

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Abbou, et al. first performed robot-assisted radical prostatectomy (RARP) in 2000.1 Since then, the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) has been used in South Korea to conduct various types of urological surgery including radical prostatectomy, partial nephrectomy, and radical cystectomy, beginning in 2005.2 Radical prostatectomy is considered the gold standard of surgical treatment.3 However, the demand for RARP has increased due to better defined surgical anatomy and improved surgical maneuverability.2 Thirty-six da Vinci robotic surgery platforms are currently in use throughout 30 hospitals in Korea. A total of 24207 (24337 cases) patients underwent robotic surgery from 2005 to 2012, and the average annual growth rate for robotic surgery was 51.4% from 2005 to 2011. One-third (33.7%) of all robotic surgeries in the world were RARP; this was the most commonly performed robotic procedure.4
In 2013, the Korean government announced plans to radically enhance health insurance coverage for major conditions including cancer. Robotic surgery to treat prostatic cancer was to be included in the discretionary benefits list by as early as 2015.5 However, its inclusion has been questioned by some, since the comparative effectiveness of robotic surgery remains unclear. In previous reviews of RARP versus retropubic radical prostatectomy (RRP), RARP yielded better peri-operative outcomes.67 However, the evidence suggesting that RARP is associated with a decrease in urinary incontinence, improved potency, and reduction in biochemical recurrence (BCR), compared to RRP is limited. This is because most publications had a high risk of bias and exhibited extensive patient heterogeneity. While some experts have argued that the extension of discretionary benefits to robotic surgery increases patient choice, others point out that, without scientific evaluation, expansion of coverage will undermine the National Health Insurance system because demand will explode.8
Accordingly, the aim of the present paper was to comprehensively review and update data on the efficacy and safety of RARP versus RRP in patients with prostate cancer.
MATERIALS AND METHODS
Inclusion criteria
Studies eligible for inclusion consisted of randomized controlled trials and prospective and retrospective cohort studies that compared RARP and RRP. A study was excluded if it did not report any outcome of interest (i.e., safety or functional and oncological outcomes).
Search strategy
We systematically reviewed recent research using techniques that evaluated comparative effectiveness, as suggested by the Agency for Healthcare Research and Quality.9
Existing systematic reviews and health technology assessment reports were identified by searching ovidMEDLINE, ovidEMBASE, the Cochrane Library, KoreaMed, RISS4U, KISS, KISTI, KMbase, and NDSL from January 1980 to August 2013. We used combinations of MeSH terms and the following phrases: exp Prostatic Neoplasms/or prostatic cancer, exp Robotics/ or exp Surgery; and Computer-Assisted/or robot*/or (da vinci or davinci) (Supplementary Table 1, only online). In addition, we scanned the reference lists of relevant reviews and reports by international health technology assessment agencies to ensure comprehensive data collection. We then searched for recent studies (published from January 2010 to September 2013), because two high-quality systematic reviews (HIQA10; Ramsay, et al.11) had only searched primary studies up to March 2011. We did not restrict publication language.
Two authors independently reviewed all titles and abstracts and retrieved full-texts of all studies potentially meeting inclusion criteria. If the reviewing authors disagreed, the conflict was resolved by discussion and consensus, or by consulting a third member of the review team. We used structured data extraction forms to gather pertinent information; this included characteristics of the country of publication, study design, study participants, interventions, comparisons, outcome measures, outcome definitions, follow-up durations, and results that were statistically significant. If information was unclear or missing, we contacted the original authors by e-mail.
Quality assessment and data synthesis
Two reviewers independently assessed the risk of bias. Systematic reviews were evaluated using the Revised Assessment of Multiple Systematic Reviews (R-AMSTAR) tool,12 and non-randomized studies newly published after 2010 were evaluated using the modified Cochrane Risk of Bias tool.11 The modified RoB tool is composed of seven specific domains: random sequence generation (selection bias), allocation concealment (selection bias), controlling for confounding (selection bias), blinding (performance and detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and other sources of bias (regarding funding source). Any disagreement was resolved by discussion.
