

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Benign prostatic hyperplasia (BPH) with lower urinary tract symptoms (LUTS) is common in older men. Medical treatment with alpha blocker is the first recommended option for patients with BPH/LUTS.1 Alpha blockers could improve BPH/LUTS by relaxing the prostatic urethra and bladder neck through alpha-receptor block.2 As a result of its prostate selectivity, tamsulosin may improve LUTS with fewer side effects. Many studies have shown that tamsulosin is effective and tolerable at doses of 0.2–0.8 mg once daily in patients with symptomatic BPH.34567 In Asian countries, tamsulosin 0.2 mg has been widely used because of their relative low body mass index (BMI).357
Although tamsulosin is one of worldwide favored alpha blockers due to good efficacy and relatively fewer adverse events, tamsulosin has some adverse events including retrograde ejaculation and anejaculation. Considering that most of the adverse events are tolerable, abnormal ejaculation is significant because it increases the drug withdrawal rate. Abnormal ejaculation is a dose-related phenomenon.8 It is due to anemission, which is attributed to the alpha 1A receptor selectivity of seminal vesicle and vas deferens.9
Several studies reported the efficacy and safety of tamsulosin 0.2 mg,5101112 but the results were varied, thus hampering any decision of whether to apply tamsulosin 0.2 mg as an initial treatment in real practice. Several studies reviewed the efficacy and safety of tamsulosin with or without meta-analysis,1314 however, there have been no comparative studies on the tamsulosin 0.2 mg with other alpha blockers, especially including outcome measurement such as International Prostate Symptom Score (IPSS). Our previous study has focused on the improvement of LUTS by treatment with low-dose tamsulosin, however, it did not show the differences from other alpha blockers; 15 the study merely described the overall improvement by tamsulosin 0.2 mg, and there were no controls for comparison.15
The present study attempted to overcome the limitation of previous study15 and demonstrate the treatment efficacy and safety of tamsulsin 0.2 mg compared with other alpha-blockers. In addition, this is the first meta-analysis of tamsulosin 0.2 mg to evaluate the moderat or effects comparing with other alpha blockers.
MATERIALS AND METHODS
This systematic review and meta-analysis were guided by the standard Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol and also guided by the Cochrane Collaboration.1617
Searching strategy
A MEDLINE and Cochrane Collaboration search for studies from 1980 to 2013 were selected using electronic database search formula: Search ((((((("Lower Urinary Tract Symptoms" [Mesh]) OR "lower urinary tract symptom" [tiabkw]) OR "LUTS" [tiabkw]) OR "Prostatic hyperplasia" [Mesh]) OR "benign prostatic hyperplasia" [tiabkw]) OR "BPH" [tiabkw])) AND ((("tamsulosin" [Supplementary Concept]) OR "tamsulosin" [tiabkw]) OR "YM178" [all]). Same electronic database search formula using Emtree was adopted for EMBASE search. Screening criteria were comparison (adrenergic alpha-1 receptor antagonists), outcome (IPSS), and article type (randomized controlled trial) without language restrictions.
Study selection
The studies were included if they met the following criteria: 1) reported outcome measurements included IPSS, 2) interventions included administration of tamsulosin and other alpha-blockers, 3) participants included BPH, and 4) reasonable intention-to-treat (ITT) analysis was performed in randomized controlled trials (RCTs). Two authors (SR Shim and JH Kim) reviewed all filtered articles with title and abstract using predefined inclusion and exclusion criteria. Final inclusion was determined by the GRADE Working Group. References and data for each included study were carefully cross checked to ensure no over lapping data was presented and to maintain the meta-analysis integrity.
Types of interventions and outcomes
The experimental group received tamsulosin 0.2 mg and the control group orally received other standard dose of alpha-blockers (terazosin, doxazosin, naftopidil, silodosin). Outcomes measured mean changes of IPSS, quality of life (QoL), maximal urinary flow rate (Qmax), and post-voided residual volume (PVR) from baseline in patients receiving tamsulosin versus patients receiving other alpha-blockers. Adverse events measured the proportional differences between the tamsulosin group and the other alpha-blockers group.
