

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Non-small cell lung cancer (NSCLC) is the most common type of lung cancer. Until now, the main therapeutic method for NSCLC has been surgical resection with adjuvant chemotherapy, and for patients with unresectable, recurrent, or metastatic tumors, chemotherapy is the predominant treatment method. 1 Unfortunately, the use of traditional chemotherapy in the treatment of NSCLC is greatly limited by primary or secondary multi-drug resistance (MDR).2 MDR, which is defined as a resistance to one drug that is accompanied by a resistance to many other drugs, is believed to be a major reason for the primary drug resistance of NSCLC and can lead to the failure of traditional chemotherapy.34 Therefore, determining how to treat NSCLC patients with primary drug resistance has become an urgent problem. Tyrosine kinase inhibitors targeting epidermal growth factor receptor (EGFR-TKIs) comprise one class of molecular target drugs and have achieved remarkable success in the treatment of patients with NSCLCs bearing activating mutations of EGFR in exons 19 and 21.56 Moreover, these activating EGFR mutations appear more frequently in adenocarcinomas from Asian, female, and non-smoking patients. 78910 Primary drug resistance to EGFR-TKIs still exists in NSCLC patients bearing the activating mutations in exon 2 of the Kirsten rat sarcoma viral oncogene homolog (KRAS) gene.11 Activating mutations in EGFR exons 19 and 21 have been used as biomarkers of NSCLC sensitivity to EGFR-TKIs, while activating mutations in KRAS exon 2 have been used as biomarkers of resistance to EGFR-TKIs. Clinically, many NSCLCs with MDR are well differentiated carcinomas, and well differentiated adenocarcinomas are generally sensitive to EGFR-TKIs. Therefore, it could be hypothesized that some NSCLCs with primary MDR may be sensitive to EGFR-TKIs or, in other words, that NSCLC patients with primary MDR may benefit from EGFR-TKIs. Both P-glycoprotein (P-gp) and lung resistance-related protein (LRP) are drug transporters in cells, and the expression of these factors is often observed in cancers that have developed MDR.41213141516 Recently, the expression levels of these factors have been recognized as major biomarkers of MDR in NSCLC.
In this study, the expression of P-gp and LRP as biomarkers of MDR was detected in NSCLCs by immunohistochemistry, and mutations in EGFR exons 19 and 21 and KRAS exon 2 (as biomarkers of whether the patients can benefit from EGFR-TKIs, respectively) were analyzed by high-resolution melting analysis (HRMA) in 127 NSCLCs. By comparing the expression of P-gp/LRP and EGFR mutation status, we investigated whether patients with NSCLC resistant to traditional chemotherapy would benefit from treatment with EGFR-TKIs.
MATERIALS AND METHODS
Patients and tissue samples
The NSCLC samples were collected from 127 patients who underwent surgical procedures without any traditional chemotherapy or radiotherapy at the affiliated hospitals of Dalian Medical University from July 2007 to May 2009. Seventy-five of these patients were male and 52 were female. The patients had a mean±SD age of 62.1±9.1 years (range 36-80 years); 47 patients had a history of smoking, and 80 patients had no history of smoking. Histologically, the tumor samples consisted of 42 squamous cell carcinomas and 85 adenocarcinomas. Lymph node metastases were found in 64 of the patients. There were 74 patients with well to moderately differentiated tumors and 53 patients with poorly differentiated tumors. All of the tissue samples were collected with the approval of the Ethics Committee of the affiliated hospitals of Dalian Medical University and with the informed consent of the patients or families before the surgical procedures.
Immunohistochemistry
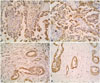
Monoclonal antibodies (Abs) against human P-gp (1:200; clone F4; Sigma-Aldrich Co., LLC, St. Louis, MO, USA) and LRP (1:100; clone 1032; Beijing Golden Bridge Biotechnology Company Ltd., Beijing, China) were used as primary antibodies. Biotin-streptavidin-peroxidase staining with 3, 3'-diaminobenzidine-tetrahydrochloride detection was used. Tumor cells with staining in the cell membrane or cytoplasm were considered to be positive. Each slide was graded blindly according to the percentage of positive tumor cells. The immunoreactivity of P-gp and LRP was scored as negative (-) when the proportion of positive tumor cells was less than 10% or as positive (+) when the number of positive tumor cells was between 10% and 100%.