Meta-analysis was performed using Revman 5.2 and Comprehensive Meta-Analysis (CMA) version 2.0. For continuous outcomes, weighted mean differences or standardized mean difference and 95% confidence intervals (CIs) were calculated using the random-effects model of the Dersimonian-Laird method.13 Mantel-Haenszel risk ratios (M-H RRs), with 95% CIs, derived using a random effects model, were calculated if outcomes were dichotomous.14 Heterogeneity was assessed using the I2 and Q statistics. An I2>50% was considered to indicate substantial heterogeneity.15 With the Q statistic, heterogeneity was deemed to be significant if p<0.10. Publication bias was tested by Funnel plotting and using Egger's test.16
RESULTS
Details of included studies
An overview of the study selection process is provided in Fig. 1. We used two existing systematic reviews on RARP in patients with prostate cancer as the best-available evidence, which included 38 studies. An additional twenty-three studies were included through new searches for updates. Finally, we evaluated 61 articles, none of which was a randomized controlled clinical trial (Supplementary Table 2, only online). In characteristic of the included studies, the average age of the participants ranged from late fifties to sixties, which were similar between the two procedures. Of the 61 studies, 14 reported significantly different pre-operative prostate-specific antigen (PSA) levels. Also, 22.9% of the included studies reported significantly higher clinical stages for RRP patients than for RARP patients.
Quality assessment results
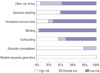
The summary of risk of bias in the cohort studies is shown in Fig. 2. In this evaluation, random sequence generation and concealment of allocation to group were considered to be important in terms of estimating any treatment effect. Most studies were flawed in this respect. Accordingly, most of the studies were susceptible to selection bias. Blinding domain was rated as a low risk of bias because of objective outcome measures or patient reported outcomes using valid and reliable questionnaires. In the selective outcome reporting domain, approximately 40% of the included studies were rated as having a high or unclear risk of bias, because those studies did not investigate all of the outcomes of interest in this review.
Perioperative outcomes
Complications
There was no significant difference in the rates of anastomosis site leakage (eight studies with 4880 participants; RR 0.78, 95% CI 0.47–1.28; p=0.330), infection (six studies with 7373 participants; RR 0.37, 95% CI 0.09–1.54; p=0.770), ileus (six studies with 2437 participants; RR 0.82, 95% CI 0.41–1.66; p=0.580), or deep vein thrombosis (five studies with 4576 participants; RR 0.75, 95% CI 0.39–1.46; p=0.400) between RARP and RRP in the selected studies (Supplementary Table 3, only online). However, RARP was associated with lower rates of bladder neck contracture (five studies with 2846 participants; RR 0.26, 95% CI 0.09–0.73; p=0.010), organ injury (ten studies with 6715 participants; RR 0.54, 95% CI 0.30–0.99; p=0.040), and pulmonary embolism (three studies with 3159 participants; RR 0.24, 95% CI 0.07–0.83; p=0.002), compared to RRP (Supplementary Fig. 1A, B, and C, respectively, only online). Transfusion data were reported in 25 studies (10605 participants). Although high degrees of study heterogeneity were evident, RARP was associated with a lower risk of transfusion than RRP in both prospective (12 studies with 6038 participants; RR 0.19, 95% CI 0.11–0.30; p<0.001) and retrospective studies (13 studies with 4567 participants; RR 0.14, 95% CI 0.07–0.30; p<0.001) (Supplementary Fig. 1D, only online).
Clavien-Dindo classification
Data from 19 studies (12175 participants) indicated a slight, but significant, difference in Clavien-Dindo complication rates after RARP, compared to RRP (RR 0.37, 95% CI 0.25–0.55, I2=84%; p<0.001). When complications were classified by severity, Clavien-Dindo I–II scores (11 studies with 5295 participants) and Clavien-Dindo III–V (8 studies with 6880 participants) scores suggested that RARP was associated with a decreased risk of Clavien-Dindo scores of I–II (RR 0.27, 95% CI 0.16–0.46, I2=88%; p<0.001) However, studies reporting such outcomes exhibited substantial heterogeneity (Supplementary Fig. 1E, only online).
Operation time
RARP was associated with longer operating times than RRP (25 studies with 8080 participants; mean difference 32.27 min more; 95% CI: 12 to 52.54 min; p=0.002). Heterogeneity among study data was high (I2=98%) (Supplementary Fig. 1F, only online).
