

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) is a chronic, relapsing, inflammatory skin disease characterized by severe pruritus and eczematous skin lesions.1 Lichenified plaques and itching all day long and even worse at night, causing loss of sleep (LOS), are debilitating. Various treatment methods have been introduced, including emollients, topical steroids, topical calcineurin inhibitors, systemic immunosuppressants and/or phototherapy,2 but none of these are curative. In some AD patients, there is convincing evidence that allergens, especially the house dust mite (HDM), play a relevant role in eliciting or aggravating the eczematous skin lesions and may contribute to eczema flare-ups.34 The nature of the skin inflammation in AD has raised a growing interest in treatment with allergen-specific immunotherapy (SIT).3 Besides, SIT has been used as the only specific therapy in allergic disease, such as allergic rhinitis, mild allergic asthma and bee venom anaphylaxis.456 Several studies with AD patients have been reported, but most include small sample sizes and usually a maximum of one year of follow-up.78910 Our clinic has designed a protocol to maintain SIT for at least 3 years or more, as patients tend to keep improving even after one year of treatment. To evaluate the efficacy of long-term treatment with HDM-SIT, we performed a retrospective analysis of over 200 AD patients.
MATERIALS AND METHODS
Subjects and treatment
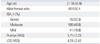
Study subjects were selected by retrospective review of medical records at the Yonsei University Severance Hospital outpatient clinic in the Department of Dermatology. Medical records between 1995 and 2012 were reviewed as approved by the Institutional Review Board. A total of 217 extrinsic AD patients treated with SIT for at least 3 years were selected. Among them, 70 (32.3%) patients were characterized as having severe AD with an investigator global assessment (IGA) above 4 at baseline evaluation, 106 (48.8%) as moderate AD with an IGA of 3, and 41 (18.9%) as mild AD with an IGA of 2. There were no patients with an IGA of 1. The male to female ratio was 49.6:50.4. The mean patient age was 21.16±8.46 (mean±standard deviation) years (Table 1). Subjective symptoms of pruritus and LOS were scored using the visual analogue scale (VAS). Skin prick test (SPT) was performed with 55 allergens (30 inhalants and 25 food allergens) and ImmunoCAP-test was done with 6 commonly offending allergens including egg white, milk, soybean, wheat, Dermatophagoides pteronyssinus (D. pteronyssinus) and Dermatophagoides farinae (D. farinae). Wheal diameters ≥3 mm in about 15 minutes after the test a were considered positive in SPT and ≥3.5 kU/L in CAP-test were regarded as positive. Initially, candidates for SIT were selected through total IgE and CAP-test or SPT results showing hypersensitivity to HDM. A HDM allergen extract containing a mixture of D. pteronyssinus and D. farinae extracts (50:50%) adsorbed to tyrosine (Tyrosine-s®; Allergy Therapeutics Inc., West Sussex, United Kingdom) was used according to the manufacturer's instructions. Treatment schedules included two stages: an induction phase and a maintenance phase. During the induction phase, both vial #1 (5 mL, green, 1/8 dilution of vial #2) and vial #2 (5 mL, red, with maximum allergen extract) were used. We slowly escalated the HDM extract dosage to safely induce desensitization every week for 16 to 18 weeks following the manufacturer's instructions. When the maintenance dosage was reached (1 mL of red vial), the patient visited the clinic a total of four times bi-weekly with following visits occurring monthly, and the treatment continued for 3 to 6 years depending on the patients' response. Post-treatment clinical outcome was measured at the end of treatment session.
