

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radiofrequency catheter ablation (RFCA) has become an important rhythm control therapy in the management of anti-arrhythmic drug-resistant atrial fibrillation (AF).12 However, the risk of procedure-related thromboembolic events exists at the time of catheter ablation, and the embolic risk is reportedly in the range 0.4–2.0%.345 Most strokes occur within 24 hours of the procedure.5 Therefore, an optimal peri-procedural anticoagulation is required, although its specific details have not been determined. Most patients with AF take oral anticoagulants. Anticoagulation guidelines that pertain to cardioversion of AF have been proposed for patients who present for AF ablation at the time of the procedure.6 Therefore, if the patient has been in AF for 48 hours or longer or for an unknown duration, most experts prescribe 3 weeks of effective oral anticoagulation prior to the RFCA. Since there are no studies comparing the use of heparin with no heparin use during RFCA, all patients receive intra-procedural heparin regardless of anticoagulation status or anticoagulant use. After a successful procedure, oral anticoagulants are usually restarted after hemostasis is achieved and then continued for at least 2–3 months, even in patients with a low CHA2DS2-VASc score.7 Several studies have recently examined the peri-procedural management of novel oral anticoagulants (NOACs) for patients who are scheduled to undergo RFCA.89101112 The advantages of NOACs as peri-procedural anticoagulants include a rapid onset of action with shorter time required to achieve therapeutic anticoagulation and no concern for a sub- or supra-therapeutic international normalized ratio (INR) on the day of the procedure. In contrast, although there is a consensus that pre-procedural uninterrupted warfarin is safe and effective for preventing procedure-related thromboembolism,13 termination of NOACs for 24–48 hours before the procedure has been recommended by the European Heart Rhythm Association (EHRA) practical guide.14 Therefore, we hypothesized that NOACs are non-inferior to continuous warfarin in the peri-procedural period of AF catheter ablation, despite the transient blanking period. The purpose of our study was to compare the use of NOACs and uninterrupted warfarin in the peri-procedural period for AF catheter ablation in terms of safety, efficacy, and intra-procedural heparin requirement.
MATERIALS AND METHODS
Study design
The study protocol adhered to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Yonsei University Health System. All patients provided written informed consent. Among 632 consecutive patients in the Yonsei AF ablation cohort between September 2012 and October 2014, 141 patients taking peri-procedural NOACs (72% men; 58±11 years old; 71% with paroxysmal AF) were initially compared to 491 patients taking uninterrupted warfarin before AF ablation. We then conducted propensity score matching between the continuous warfarin group and the NOAC group. A total of 141 patients in the NOAC group and 281 age-, sex-, AF type-, and history of stroke-matched patients in the warfarin group were compared. All patients had anti-arrhythmic drug-refractory AF and underwent RFCA. All patients received warfarin or NOAC as oral anticoagulants prior to the procedure for 3 or more weeks. All patients, including those with effective pre-procedural oral anticoagulation, underwent transesophageal echocardiography (TEE) prior to RFCA. The choice of oral anticoagulant was decided based on the preference of the cardiologists or primary care physicians who treated the patients before the procedure. Among the 141 patients in the NOAC group, 11 were switched from warfarin after the referral because of an unstable INR.
We assessed each patient's heparin requirement and activated clotting time (ACT) during the procedure, and thromboembolic and bleeding complications during 30 days post-AF ablation. Thromboembolic complication was defined as stroke, transient ischemic attack (TIA), or systemic embolism. Bleeding complications were classified as major or minor bleeding. Major bleeding was defined as pericardial tamponade or bleeding including a hematoma requiring a blood transfusion or a decreased level of hemoglobin ≥4.0 g/dL without an overt source.15 Minor bleeding was defined as bleeding with a decreased hemoglobin level at 3.0–4.0 g/dL without an overt source, groin hematoma, or pericardial effusion without tamponade. Hematoma was defined as any significant palpable mass associated with purpura at skin level.16 We also evaluated vascular complications (any identified pseudoaneurysm or arteriovenous fistula) that required re-hospitalization or longer hospitalization. We compared the NOAC and warfarin groups for 1) duration of pre-procedural anticoagulation, 2) intra- procedural heparin requirement, and 3) intra-procedural ACT, and 4) complication of thromboembolism, and 5) bleeding during the 30-day post-RFCA period.