Types of moderators
Earlier studies have differed in a number of parameters such as countries, control agents, the number of patients, and study duration. We now elaborated on how differences in some of these moderators affect outcomes.
Quality assessment
The risk of bias and methodological quality were assessed in duplicate using the Cochrane Collaboration tool.16 We evaluated the following six parameters: 1) random sequence generation, 2) allocation concealment, 3) blinding of caregivers, personnel, and outcome assessors, 4) incomplete outcome data, 5) selective outcome reporting, and 6) other bias. We graded each parameter of trial quality as low risk of bias, unclear risk of bias, and high risk of bias, and conducted an overall assessment for each controlled trial using the same three criteria. The quality of the evidence related to the estimation of benefits and disadvantages in the population followed the suggestions of the GRADE Working Group by adopting the use of Grade Pro software 3.6.
Meta-analysis assessment of outcome findings and statistical analysis
All variables used the same measurement units and outcomes were recorded as continuous data. The primary outcome was change in LUTS measured by IPSS. Secondary measures included QoL, Qmax, PVR, and adverse events. In the study without standard deviation, the estimate of the pooled standard deviation of the two groups (before/after) was applied. Standardized mean differences (SMD, Hedges' g, the difference between experimental and control group pooled mean change) along with their 95% confidence intervals (Cls) were calculated for continuous variables. Random-effects model of DerSimonian and Laird18 were conducted to obtain pooled overall SMD and 95% CIs for outcomes.
Meta-ANOVA or meta-regression analysis was conducted for each moderator. To examine potential moderators, we used the meta-analytic mixed effects model (MEM).19 We analyzed the variability in the effect sizes due to differences between the categorical moderators (e.g., countries and control agents) with a weighted meta-analytic an alogue to the analysis of variance. For continuous moderators (e.g., number of patients and study duration), we used a restricted maximum likelihood (REML) estimator of the variance of the true effects. However, we didn't analyze moderator effects of post-voided residual urine due to insufficient observations and also we excluded the moderator if there was one observation in each category. The above mentioned analyses were conducted with Comprehensive Meta-Analysis version 2.2 software (Biostat, Englewood, NJ, USA) and STATA version 11.2 software (Stata Corp LP, College Station, TX, USA). SPSS version 21.0 software (IBM, New York, NY, USA) was used to perform the chi-squared-test.
Assessment of heterogeneity
Statistical heterogeneity was assessed by the Cochran's Q test and the I2 statistic. For Cochran's Q, a value of p<0.1 was considered to indicate statistically significant heterogeneity. If either the Cochran's Q statistics (p<0.1) or I2 statistic (>50%) indicated the existence of significant heterogeneity between studies, a random-effects model of analysis (DerSimonian and Laird method) was used.
Assessment of potential publication bias
Publication bias was explained by Funnel plot of this metaanalysis using standard error as the measure of study size and ratio measures of treatment effect. Asymmetry findings in funnel plots indicate publication bias, but the shape of the plot in the absence of bias depends on the choice of axes.