Length of stay
Hospital days were reported in 27 studies (7939 participants). Sub-group analysis was carried out by classifying countries into the US, Asia-Pacific, and Europe. RARP was associated with shorter hospital stay in the US (13 studies with 5112 participants; mean difference -0.66 days, 95% CI -1.19–-0.14; p=0.010), Asia-Pacific (five studies with 1256 participants; mean difference -3.39 days, 95% CI -4.11–-2.67; p<0.001), and Europe (nine studies with 1571 participants; mean difference -1.81 days, 95% CI -2.76–-0.86; p<0.001). Considerable heterogeneity was evident between studies (I2=99%), possibly attributable to differences in healthcare systems (Supplementary Fig. 1G, only online).
Functional outcomes
Incontinence rate at 12 months
Based on the results of 11 studies (participants: 2510), RARP was associated with reduced urinary incontinence 12 months after surgery, compared to RRP (RR 0.62, 95% CI 0.42–0.93, I2=47%; p=0.020) (Fig. 3A). In order to consider differences in baseline characteristics of participants, subgroup analysis was performed. In 10 studies with a similar pre-operative PSA level between groups, urinary incontinence rate at 1 year after surgery was lower for RARP than for RRP (participants: 2214; RR 0.66, 95% CI 0.45–0.99, I2=45%; p=0.040). Also, pre-operative clinical stage for all of the studies was not significantly different between procedure groups.
Potency rate at 12 months
Based on the results of 10 studies (participants: 2142), RARP was found to be associated with improved postoperative potency rate, compared to RRP (RR 1.41, 95% CI 1.18–1.70, I2=65%; p<0.001) (Fig. 3B). In addition, nine studies (participants: 1956) with a similar pre-operative PSA level between groups demonstrated favorable potency rate for RARP (RR 1.41, 95% CI 1.16–1.72, I2=63%; p<0.001). In eight studies (participants: 1965) with comparable pre-operative clinical stages between groups, RARP was associated with higher recovery of erectile function (RR 1.37, 95% CI 1.12–1.67, I2=69%; p=0.002).
Oncological outcomes
Positive margin rates
Positive margin rates for RARP were equivalent to those for RRP in both prospective (13 studies, 6226 participants; RR 0.95, 95% CI 0.74–1.23, I2=80%; p=0.72) and retrospective studies (23 studies, 12813 participants; RR 0.88, 95% CI 0.75–1.03, I2=71%; p=0.110) (Fig. 4A). However, the heterogeneity among the results of individual studies was considerable. Sensitivity analysis was performed with only low risk studies (seven studies with 1412 participants; RR 0.93, 95% CI 0.67–1.30, I2=65%; p=0.670) (Fig. 4B) and for pT2 tumors in studies published after 2010 (7 studies with 2321 patients; RR 0.73, 95% CI 0.45–1.19, I2=73%; p=0.210) to determine the effect of removing any outliers. However, there was still moderate heterogeneity (Fig. 4C).
Biochemical recurrence
Fourteen studies (8259 participants) reported recurrence of prostate cancer, defined at various cut-off values of >0.4 ng/mL, >0.2 ng/mL, ≥2 ng/mL, >0.1 ng/mL, or ≥0.1 ng/mL. Therefore, the subgroup analysis was performed according to definition of PSA failure. Rates of BCR were reported in five studies (1485 participants) using the definition PSA level >0.2 ng/mL.1718192021 RARP was associated with a reduced risk of BCR, compared to RRP (RR 0.71, 95% CI 0.61–0.81, I2=0%; p<0.001) (Fig. 5A). Subgroup analysis according to follow-up duration demonstrated a similar recurrence-free survival between the two procedures upon long-term follow up (Fig. 5B).
Publication bias
Publication bias for each outcome was tested using Egger's regression test, and showed only one example of publication bias associated with reported transfusion rates (Supplementary Table 4, only online). So, trill and fill analysis was performed to adjust the publication bias. After excluding eight studies by trim-and-fill analysis, the risk ratio of transfusion rate was still lower in RARP than in RRP (RR 0.26, 95% CI 0.17–0.38).
DISCUSSION
To explore the supposed superiority of robotic platforms in treating prostate cancer, we performed a systematic review of all research published to 2013 that compared RARP with RRP. We found no randomized controlled study in which the two modalities were compared. Thus, we included only 61 non-randomized studies, of which 20 were prospective and 41 were retrospective. Studies were regarded as being of high quality if three of four domains (random sequence generation, confounding, blinding, and incomplete outcome reporting) were judged to have a low risk of bias. Only 13 (21.3%) publications met these criteria, and the risk of bias in most of the studies might confound the true effects of RARP.
