

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The treatment options for small to medium sized vestibular schwannomas include observation, radiotherapy, and surgery.1 Recent refinement of surgical techniques has made it possible to prioritize hearing preservation after tumor resection.2 Moreover, hearing after tumor removal can be restored in patients with bilateral vestibular schwannomas or those with a schwannoma in the only-hearing ear.3
The standard treatment for unilateral hearing loss after unilateral vestibular schwannoma resection has been bone conducting or bone anchoring hearing aids (BCHA or BAHA), though cochlear implantation (CI) has emerged as an alternative method of acoustic rehabilitation, provided that the cochlear nerve remains intact.4 Studies of electrical promontory stimulation in patients after vestibular schwannoma resection have demonstrated favorable results.56
Since the indications for CI have recently expanded, CI has been suggested by many as an appropriate adjunctive treatment to vestibular schwannoma resection.789 Patients with bilateral vestibular schwannomas or with a schwannoma in the only-hearing ear are candidates for CI. In addition, patients with good hearing in the contralateral side are also candidates for the quality of life. Early cochlear degeneration can limit hearing rehabilitation via CI, particularly if there is significant delay after schwannoma resection, despite of sparing the cochlear nerve.4
We describe herein two cases of hearing rehabilitation via CI implemented at the time of vestibular schwannoma resection.
CASE REPORT
Case 1
A 72-year-old woman presented with moderate to severe bilateral hearing impairment. She had used conventional hearing aids in the left ear for eight years, but presented for evaluation of deteriorating hearing secondary to worsening otorrhea. Otoscopic examination revealed a small perforation and discharge at the left tympanic membrane. A pure tone audiogram revealed right sensorineural and left mixed hearing loss (Fig. 1A). Speech discrimination scores were 72% in the right ear at the most comfortable listening (MCL) level, and immeasurable in the left ear. Temporal magnetic resonance imaging (MRI) scan was thus obtained, revealing an 8 mm intracanalicular schwannoma on the left (Fig. 1C and D).
Due to the patient's age and small tumor size, our initial management was conservative, consisting of observation and infection control. However, as the patient desired improvement of hearing in her left ear, we opted for tumor resection with simultaneous CI. Six months pre-operatively, we performed a tympanomastoidectomy on the left ear, which resulted in controlled infection and a well-tympanized eardrum. The bone conduction of the left ear was reserved, and the air-bone gap of left ear was reduced. Subsequently, we resected the tumor via a translabyrinthine approach with concurrent CI (SONATATI100, MedEL, Innsbruck, Austria) via facial recess approach (Fig. 1E and F). We were able to preserve the cochlear nerve, as well as achieve total tumor resection.
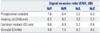
Two years post-operatively, pure tone audiometry demonstrated a threshold of 38.8 dB in the CI augmented left ear and 30.0 dB in the hearing aid augmented right ear (Fig. 1B). The results of the Korean Hearing in Noise test (K-HINT), which measures the binaural hearing performance in a noisy environment, are described in Table 1. A 1 dB decrease in the signal to noise ratio (SNR) corresponds to a 9% improvement in binaural hearing.1011 On average, patients who received CI showed a 19.8% improvement in binaural hearing under front noise; in bimodal mode, a 36% improvement was shown under front noise, and 27% improvement under composite noise.
Case 2
A 58-year-old man who had undergone canal wall down tympanomastoidectomy in his right ear presented with bilateral hearing impairment. He complained of chronic hearing loss in the right ear, as well as abrupt hearing loss in the left. A pure tone audiogram revealed bilateral mixed hearing loss with an average air conduction threshold of 43 dB in the right ear and 72 dB in the left (Fig. 2A). Speech discrimination scores were 92% in the right ear at 86 dB MCL and 88% in the left ear at 102 dB MCL. A year later, a follow-up pure tone audiogram showed complete hearing loss (scale out) in the left ear, along with an unmeasurable speech discrimination score. A left internal auditory canal intracanalicular mass lesion was noted on the preoperative brain MRI scan, with diameter of 6 mm and width of 13 mm (Fig. 2C and D).
We proposed two surgical approaches: mass excision via translabyrinthine approach, followed by either BAHA or CI. This patient and his family opted for the latter option. We conducted canal wall down mastoidectomy, subtotal petrosectomy and EAC closure for infection control, and the tumor was totally resected via translabyrinthine approach, with successful electrode insertion via round window approach (CONCERTO08363, MedEL, Austria) (Fig. 2E-H). At three month follow-up, CI-aided pure tone audiogram revealed an average sound field threshold of 48.8 dB in the left ear (Fig. 2B). Notably, his tinnitus was also markedly reduced.
DISCUSSION
In considering surgical resection of small or medium sized vestibular schwannomas, priority should be given to the preservation or restoration of hearing. BCHA or BAHA have been standard treatments for post-surgical unilateral hearing impairment, but are limited in their capacity to improve hearing in the affected ear. Reports from several centers on CI and labyrinthectomy or vestibular schwannoma resection show a favorable prognosis for concurrent or post-operative CI.79121314 In fact, the prognosis was similar to that of unilaterally deaf patients treated with CI.
Candidacy criteria for CI with tumor resection include total tumor removal, preservation of the cochlear nerve anatomy and function, and surgeon experience. Anatomical preservation of cochlear nerve cannot assure its functional preservation, therefore, intraoperative monitoring can be useful. However, in the present case, we couldn't monitor for several reasons.
MRI can be used post-operatively to evaluate remnant tumor tissue prior to CI implementation, if performed years after resection. In such cases, however, cochlear ossification and cochlear nerve atrophy can present complications. In our cases, complete tumor resection was not necessary for MRI evaluation, therefore, an enhanced CT was used instead for follow-up.
Arriaga and Marks10 were the first to report on concurrent CI and schwannoma resection with favorable outcomes. Successful hearing restoration with CI depends on survival of the spiral ganglion nerve fibers, as well as the patency of the cochlea. The rapid and significant improvement in speech recognition with CI suggests that, despite the presence of tumor in the cochlear nerve and potential intra-operative injuries, the number of surviving spiral ganglion axons is sufficient for CI rehabilitation. There are thus far no reports comparing outcomes between concurrent and staged procedures. Nevertheless, since calcification of inner ear structures can occur as a post-operative complication, earlier implementation of CI operation should be sought for hearing restoration and improvement of quality of life.


 XML Download
XML Download