

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Over the last decade, robot-assisted laparoscopic radical prostatectomy (RALP) has been increasingly adopted worldwide as a surgical treatment option for localized prostate cancer.12 The robotic technology features a magnified operative field that aids the surgeon in the identification of key anatomical landmarks, therefore facilitating the challenging steps of the procedure, such as the bladder neck dissection and the nerve-sparing (NS) dissection.3
It has been postulated that the presence of a median prostatic lobe might translate into an additional challenge during a RALP procedure, particularly during the dissection of the bladder neck, and several studies have addressed this issue, mainly by focusing on the potential additional risk of positive surgical margins.45678
Recently, intravesical prostatic protrusion (IPP) has been identified as a measurable predictor of bladder outlet obstruction in patients with benign prostatic hyperplasia910 and it can be regarded as a more objective and accurate way of assessing a median prostatic lobe. The role of IPP in patients undergoing RALP remains to be addressed, particularly regarding its impact on postoperative urinary continence, which represents a primary functional outcome influenced by several factors.11
The aim of this study was to analyze the association between the grade of IPP and the outcomes of RALP, particularly in relation to the recovery of urinary continence.
MATERIALS AND METHODS
Study design
A prospectively maintained single-institution RALP database was queried for the purpose of this study after approval from the Institutional Review Board. Medical records of 1094 men who underwent RALP for prostate cancer from January 2007 to June 2013 at Seoul National University Bundang Hospital were retrospectively reviewed. We excluded 259 patients who presented insufficient data as well as 14 patients who did not have an MRI image. Ultimately, we analyzed 821 patients who underwent RALP.
A standardized preoperative assessment included patient and tumor characteristics: age at surgery, Charlson Comorbidity Index (CCI), prostate specific antigen (PSA) at biopsy, prostate volume, presence and grade of IPP, tumor clinical stage, and biopsy Gleason score.
For the purpose of the study, all patients were stratified into three preoperative risk groups based on prostate cancer characteristics at diagnosis according to National Comprehensive Cancer Network (NCCN) guidelines.12 Patients who received neoadjuvant or adjuvant hormonal or radiation therapy were not included in the present analysis. Two experienced uroradiologists performed transrectal ultrasonography (TRUS) and TRUS biopsy, and a single experienced uropathologist the examined prostate specimen. We assessed pathologic stage, pathologic Gleason score, extracapsular extension, seminal vesicle invasion, lymph node invasion, and positive surgical margin according to IPP status.
Surgical technique
A NS technique was performed according to the method described by Srivastava, et al.13 The NS status (non-NS, unilateral NS, bilateral NS) was defined by each operating surgeon in the operative report. The indication for an NS procedure was given on a cases-by-case basis according to the patient and tumor characteristics.
Assessment of IPP
The IPP was assessed with the patient in the supine position using transrectal prostate ultrasound with a bladder volume of 100 to 200 mL. The IPP was measured as the vertical distance from the longest distance of the protrusion to the base of the urinary bladder in the mid-sagittal plane of TRUS (Fig. 1).
Assessment of postoperative urinary continence
Continence rates were estimated according to the patient-reported pad usage per day. We evaluated follow-ups at 1, 3, 6, and 12 months postoperatively and at every 6 months thereafter. Postoperative urinary continence (UC) recovery was defined as cessation of pad use.
Analysis
The characteristics of patients were analyzed using Student's t-test and the chi-square test. Chi-square analysis was used to compare the rates of continence between patient groups, namely group A (patients with IPP) and group B (without IPP).
A logistic regression analysis was performed to study the independent predictive value of main risk factors [age, body mass index (BMI), prostate volume, PSA, Gleason score, CCI, nerve sparing status, and IPP grade] in regard to postoperative continence at postoperative 12 months. We assessed the predictor of postoperative continence using a generalized estimating equation (GEE) model, which could account for the correlation structure at the same time.
SPSS 22.0 for Windows (IBM® SPSS® version 22.0, IBM, Armonk, NY, USA) was used for all statistical analyses. A p value of <0.05 was considered to be statistically significant.
RESULTS
The characteristics of the patients are listed in Table 1. Of the 821 total patients included in our study, 180 (21.9%) had IPP, while 641 (78.1%) did not. Patients with IPP were older (p=0.03) and presented a larger prostate volume (p<0.001), and more non-NS RALP procedures were performed among them (p<0.001). The median age of the IPP group was 68 years [95% confidence interval (CI): 63–72], and the median age of the non-IPP group was 67 years (95% CI: 61–71).
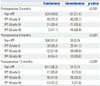
Table 2 shows the correlation between preoperative IPP and continence status after RALP. As the IPP grade increased, continence rates were found to decrease at 3 months (p<0.001). Similar patterns of continence rates were observed according to IPP grade at the 6-month follow-up as well as at 12 months (p<0.001). The grade 3 IPP group showed a lower probability of continence recovery at all time points after RALP than the non-IPP and Grade 1 and 2 IPP groups.
