

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatitis A virus (HAV) is a non-enveloped, single-stranded RNA virus of the Picornaviridae family.1 HAV infection is often asymptomatic in children. However, HAV infection in adults tends to result in acute hepatitis, called acute hepatitis A (AHA), one of the most common forms of acute viral hepatitis.234 In adult patients with AHA, severe liver injury and jaundice frequently develop and last for several weeks. However, AHA resolves spontaneously in most cases and does not progress to chronic viral hepatitis.5
Hepatitis B virus (HBV) is a partly double-stranded DNA virus that belongs to the Hepadnaviridae family.6 HBV infection is the most common form of chronic viral infection in the world, with more than 350 million people chronically infected.7 In endemic areas, chronic HBV infection is often established by vertical transmission.8 In adults, acute HBV infection causes acute hepatitis B (AHB), which is accompanied by liver injury and jaundice.89 Although AHB resolves spontaneously in most adult patients, some cases (1–5%) progress to chronic persistent infection.89
In both AHA and AHB, liver injury is known to be caused by T cells, not by the virus, because both HAV and HBV are non-cytopathic viruses.91011 Immune-mediated tissue injury, so-called immunopathology, is mediated by diverse mechanisms in different viral infections.12 The inflammatory process is mediated by cytokines, including interleukin (IL)-1β, IL-6, and tumor necrosis factor-α (TNF-α), and it is suppressed by IL-10.12 Additionally, helper 1 T (Th1) cells and helper 17 T (Th17) cells contribute to tissue injury by secreting cytokines; e.g., Th1 cells secrete interferon (IFN)-γ and TNF-α, and Th17 cells secrete IL-17 and IL-21.13 Moreover, cytotoxic T cells and natural killer (NK) cells directly lyse host cells through perforin/granzyme, and Fas ligand-mediated mechanisms.14 Chemokines are also involved in immune-mediated tissue injury by recruiting immune cells to the site of a viral infection.1516 However, in AHA and AHB, the exact mechanisms of immune-mediated liver injury remain to be elucidated.
In this study, we measured serum levels of 17 cytokines and T-cell cytotoxic proteins in patients with AHA and AHB in the acute phase to understand immunological mechanisms of liver injury in acute viral hepatitis, and identified cytokines or T-cell cytotoxic proteins associated with severe liver injury in AHA and AHB. The present study provides insight regarding which effector function of T cells contributes to liver injury in AHA and AHB.
MATERIALS AND METHODS
Study participants
Forty-six patients with AHA, 16 patients with AHB, and 14 healthy adults were recruited from hospitals in the Seoul metropolitan area (Seoul National University Bundang Hospital, Chung-Ang University Hospital, Bundang CHA Hospital, Seongnam Central Hospital, and Daejin Medical Center). AHA and AHB were diagnosed based on positive detection with anti-HAV IgM, and HBsAg and anti-HBc IgM, respectively, typical disease symptoms, and elevated serum alanine aminotransferase (ALT) levels. Peak ALT level and peak total bilirubin level were determined for each patient during the course of acute hepatitis. We obtained informed consent from participating subjects and study approval from the Institutional Review Boards. At the time of hospital admission, blood was drawn from patients, and serum samples were frozen for later analysis.
Analysis of serum cytokines
Eleven cytokines: IL-1β, IL-6, IL-10, IL-12p70, IL-18, IL-21, IL-22, IL-28, IL-29, IFN-γ, and TNF-α; and four chemokines: IL-8, CCL2 (monocyte chemoattractant protein-1), CXCL9 (monokine induced by IFN-γ), and CXCL10 (IFN-γ-inducible protein-10) were measured in this study. We also analyzed the serum levels of T-cell cytotoxic proteins, including granzyme B and soluble Fas ligand (sFasL). The serum levels of these proteins were measured with either enzyme-linked immunosorbent assay (ELISA) kits (IL-18, Abcam, Cambridge, UK; IL-22, R&D Systems, Minneapolis, MN, USA; and IL-28 and IL-29, RayBiotech Inc., Norcross, GA, USA) or cytometric bead array flex kits (BD Biosciences, San Jose, CA, USA).
Statistical analysis
Discrete variables were compared using the χ2 method, and independent t tests were used for continuous variables. Pearson or Spearman correlation analysis was used to determine simple correlations between continuous variables. All statistical analyses were performed with Statistical Product and Service Solutions 13.0. (SPSS Inc., Chicago, IL, USA).
RESULTS
General characteristics of enrolled patients
Table 1 shows the demographic and laboratory characteristics of the study population. The median age of the AHA patients, AHB patients, and healthy controls were 33.6, 35.8, and 32.1 years, respectively. The average of peak ALT levels (IU/L) was 4450 in AHA patients and 1406 in AHB patients. The average of peak total bilirubin levels (mg/dL) was 5.1 in AHA patients and 9.6 in AHB patients.
