paradoxical effect of the 5-HT system.


 XML Download
XML Download