Anticoagulation
We continued anticoagulation therapy for patients presenting for RFCA who were taking warfarin. The target therapeutic INR was 2.0–3.0. The INR was checked on a monthly basis before the procedure and on the same day as the procedure. Warfarin was continued at a maintenance dose (INR 2.0–3.0) after the procedure. For patients taking a NOAC (dabigatran, rivaroxaban, or apixaban) who presented for RFCA, we discontinued two doses of dabigatran and apixaban and single doses of rivaroxaban before procedure, and restarted NOAC on the day of the procedure after confirming hemostasis following sheath removal. All patients received intra-procedural anticoagulation with intravenous heparin. Initial bolus doses of unfractionated heparin (100 IU/kg) were administered before transseptal puncture. The ACT was monitored every 10–30 min throughout the procedures and adjusted as needed with periodic heparin boluses. The intensity of heparinization maintained was at an ACT of 350–400 s during the procedure. Oral anticoagulation was then continued for at least 3 months after the procedure in all patients.
Radiofrequency catheter ablation
Details regarding electrophysiological mapping and RFCA technique and strategy were described in previous studies.1718 In brief, an open irrigation 3.5-mm-tip deflectable catheter (Celsius, Johnson & Johnson Inc.; Diamond Bar, CA, USA; Coolflex, St. Jude Medical Inc., Minnetonka, MN, USA; 30–35 W; 47℃) was used for RFCA (Stockert generator, Biosense Webster Inc., Diamond Bar, CA, USA). Circumferential pulmonary vein isolation and bi-directional block of the cavotricuspid isthmus ablation were performed in all patients. For patients with persistent AF, we added a roof line, posterior inferior line, and anterior line as a standard lesion set. Additional ablation of the superior vena cava or non-pulmonary vein foci or after complex fractionated electrography was determined by the operator.
Follow-up after ablation
All patients were followed up after the procedure with anti-arrhythmic drugs discontinued. All patients were monitored with continuous electrocardiography overnight and discharged the day after the procedure. All patients were scheduled for outpatient clinic follow-ups and rhythm follow-ups according to the 2012 Heart Rhythm Society/EHRA/European Cardiac Arrhythmia Society Expert Consensus Statement guidelines.6 In this study, we compared the efficacy and safety of NOACs and warfarin within 1 month of the AF ablation.
Statistical analysis
The baseline characteristics between the NOAC and warfarin groups were compared. Continuous variables are reported as mean±standard deviation (SD) and analyzed using the Student t-test. Categorical variables were reported as counts and proportions and analyzed using Pearson chi-square test or Fisher exact test as appropriate. Propensity score matching was used to reduce the selection bias associated with the oral anticoagulant treatment and potential confounding bias in an observational study and to adjust for the differences in the patients' characteristics.19 At the initial comparison, AF type and history of stroke/TIA were statistically different between NOAC group and warfarin group. Therefore, we chose those 2 variables, age, and sex as references for propensity score matching. The following variables were considered each time a patient from the NOAC group was matched to a maximum of two patients from the warfarin group. A matching caliper of 0.05 SD of the logit of the estimated propensity score was enforced using R package, including Matchit, RI tools, and CEM.19 The SPSS statistical package version 20.0 (SPSS Inc., Chicago, IL, USA) was used to perform all of the statistical evaluations. p values ≤0.05 were considered statistically significant.