Serum levels of cytokines, chemokines, and T-cell cytotoxic proteins in AHA and AHB
Among the serum proteins analyzed, several were significantly elevated in serum samples from patients with AHA or AHB, compared to serum samples from healthy subjects. IL-18, IL-8, CXCL9, and CXCL10 were significantly elevated in both AHA and AHB, whereas IL-6, IL-22, granzyme B, and sFasL were significantly elevated in AHA, but not in AHB (Fig. 1).
Correlation between the serum levels of CXCR3 chemokines and liver injury
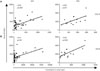
Next, we analyzed which chemokines were associated with the degree of liver injury, assessing liver injury in terms of serum ALT levels. CXCL10 and CXCL9 are CXCR3 chemokines and known to be elevated frequently in systemic viral infections.17 Fig. 2 shows that CXCL10 levels were significantly correlated with peak ALT levels in both AHA and AHB, whereas the serum CXCL9 levels were correlated with peak ALT levels in AHA, but tended to correlate with peak ALT levels in AHB (Fig. 2B).
Correlation between the serum levels of cytokines or T-cell cytotoxic proteins and liver injury
Next, we investigated which cytokines or T-cell cytotoxic proteins were associated with peak ALT levels. In AHA, serum granzyme B, but not serum sFasL, was significantly correlated with peak ALT levels (Fig. 3A). Conversely, in AHB, serum sFasL but not serum granzyme B was significantly correlated with peak ALT levels (Fig. 3B). In addition, the serum IL-18 levels significantly correlated with peak total bilirubin levels in AHA (Fig. 3C) but not in AHB (Fig. 3D). We also analyzed IL-22, a known hepatoprotective cytokine.181920 However, the serum IL-22 levels did not correlate with peak ALT levels in either AHA or AHB (data not shown).
DISCUSSION
In the present study, we found that the serum levels of IL-18, IL-8, CXCL9, and CXCL10 were elevated in AHA and AHB. In addition, the serum levels of IL-6, IL-22, granzyme B and sFasL were increased in AHA but not in AHB, indicating that AHA is accompanied by more vigorous immune responses compared to AHB. The levels of CXCR3 ligands, CXCL10 and CXCL9 correlated with peak ALT levels in AHA and AHB. Moreover, serum granzyme B levels correlated with peak ALT levels in AHA, and serum sFasL levels correlated with peak ALT levels in AHB. These findings together suggest that effector functions of T cells are elevated and contribute to liver injury in AHA and AHB.
CXCR3 and its ligand chemokines regulate the migration of Th1 cells and effector CD8+ T cells into infection sites during various human and murine acute viral infections, such as influenza,21 dengue,22 and West Nile virus infection.23 In viral hepatitis, CXCR3 chemokines have been studied, particularly in hepatitis C virus (HCV) infection. CXCR3 chemokines are detected in the peripheral blood 2–8 weeks after HCV infection.242526 The expression level of CXCR3 chemokines in the liver or the peripheral blood correlated well with the severity of hepatic inflammation in patients with chronic HCV infection.27282930 In ch-ronic HBV infection, it was demonstrated that serum CXCL10 and CXCL9 levels are associated with the acute flare-up of liver injury.31 Consistent with these reports, our data from the sera of AHA and AHB patients demonstrated that CXCR3 chemokines are increased during AHA and AHB, and that their levels correlate with liver damage, thus implying that they might play an important role in liver injury.
Notably, our present data also showed that serum granzyme B levels correlated with peak ALT levels in AHA (Fig. 3A), and that serum sFasL levels correlated with peak ALT levels in AHB (Fig. 3B). The correlation between serum sFasL and serum ALT levels was previously reported in self-limited AHB and fulminant hepatitis B.32 CD8+ cytotoxic T cells and NK cells can contribute to liver injury by target cell-killing activity. When these cells are triggered, they exert cytotoxic activity through two different mechanisms: degranulation of perforin and granzymes, and upregulation of FasL on their cell surface.33 The current findings indicate that a distinct cytotoxic mechanism might contribute to hepatocyte destruction in AHA and AHB.
In the present study, we examined serum levels of cytokines and T-cell cytotoxic proteins to evaluate immune responses during AHA and AHB. However, we did not examine immune cells such as T cells and NK cells, therefore, we do not know yet which subsets of immune cells produce the cytokines and cytotoxic proteins that are increased in the sera of AHA and AHB patients. Future studies should investigate the expression levels of cytokines and cytotoxic proteins in T cells and NK cells obtained from patients with AHA or AHB.
Recently, the levels of multiple serum proteins were systematically analyzed in blood drawn from patients with AHA, AHB, and acute hepatitis C.34 However, that study did not consider the levels of serum proteins relative to the degree of liver injury. In the present study, we compared the associations between liver injury and cytokines, chemokines, and T-cell cytotoxic proteins in AHA and AHB. Our present findings led us to propose that distinct immunological mechanisms of liver injury might operate in AHA and AHB. The exact mechanisms of liver injury require further investigation at the cellular and molecular levels in acute viral hepatitis.



 XML Download
XML Download