

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The prognosis of locally advanced hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT) remains dismal. Median survival time without treatment is only 2.7 months.1 Transarterial chemoembolization (TACE) and chemotherapy have been used as palliation,2345 and hepatic resection has been attempted as a curative measure, with less than satisfactory outcomes.5678 Under these circumstances, liver transplantation has been considered a contraindication.91011
Chapman, et al.12 have indicated that prolonged survival is achievable in this context through down-staging of HCC via neoadjuvant TACE and liver transplantation. Furthermore, Han, et al.13 recently reported an objective response rate of 45% using other modes of adjuvant treatment, such as localized concurrent chemoradiotherapy (CCRT), followed by hepatic arterial infusion chemotherapy (HAIC). Moreover, Lee, et al.14 recently reported surgical outcome of liver resection after down-staging of locally advanced HCC localized CCRT with 49.6% of 5-year overall survival rate. Herein, we report our early experience of living donor liver transplantation (LDLT) in eight patients with locally advanced HCC and PVTT after successful down-staging of tumor through CCRT followed by HAIC.
Diagnosis of HCC was based on either pathologic confirmation or radiologic findings. Patients with unresectable HCC and PVTT in the main trunk or first order branch were indicated for CCRT following HAIC. Resectability was decided through regular multidisciplinary approach meeting by hepatobiliary surgeons, transplantation surgeons, hepatologists, radiologists, and radiation oncologists, based on patient's liver function and radiologic image. To assess feasibility of LDLT, heaptobiliary surgeons and transplantation surgeons reviewed the degree and extent of portal vein thrombosis, checking for hepatic arterial stricture or stenosis, as well as viability of extra-hepatic bile duct and the need for vascular or biliary reconstruction. In patients with locally advanced HCC and PVTT, localized CCRT was administered according to the standard protocol established (1998) at Severance Hospital, Yonsei University College of Medicine, Seoul, Korea, followed by HAIC. This protocol has been described previously. Briefly, patients received a total radiation dose of 45 Gy in 25 fractions over a 5-week period, with concurrent HAIC of 5-fluorouracil (5-FU), 500 mg daily delivered via indwelling percutaneous hepatic arterial catheter during weeks 1 and 5 of radiotherapy. One month after localized CCRT, 5-FU (500 mg/m2 over 5 hours on days 1–3) and cisplatin (60 mg/m2 over 2 hours on day 2) were infused every 4 weeks for 3–12 months, adjusting for tumor response.13 LDLTs were performed in eight consecutive patients who achieved successful down-staging of HCC by this means between December, 2011 and September, 2012. Upon approval of our Institutional Review Board, data of all consecutive patients were collected.
Histopathology of explanted liver was evaluated by a single pathologist with appropriate expertise (YNP). Trans-abdominal Doppler ultrasonography was performed on days 1, 2, and 4 post-transplantation to monitor the patency of hepatic and portal vascular anastomoses. Thereafter, dynamic multi-detector computed tomography (MDCT) was done on days 7, 14, and 21 post-transplantation, primarily to confirm patency of hepatic vessels and to monitor patients for potential postoperative complications. As surveillance for tumor recurrence, MDCT was performed every 6 months during the first year post-transplantation, then on a yearly basis. Tumor markers such as alpha-fetoprotein (AFP) and protein induced by vitamin K absence-II (PIVKA-II) were routinely checked each month. Disease-free survival rate was calculated by the Kaplan-Meier method with SPSS 20 for Windows (SPSS Inc., Chicago, IL, USA).
Each patient initially presented with locally advanced HCC and intrahepatic PVTT as well as active hepatitis B viral infection; and each was subjected to a regimen of CCRT, followed by HAIC, for tumor down-staging. All but one were male (median age, 46 years; range, 38–52 years). Three patients first underwent hepatic resections (hemi-hepatectomies: left, 2; right, 1), but intrahepatic recurrences developed in all three. TACE procedures, performed for tumor down-staging, had resulted in peribiliary necrosis (n=2) and liver failure (n=3). Semi-elective LDLTs were performed as life-saving treatment in these five patients, whose hepatic functions were rapidly deteriorating (Fig. 1).
