

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Immune thrombocytopenia (ITP) in children is a disorder with favorable prognosis characterized by increased platelet destruction and decreased platelet number. It may be triggered by viral infection or immunization.1 Newly diagnosed ITP in children is usually a short self-limiting disorder without any late sequelae; in most cases, ITP lasts for several weeks or months, although in 5% to 30% of affected children, the condition becomes chronic.2345 Chronic ITP (cITP) is associated with a high risk of bleeding, such as cerebral hemorrhage, and often requires restriction of physical activities.
Various medical approaches, ranging from observation-only to aggressive management with intravenous immunoglobulin (IVIG), steroids, other immunosuppressive agents, and splenectomy have been used to treat ITP.6789 However, it is generally accepted that most of these treatments do not change the natural course of ITP. Splenectomy is commonly considered for patients without long-term responses to other therapies.
Previous studies on the outcome of cITP in children have shown that the incidence of spontaneous remission is approximately 16% at 1 year and 30% to 52% at 5 years after diagnosis. 1011 A previous Korean study conducted according to the criteria after revision reported a remission rate of 45% at about 3-4 years after diagnosis.12
It is important to predict the occurrence of spontaneous remission with the greatest accuracy possible to establish the optimal time for splenectomy in patients with cITP.13 However, there is a paucity of data on the long-term outcomes and probability of remission in children with cITP.
This study analyzed the natural course of ITP and the remission rate of children with this disorder at a single institution. We also reviewed the trends in ITP treatment at our institution by reviewing historical data.
MATERIALS AND METHODS
Patients
We retrospectively analyzed the medical records of all patients diagnosed with ITP at the Department of Pediatrics of Kyung Hee University Medical Center from January 1992 to December 2011. This population included 268 children aged 1 month to 18 years. We excluded patients who had secondary causes of thrombocytopenia and ultimately reviewed the charts of 200 patients with ITP. Study protocols were approved by the appropriate Institutional Review Boards of Kyung Hee University Hospital and complied with the declaration of Helsinki.
Diagnosis and treatment
ITP was defined as a platelet count of <100×109/L in the absence of other causes or disorders that may be associated with thrombocytopenia. We also classified ITP as newly diagnosed (≤3 months since diagnosis), persistent (3-12 months since diagnosis), and chronic (lasting ≥12 months) according to the criteria of the International Childhood ITP Working Group.14 Initial treatments comprised IVIG, steroids, anti-D immunoglobulin, and observation.
Response criteria
Complete response (CR) was defined as any platelet count of ≥100×109 with concurrent resolution of bleeding symptoms. Partial response (PR) was defined as any platelet count between 30 and 100×109/L and at least doubling of the baseline count. No response was defined as any platelet count lower than 30×109/L or less than doubling of the baseline count. The response rate (RR) was defined as the proportion of cases that experienced increases in the platelet count to >30×109/L or double the baseline after treatment.14
Statistical analysis
Statistical analysis was performed using SPSS software (SPSS Inc., Chicago, IL, USA). The results are presented as medians or means±standard deviation for quantitative variables and as percentages for non-quantitative variables. Comparisons between groups were performed using two-sample t-tests, the Kaplan-Meier method, and the Cox proportional hazard model. Differences were considered significant at p values of <0.05.
RESULTS
In total, 200 patients with ITP were identified (52% male, 48% female): 128 (64%) with newly diagnosed ITP, 31 (15%) with persistent ITP, and 41 (21%) with cITP, including 37 patients with CR and 4 with PR (Fig. 1).
No seasonal variation in the presentation of ITP was observed in this study. The median age at diagnosis was 4.5 years (1 month to 18 years). Approximately 30% of patients had a history of an upper respiratory infection before the onset of ITP. The median platelet count was 32×109/L (range, 4-98×109/L) at diagnosis. Bone marrow examinations were performed in 111 of the 200 patients (55.6%); the number of bone marrow examinations was lower between 2001 and 2011 than between 1991 and 2000 (n=36 vs. n=75, respectively) (Fig. 2).
Initial treatment involved IVIG in 96 patients (RR, 77%), observation in 61 (RR, 85%), steroids in 25 (RR, 70%), and Rho (D) immunoglobulin in 18 (RR, 72%). There were no significant differences in the RR among these therapies. The rate of clinical observation was higher between 2001 and 2011 than between 1991 and 2000 (39 vs. 22, respectively) (Fig. 2). No patients developed severe bleeding, such as central nervous system hemorrhage.
There were no differences in sex or platelet, white blood cell, and hemoglobin counts at diagnosis between patients diagnosed with persistent ITP and those with cITP (Table 1). At the time of diagnosis, patients with cITP were older than those with newly diagnosed ITP (6.6±0.3 years vs. 3.8±0.2 years, respectively). However, this difference was not statistically significant (p=0.17).