RESULTS
Baseline characteristics
The patient population comprised 141 patients in the NOAC group and 491 patients in the uninterrupted warfarin group. We selected 281 patients in the warfarin group after age-, sex-, AF type-, and history of stroke-matching and compared them with the 141 patients in the NOAC group. Patients in the NOAC group were prescribed dabigatran (n=99; 70.2%), rivaroxaban (n=18; 12.8%), or apixaban (n=24; 17.0%). Table 1 compares the baseline characteristics of the study population according to oral anticoagulant. Before propensity score matching, NOACs were more likely to be prescribed for patients with paroxysmal AF (p=0.004) and those without a history of stroke/TIA (p=0.034). After age-, sex-, AF type-, and history of stroke-matching, the duration of pre-procedural anticoagulation was significantly shorter in the NOAC group than in the warfarin group (76.3±110.7 days vs. 274.7±582.7 days, p<0.001). None of the other variables significantly differed between the two groups.
Intra-procedural characteristics
There was no significant difference in total procedure (181.8±47.9 min vs. 177.2±52.0 min, p=0.387) and total ablation times (4364.5±1560.1 s vs. 4353.4±1563.6 s, p=0.945) between the NOAC and warfarin groups. During the procedure, the mean ACT differed significantly between the NOAC and warfarin groups (350.0±25.0 s vs. 367.4±42.9 s, p<0.001) (Fig. 1A). The total dose of unfractionated heparin to maintain a therapeutic ACT during RFCA was significantly higher in the NOAC group than in the warfarin group (18068.3±6844.4 IU vs. 11890.3±5808.1 IU, p<0.001) (Fig. 1B).
Complications
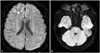
The overall rate of peri-procedural complications, including minor bleeding, was 11.1% (70/632) (Table 2). Two thromboembolic (0.3%), 44 bleeding (7.0%), and 17 vascular complications (2.7%) occurred during the 30-day follow-up period. Although stroke-related events tended to occur more often in the NOAC group (1.4% vs. 0%, p=0.049), bleeding (4.3% vs. 7.7%, p=0.152) and vascular complications (1.4% vs. 3.1%, p=0.386) did not differ between the groups. The overall complication rate was not significantly different after age-, sex-, AF type-, and history of stroke-matching. There were two cases of post-procedural stroke in the NOAC group (Table 3). One patient complained of vomiting and headache immediately after the procedure, while another manifested diplopia 10 hours after RFCA. Both patients showed small acute infarctions documented by brain magnetic resonance imaging (Fig. 2). These patients had a CHA2DS2-VASc score ≤1 and paroxysmal AF. Both patients recovered without neurological sequelae after medical therapy.
DISCUSSION
In the present study, we explored the difference between the use of NOACs and uninterrupted warfarin in the peri-procedural period in patients with AF who underwent catheter ablation. In this retrospective observational study, pre-procedural anticoagulation duration was shorter and intra-procedural heparin requirement was higher with NOAC than with uninterrupted warfarin in AF ablation. Although the incidences of peri-procedural thromboembolism and bleeding did not differ, there were two cases of minor stroke in the NOAC group with pre-procedural blanking of the anticoagulation.
Comparisons of NOAC and warfarin in patients with non-valvular AF
Options for anticoagulation have expanded steadily over the past few decades, providing a greater number of agents for preventing and managing thromboembolic disease. In particular, anticoagulation with NOACs have led to similar or lower rates of both ischemic stroke and major bleeding, compared to warfarin, in patients with non-valvular AF in large randomized trials.20 These results support the broad concept that NOACs are preferable to warfarin in many cases. For example, the use of peri-ablation anticoagulation with NOACs has been rapidly expanding worldwide. The majority of similar studies has reported non-inferiority or even superiority of NOACs in terms of thromboembolism and bleeding complications.2122232425 As with most studies, our study showed no difference in the peri-procedural incidences of thromboembolism and bleeding during AF ablation in the NOAC and warfarin groups.