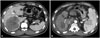
Biologic and morphologic status of HCC improved after CCRT and other treatments. In all patients, serum tumor markers were initially quite high [AFP: median, 4418.07 ng/mL (range, 4.06–69912.95 ng/mL); PIVKA-II: median, 2000 mAU/mL (range, 16–14044 mAU/mL)] but dropped dramatically prior to LDLT [AFP: median, 26.87 ng/mL (range, 1.70–251.34 ng/mL); PIVKA-II: median, 84.5 mAU/mL (range, 18–350 mAU/mL)]. Median tumor diameter (at maximum) was 10.8 cm initially (range, 6.4–15.4 cm) by radiologic assessment, falling to 3.8 cm (range, 1.3–9.0 cm) at post-transplantation pathologic examination (Fig. 2). No viable tumor was evident in the explanted livers of two patients, indicating complete resolution of HCC after CCRT followed by HAIC (Table 1, Fig. 3).
Median post-transplantation follow-up monitoring was 17 months (range, 10–22 months), and median survival time from initial diagnosis was 33 months (range, 22–48 months). No patient deaths occurred during the follow-up period, although three patients developed recurrent HCC at 4, 10, and 13 months post-transplantation as follows: multiple intrahepatic metastases (patient 6, day 119), supraclavicular node metastasis (patient 4, day 294), and solitary lung metastasis (patient 1, day 394) (Table 2). The lung and lymph node metastases were surgically resected with no further progression of disease. The patient with multiple intrahepatic metastases and portocaval lymph node metastasis underwent transcatheter arterial chemoinfusion (TACI), followed by oral sorafenib (Nexavar®; Bayer Pharma AG, Berlin, Germany).
Intraoperative bleeding during LDLT was greater than expected, due to extensive adhesions and deteriorated states of perihepatic anatomy. Median intraoperative blood loss was 7550 cc (range, 2500–12200 cc). Patient 2 had suffered peribiliary necrosis prior to transplantation, resulting in significant hilar restructuring (i.e., portal vein anastomosis, using preserved iliac artery conduit; anastomosis of hepatic artery, with autologous middle colic artery interposition; and Roux-en Y hepaticojejunostomy for anastomosis of bile duct). Five of eight patients required unconventional hepatic artery anastomoses, using autologous arterial interposition or transposition graft. In three patients, Roux-en Y hepaticojejunostomy was done for bile duct reconstruction. Ultimately, four complications related to anastomoses were recorded in three patients (bile duct stricture, 2; portal vein stenosis, 2) (Table 3). All complications were successfully resolved through radiologic interventions.
Liver transplantation is considered one of the best treatment options for patients with early-stage HCC.151617 However, this accounts for only 10–20% of those with HCC overall. The majority of sufferers have more advanced disease.18 Various down-staging procedures, including radiofrequency ablation, TACE, TACI, and transarterial radioembolization with Yttrium-90 microspheres (TARE-Y90), have been devised for advanced HCC.101218192021 However, recent use of liver transplantation after successful down-staging of tumors has yielded acceptable results compared with outcomes of liver transplantation in early-stage HCC and in end-stage liver disease.222324
TACE or TARE-Y90 are viewed as a relative contraindications in patients with advanced HCC and PVTT, because conventional down-staging protocols have had negligible success.25 Using a regimen of localized CCRT followed by HAIC in precisely such patients, who were unresponsive to conventional therapy, Han, et al.13 showed a substantial response rate (45%) and an acceptable median survival time (13.1 months). Localized radiotherapy (RT) of the liver has also emerged as an effective means of controlling the progression of HCC, compared with whole-liver RT.26 Highly selective localized RT enables more intense targeting of masses in liver, with less hepatotoxicity.