RESULTS
Inclusion of studies
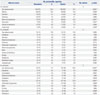
The initial search identified a total of 2862 articles from the electronic database (PubMed: n=722, Cochrane: n=129, Embase: n=2011). After exclusion of 690 studies containing overlapping data or appearing in more than one database and after screening the titles and abstracts, 2026 studies that did not meet the inclusion criteria were further excluded. After intensive screening by detailed evaluation of 146 studies, a total of 21 studies were found to be eligible. Of these, 11 were excluded due to not using low-dose (0.2 mg) tamsulosin in the experimental group (n=5), not using alpha blocker in control group (n=4), and outcome value discordance (n=4). Finally, 10 studies that met all inclusion criteria were included.461220212223242526 The 10 studies consisted of 1418 subjects (722 experimental group and 696 control group). A detailed flow chart showing the selection process is shown in Fig. 1. A systematic review of 10 studies was conducted on the detailed experimental differences and subject descriptions (doxazosin 4 mg, one study; terazosin 5 mg, one study; terazosin 2 mg, two studies; silodosin 8 mg, two studies; naftopidil 25 mg, one study; naftopidil 50 mg, three studies) (Table 1). The duration of treatment ranged from 4–12 weeks. The language of included studies were English, 46122023242526 Chinese,22 and Japanese.21
Quality assessment
Two authors (SR Shim and JH Kim) critically appraised the selected studies using critical criteria of Cochrane Collaboration. Table 2 shows the quality assessment and characteristics of the included studies. All of the studies described randomized methods and reasonable ITT analysis. One study20 included allocation concealment. Blinding methods were conducted as single-blind in three studies4625 and double-blind in three studies.222326 After rating of each item of the critical appraisal, allocation concealment, blinding method, and detection bias resulted in a moderate grade.
Outcome findings
IPSS
Ten studies (n=1418; 722 experimental group and 696 control group)461220252626 reported detailed data on IPSS. The pooled overall SMD in the mean change of IPSS from baseline for the tamsulosin group versus the control group was 0.02 (95% CI; -0.20, 0.25). There was no statistical difference between groups. Heterogeneity test produced p<0.01 and the Higgins' I2 was 75.9%. For evaluation of control agents that have an impact on the improvement of BPH, we also conducted subgroup analysis. The SMD changes of IPSS for the tamsulosin group versus the control group were -0.15 (95% CI; -0.43, 0.13) in terazosin 2 mg, 0.21 (95% CI; 0.04, 0.38) in silodosin 8 mg, and -0.30 (95% CI; -0.68, 0.09) in naftopidil 50 mg (Fig. 2).
QoL
Seven studies (n=1068; 541 experimental group and 527 control group)12202123242526 reported detailed data on QoL. The pooled overall SMD in the mean change of QoL from baseline for the tamsulosin group versus the control group was 0.16 (95% CI; -0.16, 0.48). There was no statistical difference between groups. Heterogeneity test produced p<0.01 and the Higgins' I2 was 83.8%. For evaluation of control agents that have an impact on the improvement of BPH, we also conducted subgroup analysis. The SMD changes of QoL for the tamsulosin group versus the control group were 0.21 (95% CI; 0.04, 0.38) in silodosin 8 mg, and -0.11 (95% CI; -0.57, 0.35) in naftopidil 50 mg (Fig. 3).
Qmax
Ten studies (n=1418; 722 experimental group and 696 control group)461220212223242526 reported detailed data on Qmax. The pooled overall SMD in the mean change of Qmax from baseline for the tamsulosin group versus the control group was 0.00 (95% CI; -0.16, 0.16). There was no statistical difference between groups. Heterogeneity test produced p=0.03 and the Higgins' I2 was 51.2%. For evaluation of control agents that have an impact on the improvement of BPH, we also conducted subgroup analysis. The SMD changes of Qmax for the tamsulosin group versus the control group were 0.02 (95% CI; -0.28, 0.32) in terazosin 2 mg, 0.22 (95% CI; 0.05, 0.39) in silodosin 8 mg, and 0.02 (95% CI; -0.21, 0.26) in naftopidil 50 mg (Fig. 4).
PVR
Four studies (n=474; 237 experimental group and 237 control group)12202124 reported detailed data on PVR. The pooled overall SMD in the mean change of PVR from baseline for the tamsulosin group versus the control group was 0.15 (95% CI; -0.03, 0.33). There was no statistical difference between groups (Fig. 5).