Advantages and disadvantages in NOAC use in the peri-procedural period
Anticoagulant use must be balanced to minimize thromboembolic and bleeding risks, as well as complications and side effects, in patients undergoing AF catheter ablation.26 Compared to uninterrupted warfarin, NOAC has several advantages for use in the peri-procedural period of RFCA for AF in terms of convenience (no requirement for routine testing of INR, no need for frequent dose adjustment, and rapid onset of action) and less susceptibility to dietary and drug interactions. Since saturation of warfarin and maintaining an optimal INR is difficult, especially in outpatient clinics,2728 the shorter duration of pre-procedural anticoagulation in the NOAC group versus the warfarin group reflects the convenience of NOAC use. In contrast, NOACs have the following disadvantages: 1) lack of an approved antidote/reversing agent; 2) limited data for efficacy and safety (in patients with chronic kidney disease and long-term adverse effects); 3) lack of easily available monitoring of blood levels and compliance; 4) higher cost; and 5) the required pre-procedural blanking period immediate before AF ablation.
The EHRA Practical Guide suggests that discontinuation and restarting of anticoagulation should be individualized to consider both patient characteristics (kidney function, age, history of bleeding complications, concomitant medication) and procedural factors according to the types of NOACs used.6 However, in many studies on the use of NOACs in ablation, the time for stopping anticoagulation has differed. Some studies stopped anticoagulation on the night before the procedure,2129 while others have uninterrupted anticoagulation.111224 Although there was no statistical difference in thromboembolic or hemorrhagic complications between the NOAC and warfarin groups in this study, there were two cases of minor stroke in the NOAC group. In non-valvular AF, high CHA2DS2-VASc scores reportedly reflect a high risk of stroke;30 however, both patients in this study had low CHA2DS2-VASc scores. Also, we previously reported that routine pre-procedural TEE is not mandatory for stroke prevention evaluation in patients with AF on warfarin;31 however, it is not clear whether the same strategy is acceptable for patients who are taking NOACs. Cappato, et al.32 recently reported that uninterrupted oral rivaroxaban is feasible and event rates were similar to those for uninterrupted warfarin. Therefore, further prospective randomized studies are needed to identify for optimal anticoagulation schedules with other NOACs at the periprocedural period, instead of old EHRA practice guidelines14 with limited evidence.
Effects of NOACs on ACT
Heparin plays some role in the intrinsic coagulation pathways and manifests anticoagulation effects. In contrast, warfarin affects not only the intrinsic coagulation pathways, but also coagulation factor IX in the intrinsic pathways and coagulation factors X and II in the common pathways.33 NOACs clearly affect the common pathways, although each drug targets different coagulation factors. The target coagulation factors are factor II for dabigatran and factor Xa for rivaroxaban and apixaban. We previously reported on the reduced intra-procedural heparin requirement with continuous warfarin strategy, compared to switching to heparin group.13 Saturated warfarin or NOACs increased the ACT and reduced the heparin requirement during the procedure, and a significantly higher heparin requirement in the NOAC group than in the uninterrupted warfarin group was related to skipping anticoagulation in both this study and other studies.212224
Limitations
Since this was a single-center cohort study that included a selective group of patients referred for AF catheter ablation, its results cannot be generalized. Given that most of the previous investigations exploring AF were performed in Caucasian populations, the findings from this study in an Asian population are valuable. This study was non-randomized, and the anticoagulant used in each patient was based on the clinician's preference. This selection bias is visible in the patients' baseline characteristics. To minimize the selection bias, we conducted age-, sex-, AF type-, and history of stroke-matching based on propensity score. We did not analyze the results according to the different NOACs. Although we tried to follow EHRA practice guidelines,14 it was not easy to enforce 24 hours of abstinence before the procedure. Therefore, we skipped two doses of dibigatran or apixaban and a single dose of rivaroxaban. Further double-blind studies are needed for in-depth comparisons of NOACs according to each subset of medication, as are studies with a larger number of patients.
Conclusion
The pre-procedural anticoagulation duration was shorter in the NOAC group than in the warfarin group in patients who underwent AF catheter ablation. Although the intra-procedural heparin requirement was higher and ACT was lower in the NOAC group, there were no differences in peri-procedural thromboembolism and bleeding complications. However, we must pay special attention to the anticoagulation blanking period and the potential poor compliance of patients treated with NOACs immediate before AF catheter ablation.




 XML Download
XML Download