DNA extraction and gene mutation detection
Tumor-enriched areas were selected and cut from the stained frozen sections that were marked by two pathologists. Genomic DNA was extracted from these areas and purified using the TIANamp Genomic DNA kit according to the manufacturer's protocol (Tiangen, Beijing, China). EGFR exons 19 and 21 and KRAS exon 2 were amplified in triplicate from each sample in a 10-µL reaction volume with a 15-µL mineral oil overlay in each well of a 96-well PCR plate on a Mastercycler thermal cycler (Eppendorf, Hamburg, Germany). The primers were 5'-TG GATCCCAGAAGGTGAGAA-3' and 5'-AGCAGAAACTCACAT CGAGGA-3' (EGFR exon 19); 5'-CGCAGCATGTCAAGATCA-3' and 5'-CCTCCTTACTTTGCCTCC-3' (EGFR exon 21); and 5'-A GGCCTGCTGAAAATGACT-3' and 5'-AATGGTCCTGCACCA GTAA-3' (KRAS exon 2). The reaction conditions were described previously. The mutations were detected with HRMA on a LightScanner® 96 (Biofire Diagnostics, LLC, Salt Lake City, UT, USA). Melting curves were acquired at temperatures ranging from 60℃ to 95℃ and analyzed using LightScanner software (version 2.0, Biofire Diagnostics, LLC, Salt Lake City, UT, USA) according to the manufacturer's instructions.1718
Statistics
Pearson chi-square tests were used to analyze correlations for the expression of P-gp and LRP and mutations in EGFR and KRAS with the clinical and pathological characteristics of the patients; similar tests evaluated the correlation between the expression of P-gp and LRP and mutations in EGFR and KRAS. Statistical significance was defined as p<0.05. Data analysis was performed using the SPSS 11.5 software package (SPSS Inc., Chicago, IL, USA).
RESULTS
P-gp and LRP expressions and their correlations with the clinicopathological characteristics of NSCLC patients
Of the 127 NSCLC samples analyzed by immunohistochemistry, the expression of P-gp was detected in 56 samples, corresponding to a positive expression frequency of 44.1%. LRP was expressed in 84 samples, corresponding to a positive expression frequency of 66.1% of the tested NSCLCs.
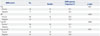
The frequency of positive P-gp expression in patients aged >60 years (52.1%, 37/71) was significantly higher than that in the patients aged ≤60 years (33.9%, 19/56) (p=0.004), and the frequency of positive P-gp expression in non-smokers was 51.3% (41/80), which was significantly higher than that in smokers (31.9%, 15/47) (p=0.034). The frequency of positive P-gp expression in adenocarcinomas was 57.6% (49/85), significantly higher than that in squamous cell carcinomas (16.7%, 7/42) (p=0.000). Significant relationships were observed between protein expression and patient age, smoking history, and tumor histology, but no significant relationships were found with patient gender, tumor differentiation, or lymph node metastasis (Table 1).
The frequency of positive LRP expression in female patients was 80.8% (42/52), significantly higher than that observed in male patients (56.0%, 42/75) (p=0.004), and the frequency of positive LRP expression in non-smokers was 80.0% (64/80), significantly higher than that observed in smokers (42.6%, 20/47) (p=0.000). The frequency of positive LRP expression in adenocarcinomas was 85.9% (73/85), significantly higher than that in squamous cell carcinomas (26.2%, 11/42) (p=0.000). We concluded that significant relationships exist between protein expression and patient gender, smoking history, and tumor histology, but not between protein expression and patient age, tumor differentiation, or lymph node metastasis (Table 1).
EGFR and KRAS mutations detected by HRMA in NSCLC
Of the 127 NSCLC samples analyzed by HRMA, EGFR mutations were detected in 52 samples, corresponding to a mutation frequency of 40.9%; 19 samples contained mutations in exon 19 (Fig. 1) and 33 samples contained mutations in exon 21 (Fig. 2). However, mutations in exon 2 of KRAS were detected in seven samples, corresponding to a mutation frequency of 5.5%.
Correlations between EGFR and KRAS mutations and the clinicopathological characteristics of NSCLC patients
The EGFR mutation frequency in female patients (59.6%, 31/52) was significantly higher than that in male patients (28.0%, 21/75) (p=0.000), and the frequency of EGFR mutations in non-smokers (55.0%, 44/80) was significantly higher than that in smokers (17.0%, 8/47) (p=0.000). The frequency of EGFR mutations in adenocarcinomas was 58.8% (50/85), which was significantly higher than that in squamous cell carcinomas (4.8%, 2/42) (p=0.000); and the frequency of EGFR mutations in well to moderately differentiated tumors (50.0%, 37/74) was significantly higher than that in poorly differentiated tumors (28.3%, 15/53) (p=0.014). We concluded that significant relationships exist between EGFR mutation status and patient gender, smoking history, tumor histology, and degree of differentiation, but not between EGFR mutation status and patient age or lymph node metastasis (Table 2).
The KRAS mutation frequency in male patients was 9.3% (7/75), significantly higher than that in female patients (0.0%, 0/52) (p=0.041). We concluded that a significant relationship exists between KRAS mutation status and patient gender, but not between KRAS mutation status and patient age, smoking history, lymph node metastasis, histological type, or differentiation (Table 2).