Data analysis
Patient IGA, pruritus scores, LOS using VAS, total serum IgE, and eosinophil counts were collected. We established our own scoring system reflecting IGA and subjective symptoms including pruritus and LOS to combine both physician and patient evaluations. We scored from 0 to 5 to estimate the overall clinical response: 0, aggravation of clinical symptom; 1, no improvement; 2, mild improvement with no change in IGA but reduction of pruritus; 3, good response with less than 2 points of improvement of IGA and subjective symptom improvement; 4, excellent response with more than 2 points of improvement of IGA to near-complete remission with symptom improvement; and 5, complete remission with an IGA of 0 with very mild or no symptoms. Patients were additionally classified into four groups according to age, initial disease severity, duration of treatment, and the number of allergen sensitizations. We used IBM SPSS statistics software, version 19.0 (SPSS Inc., Chicago, IL, USA) to analyze data with significance thresholds of p<0.05 and p<0.01. As a further evaluation, we compared baseline laboratory factors including total IgE and eosinophil counts from two groups: good SIT responders and poor SIT responders. We defined those with clinical response scores between 3 and 5 as good responders and those with clinical response scores between 0 and 2 as poor responders.
RESULTS
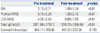
Clinical improvement of 217 patients was judged by using the IGA together with patients' subjective assessment of symptoms using VAS score. The mean IGA was significantly reduced from 3.12±0.71 to 1.08±1.24 (p=0.001) after SIT. Also, according to the eczema area and severity index (EASI) score data of 124 patients, significant improvement was still observed after SIT (from 17.47±13.19 to 2.86±4.74, p<0.001). Pruritus and LOS were also significantly reduced (Table 2). We defined VAS 1–3 as mild symptom, 4–6 as moderate symptom, and 7–10 as severe symptom. Before the treatment, 175 (80.6%) patients had suffered from moderate to severe pruritus and 120 (55.3%) patients suffered severe to moderate LOS. In a post-treatment evaluation, only seven (3.2%) patients exhibited severe pruritus and 23 (10.6%) exhibited moderate pruritus. Other patients had mild to no itching sensation. Additionally, only 14 (6.5%) patients suffered from severe to moderate sleep disturbance while 203 (93.5%) patients experienced mild to no LOS (p<0.001). Clinically, 192 patients (88.4%) improved, with 138 patients (63.6%) achieving complete or near-complete remission with mild itch only and no significant skin lesions (Fig. 1). The mean value of total serum IgE significantly decreased from 2071.88±1757.3 kU/L to 1319.23±1384.68 kU/L (p=0.012); however, eosinophil counts insignificantly decreased (p=0.103). Side effects were reported in 2 patients (less than 1%) including urticaria, localized eruption, pruritus, transient exacerbation of previous atopic lesions, and relapse of previously diagnosed asthma. All side effects were very mild and controlled well with antihistamines or resolved spontaneously.
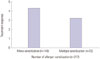
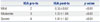
We additionally performed three different subgroup analyses according to patient's age, AD severity and the number of allergens that patients were sensitized. When patients were grouped according to age, better SIT outcomes were observed in those patients under 12 years of age (p=0.024), while patients over 18 years of age experienced the least improvement (Fig. 2). When patients were grouped by AD severity, the mild (IGA 0–2), moderate (IGA 3), and severe (IGA 4–5) groups all showed significant clinical improvement (Table 3); however, AD severity was not significantly correlated with the degree of treatment response (p=0.147). Nevertheless, patients with moderate to severe AD presenting an initial IGA over 3 responded better to SIT treatment than patients with mild AD (p=0.036). When patients were grouped by the number of allergens to which they were sensitized, patients who were sensitized only to HDM had a tendency to respond better than those who also showed positive SPT results to other food or inhalant allergens and/or who are sensitized to other allergens mainly including egg white, milk, soybean, wheat according to CAP-test results, but results between two groups were not significant (p=1.051) (Fig. 3).
To evaluate parameters for predicting treatment outcome, we compared the initial total serum IgE levels and eosinophil counts of good responders to those of poor responders. The mean total IgE level and eosinophil counts were 2098.03±1756.72 kU/L and 618.35±324.58 count/µL, respectively, in good responders and 1944.06±1805.40 kU/L and 544.29±178.57 count/µL, respectively, in poor responders. No significant differences were observed between two groups at baseline (p=0.248 and 0.736). However, both were significantly reduced only in good responders (Table 4). We additionally analyzed the duration of treatment in both groups, since the duration of treatment might have affected the treatment outcome. However, both good and poor responders groups showed same mean treatment duration (3.3 years).