Since 2010, 23 systematic reviews have been published, and they reported various outcomes. Our systematic review included recently published studies and reflects comprehensive primary outcomes, including perioperative outcomes, functional outcomes, and oncologic outcomes. Compared to open surgery, RARP yielded superior outcomes in terms of complications, such as organ injury, pulmonary embolism, and bladder neck contracture. In addition, the risk of overall complications assessed using the Clavien-Dindo classification was lower for RARP than RRP, although a high level of study heterogeneity was evident. Notably, the risk of complications after RARP was significantly lower than that after RRP, unlike earlier reports.711 Our findings are in line with results reported elsewhere. That is, a population-based observational cohort study using US Surveillance, Epidemiology, and End Results Medicare-linked data found that minimally invasive radical prostatectomy with or without robotic assistance was associated with lower rates of postoperative respiratory complications (4.3% vs. 6.6%; p=0.004), miscellaneous surgical complications (4.3% vs. 5.6%; p=0.03), and anastomotic stricture (5.8% vs. 14.0%; p<0.001), compared to RRP.22 In addition, RARP postoperative courses based on claims made to the South Korean Health Insurance Review and Assessment Service from September 2005 to December 2011 might be lower than RRP. Totals of 1830 and 1660 patients underwent RARP and RRP, respectively, and postoperative complication rates to 30 days as measured by re-admission to intensive care units were 0.1% and 0.2%, respectively.23 Thus, we suggest that RARP can be performed with a reasonably low complication rate.
In the present study, RARP was associated with better perioperative outcomes than RRP in terms of operation time and length of hospital stay, consistent with findings of previous systematic reviews and meta-analyses.724 In addition, claims data from South Korea showed that RARP-associated hospital stays were shorter than those for RRP (RARP 9 days vs. RRP 12.7 days). We sought to explore heterogeneity in pooled estimates of operative time by performing subgroup analysis according to the definition of operative time, but could not do so because most studies did not describe how they measured the duration of surgery. Only four studies reported durations of surgery as follows: from skin incision to skin closure time in both procedures;25 from insertion of the Veress needle (RARP) to the suture of the last laparoscopic port, and skin incision to suture (RRP);26 as the time from incision to placement of dressings;27 and as the mean operative time of hernia repair.28
Our results are comparable with those of a propensity-score matching study that adjusted for among-series differences in preoperative Gleason scores, preoperative PSA levels, and pathological stages. The cited work comprised a systematic review and meta-analysis of RRP, laparoscopic radical prostatectomy, and RARP patient series, and found that the rate of perioperative complications was significantly lower for RARP than RRP.24
The prevalence of urinary incontinence and erectile dysfunction after RARP are affected by preoperative patient characteristics (age, body mass index, and comorbidities), the experience of the surgeon, the surgical technique used, and methodological features, such as the definitions of continence and potency, outcome measures, and follow-up periods.29 To optimize our evaluation of functional outcomes, we included only outcome data obtained using objective measures or reliable and valid measurement instruments. In detail, the definition of continence was the use of no pad at all, 0–1 pads per day, or no leak measured by a validated questionnaire including the International Consultation of Incontinence Questionnaire-Urinary Incontinence; and that for erectile function a positive response to a validated questionnaire reporting erection sufficient for intercourse with or without prescription of a phosphodiesterase type 5 inhibitor or a score >17 on the Sexual Health Inventory for Men or 5-item version of the International Index of Erectile Function validated questionnaires exploring erectile dysfunction.
In this review, urinary incontinence and erectile function recovery rates measured at 12 months after RARP were lower than those after RRP. Our findings suggest positive functional outcomes of RARP, because of an increase of magnitude in effect size, compared to previous systematic review.11 The beneficial effects on the functional outcomes of RARP, compared to RRP, remained even in meta-analysis that added the study findings recently reported by Haglind, et al.30 [incontinence rate: 12 studies, 4937 participants, RR (M-H, random) 0.68, 95% CI 0.47–0.98, I2=62%; potency rate: 11 studies, 4564 participants, RR (M-H, random) 1.36, 95% CI 1.18–1.57, I2=61%].
