

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Crohn's disease (CD) is a chronic inflammatory condition of the gastrointestinal tract that causes severe nutritional and emotional complications. It is characterized by periods of remission and recurrent relapses,12 and is caused by mucosal immunity dysregulation that induces overproduction of inflammatory cytokines in the bowel and leads to uncontrolled intestinal inflammation.3 The main goals in the management of CD is to induce remission and prevent relapses because this associates with improved quality of life.4 For a decade, corticosteroids were the main therapeutic option for inducing remission in patients with active CD.5 However, this approach may be less suitable for children with CD because such children already have low bone mineral density and growth delay at diagnosis. Steroid treatment may worsen these problems.
Another CD treatment option for the pediatric population is nutritional treatment. Several studies showed that this form of therapy does not associate with any side effects and leads to the recovery of linear growth.678 Consequently, the United Kingdom and many centers across Europe started recently using enteral nutrition to treat active CD. Subsequent studies then showed that nutritional therapy may be suitable as a primary treatment for active CD.910 As a result, in 2014, the European Crohn's and Colitis Organization (ECCO) issued revised consensus guidelines that recommend exclusive enteral nutrition (EEN) as the first-line treatment for inducing remission in patients with luminal CD.11 Non-adherence could negatively affect the clinical response to enteral nutrition and multitude of interacting variables including route of administration seems to paly role in adherence.
The randomized controlled trials (RCTs) by González-Huix, et al.12 and Gassull, et al.13 showed that EEN for 4 weeks induced remission in 20–88% of adults with CD. An observational study also showed that EEN for 8 weeks induced remission in 81% of children with active CD.14 Moreover, along with two other studies, it revealed, that children with CD who achieved remission after EEN may have lower relapse rates if they continue with long-term partial enteral nutrition (PEN). However, these studies were all observational studies, and enteral nutrition was often delivered by nasogastric tubes.141516 The RCT by Takagi, et al.17 also showed that patients with CD in remission had lower relapse rates if they took PEN (orally or nasogastric tube feeding) than if they had a free diet, however, these patients were all adults. Since these studies differed in terms of patient age, the type of formula, and the route of delivery, it remains unclear at present whether long-term oral PEN can be used to maintain remission in children.
Therefore, the aim of this retrospective cohort study was to determine how well oral EEN induces clinical remission in children with active CD, whether oral PEN thereafter reduces relapse rates, and which factors influence the success of EEN and PEN treatment.
MATERIALS AND METHODS
Patients
Newly diagnosed pediatric patients with CD who were managed in March 2000–January 2014 with oral EEN to induce remission and were then followed-up with oral PEN at the Asan Medical Center Children's Hospital were retrospectively included in the study.
Patients who had already received corticosteroids, immunosuppressive drugs, or infliximab before undergoing oral EEN were excluded. However, patients who received 5-aminosalicylic acid concomitantly with EEN treatment were included. Patients did not receive immunosuppressive drugs or infliximab during oral PEN treatment. Most patients who referred from other hospital for suspicion of CD and previously used corticosteroids were excluded from the study. In our hospital, we used EEN as the first therapy for induction, especially who had growth delay.
The study data were collected retrospectively from patient medical records and included demographics, clinical characteristics, and laboratory findings. The retrospective analysis was approved by the Institutional Review Board of Asan Medical Center.
CD characteristics and definitions
CD was diagnosed on the basis of a combination of the patient's history, physical and laboratory examinations, esophagogastroduodenoscopy and ileocolonoscopy with histology, and imaging of the small bowel. Indeterminate colitis, infections, and other recognized causes of intestinal inflammation were excluded by appropriate investigations.18 After confirming the diagnosis of CD, the disease status was classified according to the Paris classification system.19
Methods of oral nutritional therapy
All patients were fully informed about oral nutrition therapy and agreed to receive it. Patients shortly tried EEN at hospital for 3–4 days and who had non-adherence to treatment at this period were excluded from the study. The sole nutritional source in the study was elemental nutrition that was delivered orally (nasogastric tube feeding was not used in our study).
We used commercial product Energen® (Samil Pharmaceuticals, Seoul, Korea: 300 kcal per packet containing 63 g of glucose, 13 g of protein) until 2005 in 9 patients and thereafter we used Monowell® (Korea Medical Food, Seoul, Korea: 400 kcal per packet containing 50 g of glucose, 16 g of protein and 15 g of fat) in 57 patients. Monowell® has been provided free of charge according to the program run by the Korean Government of Ministry of Health and Welfare for the treatment of pediatric Crohn's disease patients since 2005. To induce remission, approximately 2400 Cal. (2.4 L)/1.73 BSA was delivered by the oral route for six weeks. During this period, patients were allowed unsweetened tea or water but no other food. The total daily calorie goal was achieved gradually by the first 3–4 days.
After the induction period, the patients received two meals per day that were composed of PEN (400–800 Cal./day) and one meal with free food. After 3 or 4 months later, this changed to one PEN meal and two meals with free foods.