Upon additional review of medical records, we identified 15 patients who reached complete remission within three years. The mean age of these 15 patients was 13.33±6.58 years, and male to female ratio was 46.7:53.3. Mean treatment duration was 2.13±0.61 (Table 5). Total serum IgE was significantly reduced (p<0.027) in these patients; however, we could not assess eosinophil counts due to inadequate information (Table 6).
DISCUSSION
The goal of SIT is to induce allergen-specific tolerance therefore, it is also known as allergen vaccination.11 By inducing allergen-specific regulatory T cells (Tregs), the patient can acquire immune tolerance against the antigen of interest.1213 SIT-mediated induction of Tregs expressing interleukin (IL)-10 and transforming growth factor β elicits the early desensitization phase of mast cells, basophils, and eosinophils. These Tregs also inhibit IgE production by suppressing Th2 cells.14 In addition, they also stimulate the expression of IgG4, a non-inflammatory immunoglobulin isotype.11516 SIT treatment also suppresses IL-3, IL-4, IL-5, IL-9, and IL-13, cytokines which are expressed by Th2 cells and play an important role in the activation, differentiation, and survival of mast cells, eosinophils, and basophils.1
Despite the reported controversial effects associated with SIT, several randomized controlled trials revealed significant improvement of clinical symptoms after SIT, and, follow-up meta-analyses have confirmed SIT-associated improvements.17 We recently analyzed 8 RCTs, which comprised 385 patients, and observed that SIT significantly improved AD symptoms [odds ratio (OR), 5.35; 95% confidence interval (CI), 1.61–17.77; number needed to treat, 3; 95% CI, 2–9]. SIT also exhibited significant efficacy in long-term treatment (OR, 6.42; 95% CI, 1.50–27.52), for patients with severe AD (OR, 3.13; 95% CI, 1.31–7.48), and also when administered subcutaneously (OR, 4.27; 95% CI, 1.36–13.39).
In the present study, we performed additional four different subgroup analyses according to patients' age, initial AD severity, duration of treatment, and the number of sensitized allergens. First, the subgroup with patients under 12 years of age exhibited better treatment outcome when compared with older patient groups. In our meta-analysis, a subgroup analysis of children who underwent SIT did not reveal significant associations between age and treatment outcome.17 However, the analysis had a limitation of including a small number of studies and patients, thus being a preliminary result. AD usually starts during childhood, with a high proportion of patients undergoing spontaneous remission. In severe cases, however, AD persists until adulthood or starts, relapses, or aggravates later in life.1819 Severe disease course in adult AD can be one explanation for relatively unsuccessful treatment response observed in older patients in our current study. Moreover, chronic disease associated with defined, large areas of lichenificationthick, leathery skin due to a chronic inflammation is harder to treat. Additionally, genetic predisposition (for example, a mutation in the filaggrin gene) resulting in an impaired skin barrier, has recently been identified as an another risk factor for severe, persistent AD.2021222324 Prolonged immune system dysregulation may also affect SIT response differentially with patient age, but additional studies are needed to identify precise mechanism in this interaction.
A randomized, double-blinded, placebo controlled study done by Novak, et al.25 demonstrated that only patients with a total Severity Scoring of Atopic Dermatitis (SCORAD) >50 significantly responded to SIT. In our current study, AD severity did not significantly correlate with treatment efficacy, but patients with moderate to severe AD IGA responded significantly better to SIT, and they were more likely to reach near-complete to complete remission. Patients with mild AD also responded well to the therapy. In brief, all AD patients in our study benefitted from SIT regardless of disease severity. Further controlled studies are needed to confirm the efficacy of SIT in mild AD patients.