Moderator analyses
Table 3 provides an overview of the moderator analyses. The regression analysis with the continuous variables (number of patients, study duration) revealed no significance in all outcomes as IPSS, QoL, and Qmax. With respect to study duration, there were slightly higher effect sizes in tamsulosin with IPSS and Qmax than control groups (Fig. 6). However, the differences were not significant in IPSS and Qmax (p=0.832 and 0.265, respectively). Subgroup analysis for the pooled IPSS, QoL, and Qmax was performed according to country and control agent. In particular, it was performed for the control group which included more than two studies in each category. The results of meta-ANOVA were not statistically significant in all outcomes. With respect to country, the SMD in China of QoL was 0.559 (95% CI; 0.040, 1.077) and it was in favor of control than tamsulosin. However, it didn't show the difference in the category (p=0.074). With respect to control agent, the SMD in silodosin of Qmax was 0.219 (95% CI; 0.050, 0.389) and it was in favor of tamsulosin than control. However, it didn't show the difference in the category (p=0.127).
Safety
Three of the 10 studies did not describe adverse events.122122 The remaining seven studies462023242526 described the adverse events including urogenital system, circulatory system, digestive system, nervous system, respiratory system, dermatic system, and others. Although not all studies mentioned specific adverse events, tamsulosin was generally well tolerated and had a lower rate of adverse events, especially compared with terazosin (Table 4). Tamsulosin versus silodosin was described in two studies.2326 Adverse events were reported in 52.4% (144/275) of the tamsulosin group and 70.2% (184/262) of the silodosin group. The differences were statistically significant (p<0.001). In more detailed analysis, the tamsulosin group showed high rhinitis value and the silodosin group showed high values of abnormal ejaculation, dry mouth, and loose stool. All were statistically significant. Tamsulosin versus naftopidil was described in two studies.2024 The incidence of adverse events was not significantly different (p=0.935). Tamsulosin versus terazosin was described in three studies.4625 Adverse events were reported in 8.7% (15/172) of the tamsulosin group and 50.0% (79/158) of the terazosin group. The differences were statistically significant (p<0.001). In more detailed analysis, the terazosin group showed higher values of orthostatic hypotension, headache, dizziness, dyspepsia, and dry mouth than the tamsulosin group. All were statistically significant.
Publication bias
The Funnel plot to detect the publication bias or small-study effect in the included studies is summarized in Fig. 7. In the IPSS analysis, three studies lay to the left and one study lay to the right of the funnel. Individual studies are distributed symmetrically about the combined effect size and toward the top of the graph. Thus, there was no evidence of publication bias in this meta-analysis.
DISCUSSION
Transurethral prostatectomy has traditionally been regarded as the most effective method, but most patients prefer medical treatment.27 Currently, the efficacy and tolerability of alpha-1-adrenergic blocker are of great interest and regarded as the first-line treatment for treating BPH/LUTS.28 Among the currently available alpha 1 adrenergic blockers (terazosin, doxazosin, alfuzosin, and tamsulosin), tamsulosin is one of the most commonly used alpha blocker due to its well-known efficacy and safety.29 Tamsulosin is known to have less descending effect of blood pressure compared with other non-selective alpha blockers.3031
An initial study by Abrams, et al.32 showed the efficacy and safety of tamsulosin and suggested the optimum dosage of tamsulosin as 0.4 mg. The standard treatment dosage of tamsulosin in clinical practice in Western countries starts from 0.4 mg/day. However, tamsulosin 0.2 mg as an initial treatment has also been found to be effective in several studies in Asian countries.357 The main reason is the relatively lower BMI of Asian men than Western men. East Asian males, especially Korean, Japanese, and Chinese, have smaller BMIs than Western men, and initial tamsulosin 0.2 mg was set because of expected adverse effects if the same dose used in Western men was adopted. Previous studies with standard dose of tamsulosin showed that the total IPSS score was improved by 36.2% and the Qmax by 13.7% compared with baseline.3233343536 Longterm safety and efficacy of tamsulosin 0.4 mg/day were also demonstrated.36
In our meta-analysis, the improvements of IPSS, QoL, Qmax, and PVR were similar to other alpha-blockers; thus, tamsulosin 0.4 mg and also tamsulosin 0.2 mg are suitable for initial treatment strategy, especially in Asians.