The positive effect of functional outcomes of RARP is attributable to developments in surgical technique: nerve sparing improves both continence and potency, because the urethral rhabdosphincter receives afferent fibers from the traversing bundle.31 On robotic platforms, three-dimensional-magnified views allow meticulous dissection of both the periprostatic fascia layer and the neurovascular bundle. New insights into the multilayer structure of the periprostatic fascia and the course of the cavernous nerves have supported the development of intra- or inter-fascial surgical planes, enabling the urinary and sexual functional outcomes to be improved. Developments in RARP operative techniques improving urinary function, such as puboprostatic-sparing approaches, bladder neck preservation, selective dorsal vein complex division, nerve-sparing mechanisms, reconstruction of the posterior musculofascia, and anterior restoration of the pelvic space, are advocated. Meanwhile, several physician-reported studies showed incontinence rates ranging from 10 to 15% at 12 months after radical prostatectomy.3233 Considering that an acceptable incontinence rate is about 10%, regardless of the surgical technique, two studies included in this review might be performed by under-experienced surgeons due to a high incontinence rate, reaching 25 to 30%.3435 Urinary incontinence and erectile dysfunction are highly problematic conditions affecting many aspects of quality of life, and healthcare providers must be aware of this.363738 Although a randomized controlled study was not included in this review, our results suggest that healthcare providers should consider patient preferences in terms of recovery of urinary and erectile function when choosing between RARP and RRP, even though disparities in the receipt of RARP in terms of demographic characteristics, such as household income and insurance status, were reported.39
The rate of positive surgical margins was comparable between RARP and RRP (RR 0.95, 95% CI 0.74–1.23, I2=80%). In sensitivity analysis to explore the heterogeneity, our results did not change in the analysis restricted to studies rated as low risk of bias and for pT2 tumors studies published after 2010. The results were consistent with the findings of previous systematic reviews.22 Pooled estimates from 15 studies published from 2004 to 2011 showed that RARP is associated with a lower rate of positive surgical margins for pT2 tumors (RR 0.63, 95% CI 0.49–0.81, I2=27.7%).5 However, we suggest that our findings reflect more recent evidence of the comparative effectiveness of RARP versus RRP. Furthermore, this result was consistent with the recent cohort study investigating long-term oncologic outcomes, including positive surgical margins, in RARP compared to RRP (between group comparison p=0.230).40
In the present review, RARP was associated with a lower rate of BCR, compared to RRP, regardless of the manner in which such recurrence was defined (14 studies with 8259 patients; RR 0.71, 95% CI 0.54–0.93, I2=72%). To explore the effect of heterogeneity, we classified studies in terms of their definition of PSA failure, and selected PSA >0.2 ng/mL as an optimal criterion based on clinical practice guidelines.41 Upon subgroup analysis, RARP was superior to RRP in this context (five studies with 1485 patients; RR 0.71, 95% CI 0.61–0.81, I2=0%); heterogeneity was not an issue in this subgroup. This result is inconsistent with that of an earlier meta-analysis (hazard ratio 0.9, 95% CI 0.7–1.2, p=0.526), which reported differences in the definition of BCR-free survival.42 In additional analysis according to follow-up period, PSA failure rates were significantly lower in RARP than in RRP in a short term follow-up of 1 year or less. However, PSA failure rates between the two procedures were similar in long-term follow up.
Our present review had several limitations. First, significant oncologic and functional heterogeneity was evident; surgical skills and experience vary. Second, no randomized controlled trial has been conducted. Third, virtually no significant report on cancer-specific mortality rate following RARP has been published, because of the long follow-up needed in prognostic studies on clinically localized prostate cancer and the fact that RARP is a relatively new procedure.
In conclusion, we found that RARP might be favorable to RRP in aspects of post-operative complications, peri-operative outcomes, and functional outcomes, including urinary and erectile function. Also oncologic outcomes, such as positive margins and BCR, were comparable between two groups. However, most included studies were non-randomized studies and moderate to substantial heterogeneity was evident. Therefore, we suggest that further high quality studies minimizing selection, confounding, and selective reporting biases with longer-term follow-up are needed to determine clinical efficacy and safety of RARP.




 XML Download
XML Download