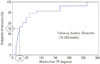
We also evaluated the remission rate in the 41 patients with cITP using the Kaplan-Meier method (Fig. 3). The median follow-up duration after the diagnosis of ITP was 56 months (range, 13-240 months). The probability of CR in patients with cITP was 50% and 76% at 2 and 5 years after diagnosis, respectively. When the age at diagnosis was less than 5 years, all children with cITP recovered spontaneously, with the exception of two patients (Fig. 4). These two patients were diagnosed with cITP at the age of <2 years and did not improve throughout a 20-year follow-up period, which was an unusual clinical situation. These patients were ultimately diagnosed with Fechtner syndrome at 17 and 23 years of age, respectively.
We also studied the prognostic factors affecting 50% remission, which refers to cases of half recovery among the cITP cases. We analyzed the following patient characteristics: age at diagnosis, sex, platelet counts at initial diagnosis and at cITP diagnosis, and treatment modalities. Age at diagnosis had a statistically significant influence: the frequency of 50% remission in patients aged <1 year at presentation was 3.8 times that of patients aged >1 year (p=0.02), even with the inclusion of the two patients with Fechtner syndrome in the analysis (Table 2). There were no significant differences among the other factors. We also investigated the relationship between Helicobacter pylori (H. pylori) infection and cITP. Unfortunately, we examined only five patients with cITP who had recently been hospitalized. All results of an H. pylori antigen test were negative.
DISCUSSION
Many treatment modalities have been used for children with cITP.1516 However, there is no gold standard for the management of children with cITP. Therefore, therapy strategies are often decided on an individual basis and are based on institutional experience.
Although splenectomy may be effective, it is associated with a considerable risk of life-threatening complications, such as post-splenectomy sepsis.17 In a study from the UK, 48% of patients (n=32) with ITP underwent splenectomy from 1950 to 1980. In the present study, splenectomy was performed in only 2 patients (1%) with cITP in 1998 and 2005, respectively. The frequency of splenectomy decreased in more recent studies.618 In addition to the invasive and irreversible nature of splenectomy, it should be noted that children with cITP have a higher probability of spontaneous remission than adults.10 Two studies reported that 26-44% of children with cITP spontaneously recovered after long-term follow-up.410 Similarly, previous Korean studies reported that approximately 45% of children with cITP recovered spontaneously about 3-4 years after the diagnosis. 12
In this study, approximately 50% and 76% of children with cITP achieved CR at 2 and 5 years after the diagnosis, respectively. These data suggest that invasive treatments such as splenectomy in children with cITP can be delayed for 4 to 5 years if thrombocytopenia and therapeutic medication do not affect the quality of life. Finally, management of cITP must be chosen on an individual basis. Additionally, two patients were ultimately diagnosed with Fechtner syndrome during long-term follow-up. Therefore, patients with cITP must be evaluated carefully for the presence of other diseases during follow-up.
The International Childhood ITP Working Group changed the definition of cITP, which had been defined as thrombocytopenia lasting for >12 months.14 A new category termed "persistent ITP" was introduced for thrombocytopenia lasting from 3 to 12 months from the time of diagnosis.14 The likelihood of spontaneous remission remains considerable during this period, which supports the delay of more aggressive therapeutic approaches. In this study, many patients achieved CR 12 to 24 months after diagnosis. Therefore, the definition of cITP may need to be changed in the future, and further studies of cITP remission are necessary.
Our study indicated a continued reduction in the number of children undergoing invasive procedures and treatments in this century when compared to historical data. We believe that these changes are caused by changes in our knowledge of ITP and its practical implications for pediatricians. Recently, we have more seriously considered various patients' circumstances, such as bleeding tendency, expected physical activity, and quality of life, rather than only platelet count when deciding how to treat ITP.
Previous studies have reported several useful predictors of cITP. The most relevant risk factors include a gradual onset of symptoms during a period of several weeks, an initial platelet count of >20×109/L, and an age of >10 years at presentation.192021 In this study, patients aged <1 year at the time of presentation had a significantly better prognosis than older patients. Age at diagnosis was the only significant factor influencing the remission of children with cITP in this study. However, our study included only four patients aged <1 year. Therefore, to obtain statistically significant results, further studies must include larger numbers of patients with cITP.
Recent reports have suggested an association between H. pylori infection and ITP.22 A high prevalence of H. pylori infection among patients with ITP and prominent improvement in platelet counts after H. pylori eradication have been reported, 23 although other studies found no evidence of such connection.2425 We also examined the association between H. pylori infection and cITP in children. Although the results of all blood and stool tests for H. pylori were negative, only five patients were examined in this respect in our study. An unequivocal demonstration of the presence or absence of an association between H. pylori infection and ITP would require testing more patients.
A limitation of this study was that it was based on a retrospective chart review. Various evaluations and treatments of children with cITP were performed in this study. A systematic multicenter prospective study of children with cITP is necessary in the future.
In conclusion, approximately 76% of children with cITP achieved CR 5 years after diagnosis. A young age at diagnosis of ITP was a significant predictor of cITP remission in this study. We suggest that invasive treatment of cITP patients aged <1 year at diagnosis should be delayed until all other treatments have been attempted for 4-5 years. Ultimately, patient management should be decided on the basis of various circumstances, such as restrictions in daily activities, fear of serious bleedings, quality of the lives of patients and their families, and burden on parents.





 XML Download
XML Download