Another merit of tamsulosin 0.2 mg is the lower rate of adverse events. Although most adverse events associated with alpha 1 blockers, especially compared with terazosin, are generally mild and well-tolerated, retrograde ejaculation is an important reason for patient withdrawal. The prevalence of retrograde ejaculation by tamsulosin is known to be about 7%.37 Several reports showed favorable outcome of retrograde ejaculation during intermittent tamsulosin treatment.3839 Giuliano8 reported that tamsulosin 0.8 mg decreased mean ejaculatory volume in almost 90% of men while no ejaculation was noted in 35% of men. This ejaculatory side effect is related with the dose of tamsulosin. This is also a reasonable ground for recommending tamsulosin 0.2 mg as a first-line treatment unless the efficacy of tamsulosin 0.2 mg is not inferior to other standard dose of alpha blockers.
Although retrograde ejaculation is a weak point of tamsulosin, a recent large retrospective study described the benefit of taking tamulosin to improve sexual function in which erectile function was best preserved in men treated with tamsulosin, compared with not taking tamsulosin.40 This abnormal ejaculation is related with the dose of tamsulosin. This is also a reasonable ground for recommending tamsulosin 0.2 mg as a first-line treatment.
To the best of our knowledge, this study is the first scientific reviews about tamsulosin 0.2 mg for BPH/LUTS as an initial treatment strategy to investigate, comparing the efficacy and safety with other alpha blockers. Our prior study has investigated the general effect of tamsulosin 0.2 mg using single arm analysis.15 Using analysis with moderation including meta-regression and meta-ANOVA, we could overcome the heterogeneity of control including different types of alpha blockers. Moreover, the objective analysis of IPSS is the most prominent feature of our study.
Limitations of this meta-analysis reflect common limitationsof other systematic reviews and meta-analyses. Indirect evidence should be cautiously applied in practice as it is usually considered less reliable than direct evidence.4142 In the present study, however, two sets of controlled trials were sufficiently similar in terms of moderators of relative treatment effect, which enabled scientific indirect analysis with moderation. These systematic reviews and meta-analyses could not overcome the bias of the original studies. Moreover, they were themselves influenced by selection bias and publication bias. For instance, four trials in the present study were laid out of the funnel plot, indicating publication bias. However, Sutton, et al.43 reviewed 48 articles from Cochrane Database of Systematic Reviews and showed publication or related biases were commonin the investigation of meta-analyses. Moreover, they found that these biases did not affect the conclusions in most cases.
Our meta-analysis focused on the comparison between tamsulosin 0.2 mg and other alpha blockers as an initial treatment option. Although we performed a subgroup analysis with limited circumstance due to small number of studies for each subgroup, all other alpha-blockers were compared as controls. This was reasonable for the initial hypothesis of our study. To control the heterogeneity of control groups, we implemented the meta-regression method to identify the moderator's effect. By this meta-analysis and meta-regressions, we could clarify the efficacy of tamsulosin 0.2 mg compared with other alpha blockers with standard doses.
Although social-demographic factors such as income and extent of education could affect the treatment pattern and outcome in BPH,44 we did not include those factors because of the widened heterogeneity and missing data. However, this overview of tamulosin 0.2 mg provides more scientific evidence of efficacy and safety of tamsulosin 0.2 mg, and also advocates the use of tamsulosin 0.2 mg for first-line treatment.
In conclusion, tamsulosin 0.2 mg is efficacious, with improvements of IPSS, QoL, Qmax, and PVR. Tamsulosin 0.2 mg is suitable as an initial treatment for symptomatic BPH. Considering dose-related adverse events, the indication for tamsulosin 0.2 mg could be widened.










 XML Download
XML Download