Patients who were unable to consume an adequate volume of the formula were defined as non-adherence to enteral nutrition. Patients' adherent was checked by reviewing medical records at regular follow-up. All patients visited hospital at regular follow-up period.
Clinical assessment
The disease and nutritional status of each patient was assessed before therapy and at regular follow-up visits after the initiation of therapy. Clinical disease activity was assessed at diagnosis and at each visit by using Pediatric CD Activity Index (PCDAI) scores.20 Clinical remission was defined as a PCDAI score <10. Relapse was defined when the PCDAI score was >10 and clinical symptoms had recurred. The disease severity was classified as mild (10≤PCDAI<30), moderate (30≤PCDAI<40), or severe (PCDAI≥40).21 Nutritional status and growth were assessed by calculating the z-scores for weight for height, height for age, and body mass index.
The efficacies of oral EEN at six weeks and oral PEN in the two years after starting the oral EEN period were evaluated.
Statistical analysis
Continuous variables were expressed as medians with ranges. Discrete data were expressed as numbers and percentages. The two groups were compared in terms of continuous variables by using the Mann-Whitney U test and in terms of the categorical variables by using the Fisher's exact test or chisquare test. The cumulative proportion of patients who maintained remission was calculated by using the Kaplan-Meier method. Differences between Kaplan-Meier curves were compared using a log-rank test.
RESULTS
Ability of EEN to induce remission and identification of factors contributing to failure
In total, 66 patients started the six weeks EEN induction course and 61 (92%) completed it. Because of poor taste of formula and consistent nausea, five patients couldn't continue EEN after two weeks from initiation. Sixty one patients were compliant with the six weeks induction EEN course, and 58 (95%) achieved clinical remission. When treatment outcome was based on all initiated courses of EEN, 58 of the 66 patients (88%) achieved clinical remission. Clinical remission was achieved with EEN on average 26 days (range: 5–85 days) after starting induction EEN.
Table 1 shows the baseline characteristics of the patients who did (n=58) and did not (n=8) achieve clinical remission. Patients with inflammatory disease behavior (B1) had a significantly higher clinical remission rate than patients with stricturing disease behavior (B2) (93.1% vs. 62.5%, p=0.033). The median PCDAI score at diagnosis was not different between two groups (35.3 vs. 35.9, p=0.692).
Ability of PEN to maintain remission and identification of factors contributing to failure
All of the 58 patients who achieved clinical remission received maintenance treatment with PEN. Of these, 43 (74%) adhered to the PEN treatment. Among the 43 PEN-compliant patients, 32 (73%) maintained clinical remission. When treatment outcome was based on all maintained courses of PEN, 32 of the 58 patients (55%) maintained it. Maintenance treatment with PEN was continued on average for 16 months (range: 3–60 months).
Table 2 shows the baseline characteristics of the patients who did (n=32) and did not (n=26) maintain clinical remission with PEN. Differing from EEN treatment, the median PCDAI score at diagnosis was significantly higher in maintenance failure group with PEN (42.2 vs. 32.9, p=0.040).
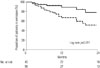
Of the 58 patients who achieved remission and underwent PEN, 27 and 13 continued PEN for more than 1 and 2 years, respectively. About 67% and 52% of these patients maintained clinical remission 1 and 2 years after starting PEN, respectively (Fig. 1, lower curve). When treatment outcome was based on PEN-compliant patients, 86% and 78% of the adherent patients maintained clinical remission 1 and 2 years after starting PEN, respectively (Fig. 1, upper curve).
Adherence to oral enteral nutrition
In total, 5 and 15 patients did not adhere to oral induction EEN and oral maintenance PEN, respectively. Thus, in total, 20 of the 66 patients (30%) did not adhere to EEN or PEN. Comparison of the adherent and non-adherent children revealed that non-adherent children were more likely to be female than the adherent children (58.3% vs. 24%, p=0.019). The median PCDAI score at diagnosis was not different between two groups (39.2 vs. 33.7, p=0.154).
DISCUSSION
This retrospective study showed that in the adherent patients, oral EEN induced clinical remission in about 95% and oral PEN cumulatively maintained remission in about 78% during an average follow-up period of two years.
Several studies have shown that EEN therapy is useful for children with CD. A review of five RCTs in 2000 showed that EEN was as effective as corticosteroids in terms of inducing remission in children; moreover, it improved growth and development. These effects were achieved without the side effects of steroid therapy.7 A subsequent RCT in 2006 by Berni Canani, et al.5 also showed that EEN yielded clinical remission rates similar to steroid treatment; it also had more pronounced effect on mucosal healing and associated with more sustained remission. However, given the lack of guidelines regarding the route of ingestion and the type of formulas during this period, the centers participating in these RCT used quite different methods and types of formula. Thus, it remains unclear at present whether one method is superior to the others.