Our data did not indicate that the effect of SIT was directly associated with treatment duration when the treatment was given for more than three years. Meta-analyses revealed success with long-term treatment (over one year); however, most patients did not reach near complete to complete remission, and there are no specific established guidelines for how long treatment should be maintained. When compared to the previous randomized double blind, placebo controlled studies done after one year of treatment, we found better treatment responses after three years of therapy. Therefore, we propose that therapeutic success can be achieved not only in patients with severe AD but also in other AD patients with long-term SIT treatment (over three years).
Patients mono-sensitized to HDM had a better outcome than multi-sensitized patients; however, this difference in treatment outcome was not significant. Although some patients were multi-sensitized to other allergens, multi-sensitized patients can also benefit from the treatment since HDM is thought to be the most potent exacerbating factor. More effective treatment approaches for multi-sensitized patients should be considered in future studies.
We also analyzed total serum IgE levels and eosinophil counts, both at baseline and after treatment. Both were reduced after treatment, but there was no significant difference between good and poor responders at baseline. Furthermore, although both IgE and eosinophils significantly decreased in good responders, they did not correlate with clinical improvement. Currently, there are no biomarkers for predicting SIT outcome in AD patients. Many clinicians and scientists are working to identify such biomarkers, but this is a very challenging task because AD is multifactorial disease associated with a complex immunologic reaction. Nevertheless, we expect a forthcoming surge in biomarker discovery, which can predict, assess, and standardize treatment responses in the near future.
Considering that this is a retrospective study analyzing the data from AD patients who received SIT for more than three years, several limitations exist. First, since not all the patients had SCORAD or EASI scores, we had to use IGA which is less objective than other methods. However, we used our own scoring system in evaluating final treatment outcome by combining the pruritus and LOS result, which is similar to SCORAD system. Second, there may be a selection bias that could result in more favorable outcome. "Three years of treatment" could mean that patients were tolerating the procedure because it had been effective, while those who did not experience symptomatic improvement may have dropped out. And also, it was difficult to precisely evaluate patients' compliance since it was a retrospective analysis which might have resulted in statistical bias. When we reviewed our records from 1995 to 2012, only about 11.9% of patients had decided to withdraw from the treatment regimen. These patients included those who were unable to maintain SIT or had to postpone the maintenance therapy due to military service, getting a new job, moving to another location, or studying abroad. As we did not have a control group, there is a chance that the observed beneficial effects could be due to other oral or topical medications, especially among those patients with milder AD. However, because SIT is usually given considering not only disease severity but also the long-standing and recurrent history of disease, treatment responses might reflect the effect of SIT. Lastly, we were unable to distinguish remission after SIT from natural remission. Even though persistent AD is increasing and about 60% of patients have AD still in their adulthood,26 it is not possible to differentiate the spontaneous remission from successful treatment result. Further studies with a control group are necessary to confirm the age-related treatment efficacy.
As mentioned above, there have been several studies on the efficacy of one year SIT treatment regimens. Nonetheless, the merit of our current study is a long-term (more than three years) SIT treatment efficacy. Only 15 patients reached complete remission within three years and the number is far less than that of patients reaching complete remission after more than three years of SIT (98 patients). In the future study, we will compare; long-term treatment efficacy more thoroughly the SIT efficacy at one year, two years.
In conclusion, we emphasize the usefulness of HDM SIT as the only curative strategy for AD. Starting therapy at a younger age and maintaining long-term treatment (more than three years) may be necessary to achieve a good outcome. Although patients with more severe AD and mono-sensitized patients were more likely to experience better treatment outcomes, other patients also benefitted from the treatment. Optimizing preparation with more refined specific antigenic peptides from major allergens,27 and the use of potent adjuvants would improve the treatment outcome. Identification of a good biomarker to predict, assess, and standardize treatment efficacy is expected to develop an advanced SIT application in the future.





 XML Download
XML Download