Correlations of P-gp and LRP expression with EGFR mutation
The EGFR mutation frequency in P-gp-positive samples was 57.1% (32/56); this was significantly higher than that in the P-gp-negative samples (28.2%, 20/71) (p=0.001). The EGFR mutation frequency in the LRP-positive samples was 53.6% (45/84), significantly higher than that in the LRP-negative samples (16.3%, 7/43) (p=0.000). We then selected samples that were positive for P-gp or LRP and analyzed the correlation between the expression in these samples and the presence of EGFR mutations. We found that the EGFR mutation frequency in these samples was 52.1% (49/94), significantly higher than that in the negative samples (9.1%, 3/33) (p=0.000). We then selected the samples that coexpressed both P-gp and LRP and analyzed the correlation between the coexpression of these proteins and EGFR mutations. We found that the EGFR mutation frequency in these samples was 60.9% (28/46), significantly higher than that in the P-gp- and LRP-negative samples (29.6%, 24/81) (p=0.001). Because the samples with positive expression of either P-gp or LRP could be considered to have MDR, we concluded that the NSCLCs with MDR always bear the EGFR mutations (Table 3, Fig. 3).
Correlations between P-gp and LRP expression and KRAS mutations
The KRAS mutation frequency in the P-gp-positive samples was 5.4% (3/56), lower than that in the negative samples (5.6%, 4/71), although this difference was not significant (p=1.000). The KRAS mutation frequency in the LRP-positive samples was 6.0% (5/84), higher than that in the LRP-negative samples(4.7%, 2/43), although this difference was also not significant (p=1.000). Moreover, we selected the samples that were positive for P-gp or LRP and analyzed the correlation between the expression of these proteins and KRAS mutations. We found that the KRAS mutation frequency in these samples was 5.3% (5/94), lower than that in the negative samples (6.1%, 2/33), although this difference was not significant (p=1.000). We then selected the samples that coexpressed both P-gp and LRP and analyzed the correlation between the coexpression of these proteins and the presence of KRAS mutations. We found that the KRAS mutation frequency in these samples was 6.5% (3/46), higher than that in the P-gp- and LRP-negative samples (4.9%, 4/81), although this difference was not significant (p=1.000). Thus, we concluded that no significant relationship exists between MDR and the presence of KRAS mutations in NSCLC (Table 4).
DISCUSSION
NSCLC accounts for approximately 85% of lung cancers.19 Traditional chemotherapy has played an important role in the treatment of NSCLC, although its curative effect has been greatly limited by MDR. It is well known that the occurrence of MDR is closely related to the expression of P-gp/LRP in NSCLCs. P-gp is a 170-kDa transmembrane protein that was first discovered in 1976. P-gp can decrease the concentration of various drugs in the cytoplasm by extruding them out of cells and promoting the development of MDR.20212223 LRP, which was initially identified in a non-P-gp MDR lung cancer cell line, is a major component of the human major vault protein.2425262728 LRP can decrease the concentration of chemical drugs in the nucleus by regulating nucleocytoplasmic transport and the drugs that are transported to the cytoplasm can then be extruded from the cancer cell by exocytosis.16293031 Previous studies have reported that P-gp is expressed in 35-52% of NSCLCs and LRP is expressed in 65-88% of NSCLCs.293233 The expression of P-gp/LRP could be regarded as a biomarker of primary MDR in NSCLCs. In this study, we found that the frequencies of positive expression of P-gp and LRP detected by immunohistochemistry were 44.1% and 66.1% respectively, which was consistent with the frequencies reported previously, thus the expressions of them were reliable for used as biomarkers to indicate primary MDR of the patients in this study.
In this research, clinicopathological characteristics of the patients with NSCLCs expressing P-gp/LRP positively were similar to those bearing EGFR mutation in exon 19 or 21. Generally, patients with NSCLCs bearing these mutations could benefit from EGFR-TKI. Therefore, one could speculate that patients with NSCLCs expressing P-gp/LRP would also benefit from EGFR-TKIs. Recently, mutation in EGFR exon 19 or 21 has been used as a biomarker for sensitivity of NSCLCs to EGFR-TKIs.34353637 Thus, we analyzed correlations of P-gp/LRP expression with EGFR mutation status to investigate whether patients with NSCLCs expressing P-gp/LRP would bear the EGFR mutation in exon 19 or 21. We found that the EGFR mutation frequency in cancers expressing P-gp/LRP was significantly higher than in those without. These results suggest that NSCLCs expressing P-gp/LRP bear the EGFR mutation in exon 19 or 21. As P-gp/LRP expression was found to be a biomarker for MDR, we discerned that NSCLC patients who are not fit for traditional chemotherapy due to cancers with MDR may benefit from EGFR-TKIs.





 XML Download
XML Download