Non-adherence with enteral nutrition can occur frequently in children and may limit the success of treatment. Indeed, our study found that 5 of 66 and 15 of 58 of our pediatric patients were not adherent to induction EEN and maintenance PEN, respectively. Several other studies report non-adherence rates of 0–40%.2223 Adherence rates may be influenced by race since the Dutch study by de Bie, et al.24 found that non-adherence was high in children from non-Dutch parents. They also showed that older children and females were particularly likely to be non-adherent. Similarly, we observed that female gender associated with non-adherence (p=0.019). They also found that patients taking hyperosmolar sip feeds were less adherent than children receiving continuous polymeric formula via a nasogastric tube. However, Rubio, et al.25 found that children receiving fractionated oral EEN were as adherent as children receiving continuous EEN and had similar remission rates.
Adherence to enteric feeding therapy in children may also be hampered by the use of a nasogastric tube to deliver the formula as most children are afraid of tube feeding. As a result, the newly revised consensus guidelines of ECCO recommend that feeds should be given orally by using a whole protein formula.11 While the expense and poor palatability of enteral nutrition could still hinder adherence, this problem could be overcome by using polymeric formula, which is significantly less expensive and more palatable than elemental formula, and two RCTs showed that it has similar efficacy.2627 Financial governmental support could also improve adherence: in our country, the national insurance system pays half of the price if patients choose oral elemental formula.
A systematic review has shown that disease location can affect the efficacy of EEN.28 For example, Afzal, et al.29 showed that isolated colonic disease does not respond to EEN as much as ileocolonic or ileal disease. Conflicting data regarding efficacy of EEN on perianal disease have been also reported. Wong, et al.30 showed significant improvement in symptoms, PCDAI, and mucosal healing in three CD patients with perianal disease who were managed with EEN. However, we did not detect an association between disease location and treatment outcome. Instead, we observed that disease behavior influenced EEN success. Compared to patients who achieved remission, patients who did not achieve remission were more likely to have stricturing behavior disease (B2) and less likely to have inflammatory behavior disease (B1).
A systematic review in 2010 of ten studies suggested that PEN as maintenance therapy may be useful for maintaining remission; however, it was also noted that the level of evidence for this notion was not high.31 Moreover, there are only a few studies on the effect of maintenance therapy in children with CD.1416 Similar to these studies, we found that children who achieved remission with EEN were likely to maintain remission if they continued with maintenance therapy with PEN. However, our study differed from the preceding studies in that all of our patients received enteral nutrition orally; by contrast, the preceding studies administered the feeding by nasogastric tube only or by a mixture of nasogastric tube and oral feeding. Prospective study by Kang, et al.8 reported that short-term PEN was effective in simultaneously improving nutritional status and disease severity in severe CD. In this study, however, the therapeutic effect of PEN was limited in severe CD patients. More aggressive or combined treatment with other medications may be needed in these patients.
How induction EEN and maintenance PEN induced and maintained remission, respectively, in this study, is not clear. Several hypotheses have been proposed, including the possibility that the low-fat content and poor antigenicity of the formula quiet the inflammation that drives CD. This is supported by the prospective study of Yamamoto, et al.3 This study consisted of 40 patients with quiescent CD, half of whom received nighttime enteral nutrition and a low-fat diet during the daytime; the remaining patients did not receive enteral nutrition or diet restrictions. After 12 months, the enteral nutrition group had much lower endoscopic inflammation scores and significantly lower mucosal tissue levels of interleukin (IL)-1beta, IL-6, and tumor necrosis factor-alpha, which are suspected to play critical roles in modulating and exacerbating intestinal immune reaction.32 However, double blind randomized study by Leiper, et al.33 showed no difference in the response of active CD to whole protein feeds that have a high content of long chain triglyceride (30% vs. 5%). In our study, although the number of patients who had low fat formula was small, any significant difference in treatment success was not shown between two groups.
Another possible mechanism underlying the effect of EEN and PEN in CD is that the enteric feeding alters the bacterial flora in the intestines. There is considerable evidence that suggests that the intestinal microflora contributes to the pathogenesis of CD.34 When Lionetti, et al.35 analyzed the biodiversity of the fecal microflora of children with CD by 16S rRNA polymerase chain reaction, they found that patients treated with 8 week EEN, followed by maintenance PEN, exhibited profound modification of the fecal microflora after both EEN and PEN.
This study has several limitations. First, it only involved a single center. Second, it was retrospective, and the patients were therefore not randomized. Third, the follow-up period was relatively short. Fourth, remission was evaluated by only measuring PCDAI. To assess the true efficacy of enteral nutrition, both clinical activity and intestinal (mucosal) inflammation should be assessed. Fifth, a control group to assess the efficacy of PEN was not employed. Nevertheless, this is the first study to evaluate the efficacy of and adherence to oral induction EEN and oral maintenance PEN in an Asian pediatric population. While it suggested that PEN prolongs remission and reduces relapse rates, well-designed prospective studies that test the effect of long-term enteral nutrition are warranted. Adherence issues should also be considered to improve treatment success.
In conclusion, oral EEN and PEN effectively induced and maintained remission in pediatric CD, respectively. Differing from EEN, therapeutic effect with PEN could be decreased in severe CD patients. Non-adherence was a limiting factor in the success of therapy.


 XML Download
XML Download