Conventional systemic chemotherapy has proven ineffective in HCC, and toxicity is an issue. However, HAIC allows local delivery of chemotherapeutic agents in greater concentrations, alleviating systemic toxicity.2272829 With concurrent use of hepatic RT and HAIC, response rates in patients with locally advanced HCC stand to improve, although roughly a 30% rate of hepatic decompensation has been reported with the use of CCRT followed by HAIC in this setting.13
Generally, patients with locally advanced HCC and PVTT have been ineligible for liver transplantation, even with down-staging, due to high rates of tumor recurrence.91011 Earlier, we performed LDLTs as life-saving interventions in five patients, who suffered from rapid hepatic functional deterioration after CCRT and HAIC. Given satisfactory short-term outcomes in these initial five attempts, we then performed LDLTs in another three patients, who achieved down-staging of HCC. No mortalities occurred during the follow-up periods, and the 1-year disease-free survival rate was 75.0%.
There are two critical factors in this group of patients, in terms of eligibility for LDLT. The first issue is operative feasibility, which is often hampered by significant anatomic deterioration after various down-staging procedures, including RT, HAIC, and other treatments (e.g., TACE or liver resection). Radiation alone is known to damage the microvasculature and induce hepatic fibrosis.30 Moreover, HAIC and TACE create significant hepatic hilar inflammation and intimal arterial injury, and their inflict may result in vascular thrombosis, adding to radiation effect.1831 In this particular group of patients, LDLTs are demanding procedures, subject to elaborate preoperative preparation.
Only three of our eight patients were suited for conventional anastomoses of hilar structures. Modifications were otherwise required for reconstruction of hepatic vessels and biliary drainage. In patient 2, cryopreserved iliac artery was used as a conduit for portal vein anastomosis (due to thrombosis); hepatic artery anastomosis required autologous middle colic artery interposition graft (due to stenosis); and Roux-en-Y hepaticojejunostomy was performed for bile duct reconstruction. These types of complex and technically demanding anastomoses in damaged areas resulted in some postoperative complications: in three patients, a total of two portal vein and two bile duct strictures developed at anastomotic sites, but all complications were resolved through radiologic interventions. Nevertheless, reconstruction of vascular and biliary system was feasible, and all complications were resolved through radiologic interventions. Thus, LDLTs are not off-limits in these patients.
The second critical issue is the achieved degree of tumor down-staging. For survival of both patient and graft, successful down-staging of HCC is a prerequisite, as determined by radiologic and biologic response to treatment. Tumor necrosis and change in tumor size on imaging studies are the indices of radiologic response. Biologic response is evaluated by declining levels of serum tumor factors, such as AFP and PIVKA-II. In most published studies, an acceptable serum AFP level is <400 ng/mL, which all of our patients displayed. Median pre-transplantation serum AFP level was 26.87 ng/mL (range, 1.7–251.34) (Table 1).
There were three instances of tumor recurrence during post-transplantation follow-up periods (Table 2). Two patients (solitary pulmonary nodule and supraclavicular node metastasis, respectively) were treated by surgical resection, with no further disease progression. The remaining patient, showing multiple intrahepatic metastases, underwent TACI, followed by adjuvant sorafenib. Unfortunately, portocaval lymph node metastasis then presented. In patients with locally advanced HCC, chances of systemic recurrence after liver transplantation are actually quite high.153233 Thus, early detection of tumor recurrence and active treatment might be important for survival in these patients. Although one study has addressed the utility of adjuvant treatment for HCC after liver transplantation, controversy persists.34 The recurrence pattern and prognosis will be further analyzed in future with agents of choice for adjuvant use.
This is the first-ever report of successful consecutive LDLTs in patients with locally advanced HCC and PVTT, after down-staging by using CCRT and HAIC. Nevertheless, appropriate patient selection, proper timing of transplants, and effective post-transplantation adjuvant therapy should be further investigated on a larger scale in a randomized controlled study. In the present study, median patient and graft survival of 33 months (range, 22–48 months) was achieved after initial diagnosis of HCC, compared with an expected 1-year survival of <10%.13536
In conclusion, acceptable oncologic outcomes and short-term survival times are achievable in patients with locally advanced HCC and PVTT, using a down-staging regimen of CCRT followed by HAIC. However, long-term outcomes have yet to be determined.




 XML Download
XML Download