On multivariate analyses, age and IPP status were found to be independent predictors of postoperative continence [odds ratio (OR): 1.068 (1.018–1.121), p=0.007; OR: 7.614 (4.244– 13.663), p<0.001, respectively] (Table 3).
There was no statistical difference in pathologic outcome according to IPP status (Table 4).
DISCUSSION
Our study findings suggest that the presence and grade of IPP, as measured via preoperative TRUS, are significantly related to early recovery of urinary continence after RALP. In addition, the grade of IPP has an impact on continence recovery at 12 months after surgery. To the best of our knowledge, these findings have not been reported elsewhere.
TRUS is more accurate than transabdominal ultrasonography due to the minimal effect of urine volume during the measurement of IPP.10 The IPP grade can also be determined according to the protrusion length from the bladder neck. In a recent study, the protrusion of the median lobe was measured using preoperative MRI and was found to significantly correlate with positive surgical margins at the base during RALP.5
Several factors have been investigated as key players in the pathophysiology of urinary incontinence after RALP.11 The mechanism of IPP impact on continence status after RALP remains unclear and multifactorial.
The first hypothesis is associated with bladder outlet obstruction and subsequent bladder dysfunction. IPP was found to be a more accurate predictor of bladder outlet obstruction than PSA level or prostate volume.15 Konety, et al.16 analyzed the impact of prostate volume using data from the CaPSURE Database and reported that prostate volume is correlated with continence status up to 2 years after surgery. They suggested that subclinical bladder dysfunction related to benign prostatic hyperplasia might present after a radical prostatectomy procedure. Previous studies reported the correlation of IPP with the storage symptom scores of the International Prostate Symptom Score (IPSS).1718 Another study reported the relation between significant IPP (IPP≥5 mm) and improvement in the IPSS and IPSS storage symptom score after transurethral resection of the prostate.19 Thus, a higher grade of IPP would have a higher degree of subclinical bladder dysfunction before RALP, resulting in a lower rate of urinary continence after RALP.
The second hypothesis is related to the bladder neck preservation during RALP. During dissection at the level of the vesicoprostate junction, if the bladder neck is preserved, this can be directly anastomosed to the urethra without need for reconstruction. 2021 Previous studies reported a high rate of early continence recovery after bladder neck preservation during radical prostatectomy. Stolzenburg, et al.22 found that significantly improved continence was observed in a bladder neck preservation group compared with a no-preservation group at 3 months after laparoscopic radical prostatectomy. Lowe reported that bladder neck preservation does not produce an improved rate of postoperative incontinence, although it can be expected to shorten the interval of incontinence.23 In this respect, when the median lobe protrudes into the bladder, a higher grade of protrusion would lead to a higher chance to surgical damage at the smooth muscular internal sphincter during bladder neck dissection than non-IPP or a lower grade of IPP. In considering the pentafecta,24 we suggest that both IPP and the grade of IPP should be considered.
BMI and prostate volume may both be predictors of postoperative continence. Previous studies suggested BMI or prostate volume as an independent predictor of postoperative continence. In our patients, we measured preoperative variables including BMI and prostate volume using TRUS and MRI. We also routinely performed bladder neck reconstruction if the bladder neck was opened more than we expected.
Interestingly, we found a statistically significant difference between IPP and non-IPP patients. However, the NS group did not represent an independent significant factor on multivariate analysis. This finding might be related to the non-NS technique used. A higher grade of IPP might have favored more surgical damage at the level of the internal sphincter during bladder neck dissection.
If the patient had high-grade IPP (or significantly protruded median lobe), we occasionally found that the bladder neck could be preserved. In such cases, we performed bidirectional bladder neck reconstruction using V-loc sutures. In our opinion, priority should be given to preserving the bladder neck; however, it is also important to ensure that the bladder neck is smaller than the usual size.
We often experienced difficulties during bladder neck dissection in patients who underwent transurethral resection or incision of the prostate. However, in our opinion, the most difficult cases were patients who underwent holmium laser enucleation of the prostate. As they did not have a bladder neck junction, there was no landmark during bladder neck dissection. In these cases, we recommend that lateral dissection be performed as a first step and medial side dissection as a second step.
We recognize that the present study had several limitations. First, this was a retrospective analysis of a prospectively maintained database. Second, an objective assessment of baseline continence status was not performed. Finally, only pad usage was regarded as a proxy for the assessment of postoperative continence status; therefore, no validated questionnaire, such as the Expanded Prostate Cancer Index Composite questionnaire25 was used.
In conclusion, our findings suggest that IPP is correlated with the likelihood of urinary continence and with the time of recovery of urinary continence after RALP. Moreover, the grade of IPP seems to be a significant independent predictor of urinary incontinence after RALP. These findings can aid urologists performing RALP in proper surgical planning and patient counseling.






 XML Download
XML Download